


Abstract
Heightened awareness and concern regarding the large number of mentally ill misdemeanants in jails has led to a search for alternatives to jail and to the development nationwide of jail diversion programs for offenders with mental illness. Two such mechanisms—diversion to civil commitment and the use of mental health courts—are briefly reviewed. In Oregon, however, a rather unique mechanism is used to defer mentally ill misdemeanants (in addition to felons) from the criminal justice system: the insanity defense, with subsequent placement of the individual under Psychiatric Security Review Board jurisdiction. Statistics regarding such use from 1978 to 2001 are provided. The authors compare and contrast this jail alternative with both mental health courts and diversion to civil commitment, and discuss questions related to the feasibility of larger‐scale use of this mechanism.
An increasing number of individuals with mental illness are populating jails and prisons nationwide.1,2 It is estimated that more than 16 percent of jail inmates have a mental illness and that nearly 2 million new jail admissions a year include people with mental illness.3 A 154 percent increase in the proportion of mentally ill persons in jail was found between 1980 and 1992.2 This trend is of special concern for those mentally ill individuals placed in jail for minor offenses, a process frequently referred to as criminalization of the mentally ill.4 While the causes of this trend are complex and multifactorial, frequently cited factors include deinstitutionalization, more rigid commitment criteria, inadequate community resources, and the attitudes of police officers and society.5
The negative repercussions of this phenomenon are clear from several perspectives. Most obviously, from the standpoint of the inmate with mental illness, the stress and stigma of arrest and incarceration must be endured, with possible resultant exacerbation of mental illness symptomatology. While incarcerated, such individuals are vulnerable to manipulation, intimidation, and assault by other inmates.5 Mental health treatment while in jail is frequently suboptimal, especially when compared with the therapeutic milieu of a hospital or the array of services available in a community setting. Individuals with mental illness are also likely to be incarcerated for a longer period than those without mental illness.2 In addition, from a societal perspective, the arrest, booking, and incarceration of such individuals divert attention and resources from more serious offenders and do less to prevent recidivism than would properly addressing and treating their mental illnesses.5
From the perspective of the courts and the criminal justice system, mentally ill misdemeanants place additional strain on an already overburdened and overpopulated criminal justice system. The courts find themselves applying laws and concepts such as punishment and deterrence in a way that makes little sense for someone whose crime resulted, in many cases, from mental illness. Corrections staff are burdened when incarcerated mentally ill individuals are unable to follow instructions or display erratic, self‐destructive, or bizarre behavior. Such behavior and resultant vulnerability can necessitate housing in a single cell, at a time when jails are vastly overcrowded.
Increased awareness and concern regarding the large number of mentally ill offenders in jail has led to a search for alternatives to jail and development of jail diversion programs. In the current literature, jail diversion refers to specific programs that screen detainees for the presence of mental illness and employ mental health professionals to evaluate detainees and work with prosecutors, defense attorneys, community‐based mental health providers, and the courts to develop community‐based mental health dispositions.1 However, throughout the remainder of this article, the term “diversion” is used in the more generic sense—that is, a rerouting of mentally ill misdemeanants away from, or as an alternative to, incarceration. Using this more generic definition of diversion, we focus on the use of the insanity defense as a possible diversion mechanism for certain mentally ill misdemeanants. Two other commonly described diversion approaches, civil commitment and the use of mental health courts, are briefly reviewed.
Civil Commitment
Historically, pursuing civil commitment has been an option when mentally ill individuals are arrested and charged with minor crimes. When civil commitment occurs, the criminal charge is typically dropped, and the individual is transferred to the mental health system. However, in recent years, civil commitment has become more difficult to achieve for several reasons, including changes in commitment criteria and changes in the mental health system. Beginning in the late 1960s and early 1970s, civil commitment criteria nationwide became more stringent. The substantive criteria for commitment changed from general criteria that involved the concepts of mental illness and need for treatment, to more specific criteria that embodied either dangerousness or grave disability (the incapacity to care for oneself).4 The duration of commitment changed from indeterminant to determinant lengths of time, and an enhanced focus on ensuring due process guarantees went into effect.4 For example, in Oregon in 1973, the length of commitment was limited to not more than 180 days; the burden of proof was increased to “beyond a reasonable doubt” (although subsequently decreased to “clear and convincing evidence” in 1979); the right to legal counsel for indigent persons was codified; and the establishment of precommitment investigations took place.6 Many of these changes were needed to correct past abuses; but, not surprisingly, on a national level the changes in civil commitment criteria resulted in fewer as well as shorter commitments.4
The reduction in availability of inpatient beds in state psychiatric facilities is a major problem in Oregon and elsewhere. Because the demand for these beds now exceeds supply, they are necessarily utilized to treat only the most severely ill. For example, a 1998 study in Oregon tracked a cohort of patients with schizophrenia or bipolar disorder during two periods, 1981 to 1984 versus 1991 to 1994, and found a dramatic shift in hospitalization practices.7 From 1981 to 1984, all 1,067 hospitalizations of civilly committed individuals identified in the study occurred in one of Oregon's three state hospitals. By 1991 to 1994, however, only 39 percent of their hospitalizations were in the state hospital, while 21 percent were in community hospitals and 40 percent were in nonhospital facilities.7 While many committed individuals may not need a long‐term state hospitalization, the pressure to avoid state hospitalization due to limited availability of beds can create a less‐than‐ideal situation in which the lack of beds negatively affects the use of civil commitment statutes, both for the general psychiatric population and particularly for those mentally ill individuals who are in jails awaiting trial for minor crimes.
Nonetheless, even with the changes in criteria and the decreased availability of state hospital beds, civil commitment remains a viable, although less attractive, option for diverting mentally ill misdemeanants from jails to the mental health system.
Mental Health Courts
Mental health courts are an increasingly common approach for the diversion primarily of mentally ill misdemeanants. There are now approximately 30 such courts nationwide. These are specialty courts or dockets that handle only defendants with mental illness. Most (with a few exceptions) restrict the docket to nonviolent crimes, and all attempt to obtain quick access to community treatment services as an alternative to incarceration.8 To break the cycle of worsening mental illness and resultant criminal behavior, mental health courts strive to provide effective treatment options instead of the usual criminal sanctions for offenders with mental illness.8
There are, however, significant differences among these various courts. They vary in types of offenses covered, with approximately half limiting eligibility to defendants with misdemeanor charges and half accepting people charged with felonies, at least under certain circumstances.5 Approximately half the courts require a plea of guilty or no contest as a condition of participation, and some utilize a preadjudication model such that charges are suspended while the individual participates in treatment.5 Approximately one‐third of mental health courts allow for dismissal of charges or expunging of guilt after successful completion of treatment.5 Additional differences between currently operating mental health courts include the ability of the defendant to withdraw from the mental health court program without prejudice, as well as the scope and length of judicial supervision. While the court maintains jurisdiction over the defendant during the time the person receives services, many courts lack written procedures and some do not specify length of supervision.5 However, several courts do specify jurisdictional limits, which typically last one to two years.5 Sanctions for noncompliance vary significantly, and few studies examining outcomes of different sanctions have been undertaken.8 Sanctions currently in use include more frequent court appearances, increased judicial persuasion, lectures, jail time, and dismissal from the program.8
The Insanity Defense and Misdemeanants
Use of the insanity defense and subsequent commitment of insanity acquittees has not traditionally been thought of as a method for the diversion of misdemeanants from jails. One major reason this approach has not been used in this population of offenders is that in many jurisdictions an acquittal on the grounds of insanity results in commitment for an indefinite time that potentially far exceeds the period of incarceration for a guilty verdict. Thus, this defense has traditionally been raised primarily by individuals facing more serious felony charges that could carry long prison sentences. Release criteria for insanity acquittees typically involve a finding of restoration of sanity, and/or lack of dangerousness, since court decisions such as Foucha v. Louisiana9 have declared it a violation of a defendant's right to due process to be incarcerated indefinitely without continued findings of mental illness and dangerousness. Given that time to restoration of sanity and/or lack of dangerousness may bear little resemblance to the time that has been served under the initial criminal charge, there is great reluctance to use the insanity defense for other than the more serious felony charges.
The situation in Oregon, however, is different and unique. Since 1978, insanity acquittees who are dangerous and mentally ill have been placed under the jurisdiction of the Psychiatric Security Review Board (PSRB). The standard for the insanity defense in Oregon states: A person is guilty except for insanity if, as a result of mental disease or defect at the time of engaging in criminal conduct, the person lacks substantial capacity either to appreciate the criminality of the conduct or to conform the conduct to the requirements of the law [Ref. 10, § 295, ¶ 1].
After the determination that the individual is “guilty except for insanity”: If the court finds that the person would have been guilty of a felony, or of a misdemeanor during a criminal episode in the course of which the person caused physical injury or risk of physical injury to another, and if the court finds by preponderance of the evidence that the person is affected by mental disease or defect and presents a substantial danger to others requiring commitment to a state mental hospital…or conditional release, the court shall order the person placed under the jurisdiction of the Psychiatric Security Review Board for care and treatment. The period of jurisdiction shall be equal to the maximum sentence provided by statute for the crime for which the person was found guilty except for insanity [Ref. 11, § 327, ¶ 1].
While under PSRB jurisdiction, insanity acquittees may receive treatment on an inpatient and/or outpatient basis (an individual may be conditionally released, with the possibility of revocation and rehospitalization).12 The fact that there is a jurisdictional limit to the commitment to the PSRB makes this a viable option for those dangerous mentally ill individuals charged with misdemeanors, as misdemeanor insanity acquittees will not be under PSRB jurisdiction for more than one year and may spend only a fraction of that time in the hospital.
In the event that an individual reaches the end of his or her PSRB jurisdiction and is still considered mentally ill and dangerous, civil commitment may then be pursued at a separate proceeding.
Figure 1 illustrates the number of misdemeanants committed to PSRB jurisdiction from 1978 to 2001. From 1978 to 2001, an average of 73 individuals per year was placed under PSRB jurisdiction. Of these, misdemeanants accounted for an average of 17 commitments per year, or 23 percent of the total new commitments. A peak number of 31 misdemeanants under PSRB jurisdiction occurred in 1979, while in 1996 a nadir of 7 misdemeanants was found under the Board's jurisdiction. Since 1996, there has been significant fluctuation in the number of misdemeanants under PSRB jurisdiction. In 2001, the most recent year for which data have been compiled, 18 misdemeanants were under PSRB jurisdiction.
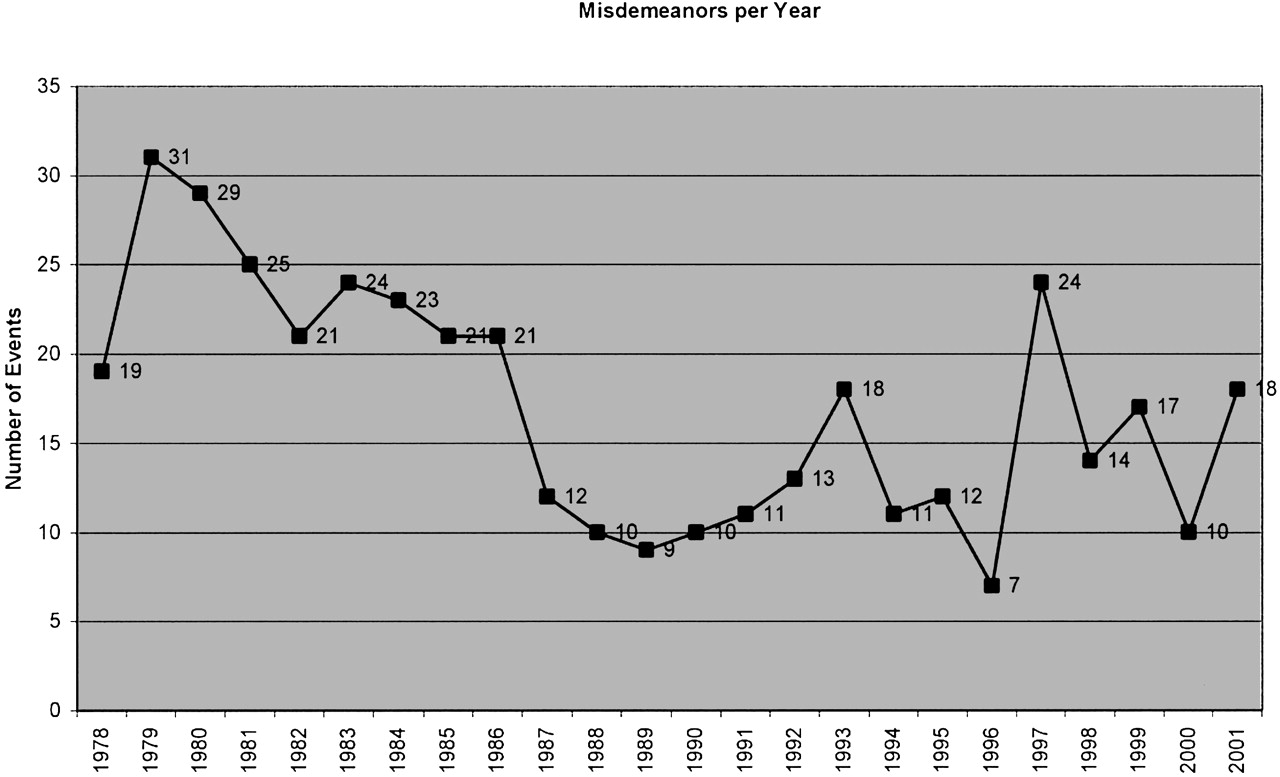
Number of misdemeanants under PSRB jurisdiction from 1978 to 2001.
Discussion
The use of the insanity defense for misdemeanants and subsequent placement of these insanity acquittees under PSRB jurisdiction has been operating in Oregon since 1978. This strategy could be considered, from one point of view, to be a unique jail diversion program. While the use of the insanity defense for misdemeanants has never involved large numbers of jail detainees and has fluctuated in frequency, its use nonetheless remains a viable diversion mechanism, according to the more broad definition of diversion provided herein. The fact that it has been used at all for misdemeanor charges primarily reflects the jurisdictional limit to PSRB commitment. Thus, a mentally ill defendant is not placed in the difficult position of having to choose between a shorter length of incarceration or treatment of mental illness. Given the magnitude and importance of the problem of mentally ill misdemeanants in jails nationwide, this use of the insanity defense is important to explore.
How does the use of the insanity defense as a diversion strategy compare with civil commitment and mental health courts? Both civil commitment and the insanity defense are statutes that are applicable across an entire state, whereas mental health courts represent local jurisdictions, usually a county. This is an important distinction. Having a set of laws affect an entire statewide population has much greater reach than what one or several counties can accomplish. Further, statewide statutes also bring the state mental health authority into the picture and allow use of resources in one county to be brought to bear on problems in another county. For example, if the best group home for a particular insanity acquittee is located in another county in Oregon, the PSRB can authorize placement of the person in the situation that best fits his or her needs. Mental health courts, however, rely on local arrangements between the courts and community mental health resources to meet treatment needs, and these resources may be quite variable and perhaps lacking in particular areas of a state.
Length of jurisdiction is another important variable in comparing these different diversion programs. Both civil commitment and the Oregon insanity defense have specific lengths of jurisdiction for those committed under each statute. Civil commitment in Oregon is for “up to 180 days,” whereas the insanity “sentence” is fixed at the time of commitment by the trial judge and is based on the “crime” charged. For those in mental health courts, time under the courts' jurisdiction may be discretionary and thus quite variable. Typically, jurisdiction in such courts lasts one to two years.5
In general terms, civil commitment, whether to inpatient or outpatient programs, appears to be the program that offers the best possibilities for true diversion of many mentally ill misdemeanants out of the criminal justice system and into the mental health system. Civilly committed individuals are spared the additional stigma of criminal justice sanctions, whether it be through a mental health court or a successful insanity defense. Unfortunately, as mentioned earlier in the article, changes in civil commitment laws themselves, which led to more stringent commitment criteria and limited treatment resources, are often cited as one of the causes of criminalization of the mentally ill. The question is whether part of the problem can still be a major part of the solution. Time will tell, but we should always keep in mind that civil commitment can be reformed and, at the same time, important rights preserved, returning civil commitment to a central place in diversion.
The insanity defense as used in Oregon is unique. The jurisdictional limit creates a closer tie between the traditional punishment for the crime and the recognition that instead of punishment, mentally ill individuals need treatment for their illnesses. In addition, once the trial court judge places the individual under PSRB jurisdiction, the person is no longer supervised by the court but instead by PSRB board members, which include a psychologist, a psychiatrist, a lawyer, a person experienced in parole and probation, and a lay person. In order for other states to use this mechanism they would have to adopt the limits to the PSRB jurisdiction that exist in Oregon. Accepting the PSRB model would require major readjustments in thinking about the insanity defense vis‐à‐vis criteria for continued commitment versus release of an insanity acquittee who remains symptomatic. Were other states to adopt the PSRB model, use of the insanity defense may be a more ideal method to deal with misdemeanants when crime, dangerousness, and mental illness are combined. The insanity defense with a jurisdictional limit affords both a clearer approach to crime and to diversion.
For the insanity defense to make an impact on the problem of criminalization of the mentally ill, more work is needed in Oregon to understand why it is not used on a larger scale. There are several anecdotal reasons for both the absolute number of individuals using this defense and the fluctuation from year to year. We have been told that the yearly fluctuations reflect periodic changes in the criminal justice system. When jails are crowded, misdemeanants are released early, and even a year of supervision may be a much longer period of supervision than time served following a conviction. Thus, attorneys familiar with the PSRB may feel it is in their clients' best interests to avoid this defense if they think their clients would serve less time in jail.
Ease of use of this option also probably influences the readiness and frequency with which attorneys turn to it. At a minimum, a forensic evaluation must be obtained to determine whether the individual meets the Oregon standard for the defense. Frequently, individuals later adjudicated under the PSRB initially also had to undergo competency‐to‐stand‐trial evaluations and treatment to restore competency, often for months. This makes it less likely that the insanity defense will be pursued when a reasonable plea bargain is offered, for example, or a civil commitment could be obtained.
Another potential explanation for fluctuation from year to year is awareness or familiarity with the PSRB on the part of defense attorneys. In addition to variances in understanding the PSRB, defense attorneys also have different levels of knowledge regarding mental illness as a whole and a variable ability to recognize the relationship between mental illness and, for example, misdemeanant behavior.
In addition, the PSRB can act only in behalf of individuals who have “caused physical injury or risk of physical injury to another”11 and who remain dangerous. This distinction is thought to be important in balancing civil rights, safety, and ideal mental health treatment. For misdemeanants in particular, however, it obviously limits the number of individuals for whom the PSRB can act, as many misdemeanants do not meet these criteria. The insanity defense, as an affirmative defense, should also continue to be raised on a voluntary basis, and a given individual may not choose, or be forced, to pursue this option.
There are, therefore, a number of areas for research regarding the feasibility of increased use of the PSRB model for misdemeanants. This work would be important in helping us understand if the model can be used entirely or in part as a practical and larger scale solution to the ever‐growing problem of the criminalization of the mentally ill.
Mental health courts are the newest programs of interest in this difficult area. The law regarding such courts is evolving. These courts function differently in different states and, to date, there appears to be just one court in a given state, although their jurisdictions, as noted, appear limited to county lines. Much more development must take place before this type of model is actually the method of choice for diversion.
It may very well be that the planners of programs in the future will recognize an important place for each of the three mechanisms described: civil commitment for less serious misdemeanor charges, the insanity defense for dangerous mentally ill misdemeanants, and mental health courts in larger counties with adequate resources in a state where specialized courts make the most sense.
Acknowledgments
The authors wish to thank Dr. Douglas Bigelow and Mr. Anton Cox for help with the data presented in the article.
- American Academy of Psychiatry and the Law









{kind=link}