


Abstract
Self-injurious behavior (SIB) is a common, disruptive, and costly occurrence in U.S. prisons. In this study, we describe the use of clozapine to treat 10 offenders with chronic, repetitive self-injury refractory to other medications and behavioral therapies. The primary diagnosis for all 10 offenders was a personality disorder. Eight of the 10 inmates allowed weekly blood draws and took medication regularly (approximately 95% adherence), whereas two inmates discontinued treatment within the first two weeks. For these eight patients, we compared the number of in-house urgent care visits and outside emergency room visits related to SIB for the six-month periods before and after treatment with clozapine. After initiation of clozapine treatment, there were 66 fewer urgent care visits (94 versus 28) and 26 fewer emergency room visits (37 versus 11), a 70 percent reduction in each. As a secondary outcome, we assessed disciplinary infractions. There were 132 fewer infractions (197 versus 65), a 67 percent reduction. The median dose of clozapine used was 125 mg/day, substantially lower than doses typically used to treat schizophrenia. Clozapine appears to be a feasible and effective treatment for some patients with chronic, repetitive SIB for whom other treatments have failed.
Self-injurious behavior (SIB) is a prevalent, costly, and disruptive problem in prison populations.1,–,6 SIB is defined as “the deliberate destruction or alteration of body tissue without conscious suicidal intent.”7 In forensic settings, this can manifest as cutting, head banging, scratching, burning, hitting, biting, amputation, foreign body insertion/ingestion, overdose, enucleation, smearing feces into wounds/orifices, and opening old wounds.
Prevalence estimates of SIB among inmates vary widely. In a recent review of SIB in England and Wales, 5 to 6 percent of male prisoners and 20 to 24 percent of female prisoners engaged in SIB each year over a five-year period.6 A national survey of prison mental health directors in the United States found that less than two percent of inmates engaged in SIB each year, but that 85 percent of prison systems observed SIB on a weekly basis.3 Repetition of SIB among inmates is common, and a substantial clustering effect of SIB in prisoners, both in time and location, has been noted.6 The cost of care for individuals with repeated episodes of SIB is markedly higher than for other offenders, primarily due to frequent emergency room and urgent care visits.8 Repetitive self-injury also takes a toll on prison staff in terms of one-to-one monitoring, transport to medical facilities, and burnout.
SIB in prisons has been associated with risk factors including younger age, white race, female sex, prior mental health diagnoses, history of violence, prior trauma, prior substance use history, developmental or intellectual disabilities, and placement in restrictive housing.2,5,6,9 Restrictive housing, also known as segregation or solitary confinement, involves confining inmates to a cell for up to 23 hours per day, with one hour out for solitary exercise or hygiene. SIB in offenders is a risk factor for both future suicide and violence toward others.6,10
Conventional management of SIB in prisons involves use of medications, seclusion, restraint, and behavioral therapies.3,11,12 To date, there is no FDA-approved medication indicated for the treatment of chronic, severe SIB, nor is there any medication approved for borderline personality disorder (BPD) or antisocial personality disorder (ASPD), illnesses that increase the risk of such behaviors, particularly in the forensic setting. Two recent reviews show limited effectiveness of pharmacological management of SIB in adults in non-correctional settings; however, these reviews relied exclusively on randomized trials and did not include clozapine.13,14
Clozapine is a second-generation antipsychotic medication with demonstrated effectiveness for treatment-refractory schizophrenia and reduction in risk of recurrent suicidal behavior in individuals with schizophrenia or schizoaffective disorder.15,–,17 Numerous reports document clozapine's benefits in decreasing SIB and aggression in both psychotic and non-psychotic populations.18,–,22 Despite its superiority to other antipsychotics, clozapine remains underutilized in the United States for a variety of reasons, primarily its requirement for hematological monitoring. In 2016, a workgroup of the National Association of State Mental Health Program Directors issued a white paper addressing the underutilization of clozapine.23 The paper noted that “accumulating evidence supports clozapine's utility for a variety of other disorders and conditions such as treatment of hostility and aggression…and borderline personality disorder” (Ref. 23, p 7). The authors also recommended expanding clozapine's use in forensic facilities, given the increasing number of incarcerated individuals with mental illness.
There are few published reports of clozapine's use in prisons and jails, and most studies have focused on patients with schizophrenia.24,–,27 Brown et al. have described clozapine's use in a cohort of non-schizophrenic violent men with ASPD, reporting reductions in impulsivity and aggression after a median of 14 weeks of treatment.26 However, much of the aggression in this group did not involve physical assaults against others. Mela and Depiang analyzed post-release patients with a psychotic disorder on clozapine and other antipsychotics and found a significantly longer time to first offense and more crime-free time in the community in the clozapine group.27 To our knowledge, there are no published articles examining the use of clozapine for chronic SIB in a prison population.
This study had two primary objectives. We sought to examine the feasibility of prescribing clozapine to male offenders in a restrictive housing setting who exhibit chronic, severe SIB, for whom multiple prior pharmacological and psychosocial therapies had failed. If feasible, we then attempted to determine whether this intervention was effective in reducing the number of episodes of SIB. As a secondary measure, we sought to determine whether there was any reduction in disciplinary infractions. We hypothesized that there would be a reduction in both SIB and infractions after treatment with clozapine for at least some patients.
Methods
Study Site
North Carolina Central Prison houses 752 inmates and operates a hospital with 216 mental health beds and 120 medical/surgical beds. All patients in this study were male offenders on a 24-bed restrictive housing mental health inpatient unit at North Carolina Central Prison Hospital. The unit is staffed by a psychiatrist, nurses, behavioral health technicians, masters-level psychologists, and correctional officers. In the hospital, inmates are confined to their cells except for therapeutic groups, recreation, or to shower. The hospital's restrictive housing unit allows up to two hours of time out of one's cell for these activities, while the non-hospital restrictive housing units only allow up to one hour and do not offer group therapy. Access to personal property is more restricted in the hospital unit for safety purposes. Groups are led by psychology staff and focus on a variety of mental health and substance use topics, particularly the development of safe and positive coping skills. All inmates, whether prescribed clozapine or not, were offered group therapy three times per week based on principles of cognitive behavioral therapy.
In 2016, the North Carolina Department of Public Safety (DPS) sought to establish a policy on the use of clozapine in DPS facilities that was consistent with the standard of care in the community. The policy approved by DPS in June 2016 was modeled after one used at a North Carolina state psychiatric hospital. It serves as a guideline for the prescribing, monitoring, and dispensing of clozapine, both for FDA-approved indications and for patients with other treatment-refractory mental illnesses. The policy outlined roles for psychiatry, medicine, pharmacy, nursing, and psychology services. Staff received training to familiarize themselves with the policy, and an online module to train nurses in clozapine's indications and potential side effects was developed.
Subject Selection
Electronic health records were reviewed for 13 patients without a primary psychotic disorder who were offered clozapine treatment for chronic, severe SIB beginning in July 2016. To receive clozapine, patients were required to be competent to make health care decisions and to be capable of providing informed consent for clozapine treatment. All had a DSM-5 diagnosis of ASPD or BPD made by prison hospital psychiatrists on the basis of all available clinical and historical information, and all had failed other pharmacological and psychosocial therapies, including two antipsychotic trials prior to clozapine initiation. In addition, treatment resistance was defined as having had three separate incidents of SIB in the prior six months. Inmates who were prescribed clozapine but did not have a history of chronic SIB and those who had a primary diagnosis of schizophrenia, schizoaffective disorder, or bipolar disorder were excluded from this analysis. All patients had been prescribed other psychotropic medications prior to clozapine initiation. The DPS guidelines for clozapine treatment encourage tapering off antipsychotics after clozapine initiation. Mood stabilizers are also tapered off and discontinued unless the indication for treatment is a seizure disorder. Patients taking carbamazepine for epilepsy are transitioned to levetiracetam due to carbamazepine's interactions with clozapine. Patients typically can continue antidepressants during treatment with clozapine. Side effects were monitored by clinical staff, although no standardized assessment tool was utilized. Patients taking clozapine were offered the same behavioral health therapies as patients who were not taking clozapine.
To assess the feasibility of prescribing clozapine for repetitive self-injury, we analyzed how many patients agreed to take clozapine once offered, the percentage of doses refused, and the number of blood draws (for routine clozapine monitoring) refused. Blood draws were counted as refused if they resulted in an interruption in treatment.
The primary outcome measure was the change in the number of episodes of severe SIB as measured by visits to an onsite urgent care clinic or visits to outside emergency rooms for the six months prior to clozapine treatment and the six months after treatment. The post-treatment period began the day after clozapine initiation. Visits were counted for new episodes of SIB but not for follow-up visits related to medical complications of prior SIB. In addition, three of eight patients had data available for the previous 12 months. Electronic records were reviewed, and the data were analyzed independently by the North Carolina DPS Quality Improvement team. A secondary analysis looked at the number of infractions issued by custody officers before and after clozapine treatment. Only infractions that were reviewed and confirmed (i.e., “guilty” infractions) were counted. In addition, we determined the direct costs incurred for medical services provided at outside hospitals.
This study was approved by the Office of Human Research Ethics at the University of North Carolina at Chapel Hill (IRB # 16-2759).
Results
Thirteen patients met criteria. Ten patients consented to treatment and were started on the medication. Two patients discontinued treatment within two weeks, reporting that they had changed their minds but denying any specific side effects. Of the 10 patients consenting to treatment, seven were diagnosed with ASPD and three with BPD. Six patients had a history of substance use disorder, and three had a diagnosis of seizure disorder. No patients had a diagnosis of intellectual developmental disorder. Five patients were African American, four were Caucasian, and one was Native American. The median age was 28 years (range 24–44 years). No patients had a comorbid psychotic disorder, although all had previously tried at least two other antipsychotics for SIB with no benefits. Four offenders had a past affiliation with a gang, but none had known active involvement or strong association with a gang during the study period.
In the three years preceding initiation of clozapine, inmates who consented to treatment had spent a median of 27 months (range 6–36 months) in restrictive housing. All patients who consented to treatment were in restrictive housing for the six months preceding initiation of clozapine. The median number of days spent in a restrictive housing hospital setting for the six months before treatment was 120 days, whereas this number was 155 days after treatment. One patient's remaining time in restrictive housing expired during the treatment period.
Eight patients took clozapine for at least six months from initiation. Of these, all adhered to weekly blood draws for routine monitoring. The medication adherence rate (i.e., the number of doses accepted divided by the number of doses offered) was 95 percent. The median dose utilized was 125 mg/day (range 75–225 mg/day).
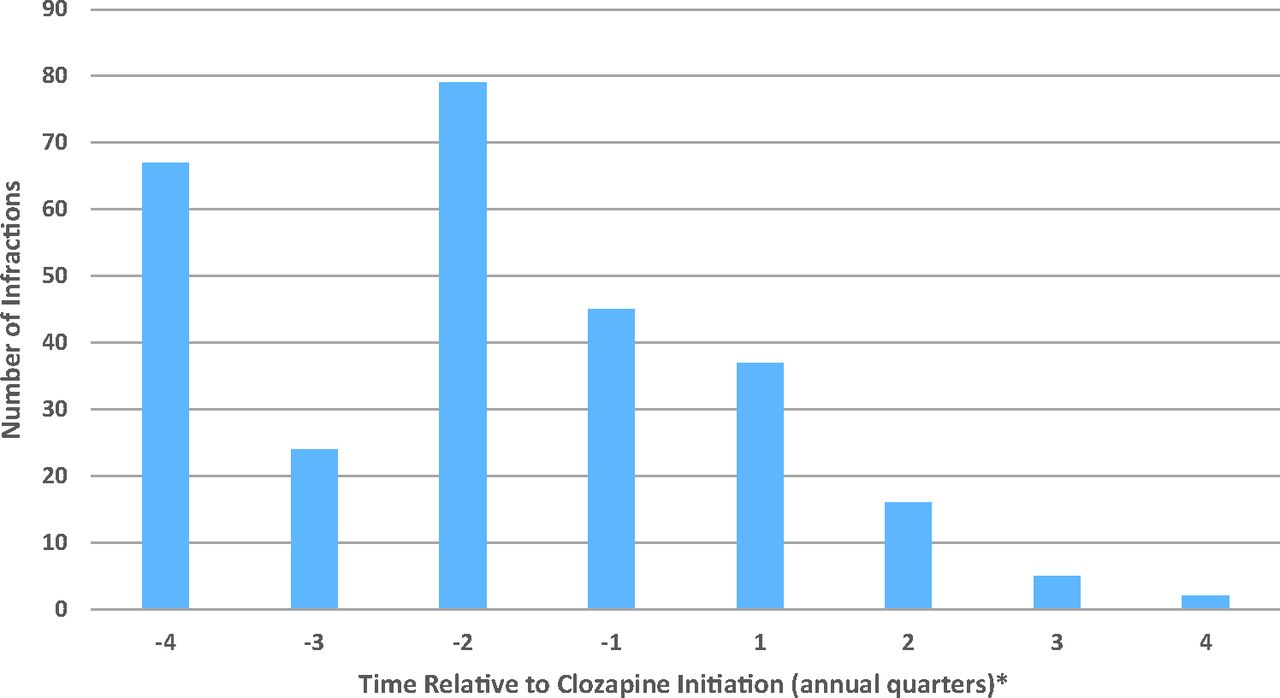
Patients' (n = 8) urgent care visits, emergency room visits, and infractions were aggregated for the six-month period before clozapine treatment and compared with the six-month period after initiation of clozapine. Patient-level data are presented in Table 1. There was a 70.2 percent decrease in onsite urgent care visits (94 versus 28), a 70.3 percent decrease in outside emergency room visits (37 versus 11), and a 67.0 percent decrease in total infractions (197 versus 65) for the time periods assessed. A subset of infractions, assaults on custody staff, was reduced by 46.2 percent (39 versus 21). Almost all SIB that occurred after initiation of clozapine occurred in the first three months of treatment. Total infractions were broken down by quarter relative to clozapine initiation and results are presented in Fig. 1.
Medical Visits Related to Self-injurious Behavior and Infractions Among Clozapine-Treated Offenders

Number of disciplinary infractions for patients (n = 8) by quarter relative to clozapine initiation (6 months pre/posttreatment). *Quarter 1 begins the day following clozapine initiation.
Of the eight patients who took clozapine for at least six months, three had also reached twelve months of consecutive treatment (the other five continued on clozapine but had not yet reached twelve months). For these three patients, the sum of infractions decreased from 215 in the 12 months prior to clozapine treatment to 60 in the 12 months of treatment (72.0% decrease). Included in this number were assaults on custody staff, which decreased from 50 to 16 (68.0% reduction) over the same time period. Most post-treatment infractions occurred early in the treatment course; in months 6 to 12 of treatment, these three patients incurred only seven additional infractions, only one of which was an assault charge. There were no episodes of SIB for these patients in months 6 to 12 of treatment. Twelve-month infraction data for these patients are presented in Fig. 2.

Number of disciplinary infractions for patients (n = 3) by quarter relative to clozapine initiation (12 months pre/posttreatment). *Quarter 1 begins the day following clozapine initiation.
Costs of outside hospital visits, defined as only directly paid charges from hospitals for new episodes of SIB, were analyzed before and after clozapine treatment. Bills to the prison system for visits related to SIB were approximately $200,000 lower during the six months following initiation of clozapine treatment compared with the six months prior to treatment.
Discussion
This study demonstrates that clozapine use for chronic and severe SIB initiated in a restrictive housing setting is both feasible and effective for some inmates. Of 13 inmates who were determined to be eligible for a clozapine trial, 8 (61.5%) agreed and cooperated with treatment for at least six consecutive months. In this small sample of repetitive self-injurious patients, clozapine was markedly effective in reducing the number of medical visits needed for SIB. Furthermore, infractions (including assaults on custody staff) also markedly decreased after treatment with clozapine.
There were initial questions about whether inmates would agree to take clozapine consistently and adhere to required blood monitoring, or whether they would use these blood draws as a means to possibly extort or manipulate the clinical team for other ends. The results overwhelmingly indicate that patients remained adherent to treatment. Indeed, the medication adherence rate of 95 percent exceeds the often-cited standard of 80 percent used in clinical trials to measure overall treatment adherence.28
In this study, clozapine's effect on SIB and infractions was striking, particularly the consistency of the results in both areas across all subjects. The effect persisted (and in fact was more profound) after six months of treatment with a continued absence of SIB and lessening of infractions. The marked decrease in SIB is consistent with prior studies done in non-correctional hospital settings.21,22 Prior studies have also shown clozapine to be cost-effective when compared with other antipsychotics in the general population.29 In this cohort, over $200,000 in outside hospital emergency room charges was saved. This figure does not include ancillary costs, such as paying correctional officers to transport and monitor patients during their visits to outside emergency rooms, follow-up emergent or scheduled treatments related to prior SIB, and costs incurred onsite at the prison. In comparison, the cost of clozapine treatment was estimated to be substantially less than the amount saved in emergency room bills, given clozapine's availability as a generic medication and the relatively inexpensive cost of an electrocardiogram and blood monitoring.
Clozapine's effect on aggression against others, including a 46 percent decrease in assaults on custody staff, is noteworthy and consistent with previously published data in patients with schizophrenia.18,19 Little data exist on the use of clozapine for violent patients with ASPD or BPD. One case series on clozapine in seven men with ASPD found decreases in aggression; however, there was only one recorded physical assault in this group prior to treatment, and most episodes of aggression were either verbal or directed toward property.26 Another study found self-harm to be a risk factor for violent crime and suggested that self-harm “could be viewed as an early behavioral marker of difficulties with emotional and behavioral regulation that…may increase the risk of committing violent crimes” (Ref. 10, p 620). To our knowledge, only one study has addressed clozapine's effect on overall infractions, noting a decrease in offenses by patients treated with clozapine versus those treated with other antipsychotics.24 However, that study analyzed patients with psychotic disorders, 40 percent of whom had no pretreatment offenses. Our analysis suggests that clozapine could potentially be effective in a population of personality-disordered inmates with impulse-control problems and a high number of pretreatment infractions.
Interestingly, the patients responded at relatively low doses (median 125 mg/day) compared with those typically required for treatment-resistant schizophrenia (FDA-approved up to 900 mg/day). The most common side effect reported was sialorrhea, and five patients were prescribed atropine ophthalmic solution sublingually to manage this with good effect. Two patients had a greater than seven percent gain in body weight. No other side effects were reported by more than one patient, and no patients discontinued clozapine due to side effects. Prior analyses of patients with schizophrenia found clozapine's anti-aggressive properties to be independent of its effect on psychosis and not secondary to sedation.18,19 Although not assessed using a standardized tool, the reduction in violent behaviors did not appear to be secondary to clozapine's sedating effect. Sedation was monitored clinically and, outside of the initial two weeks of treatment, was not reported nor observed for any of the eight patients who took clozapine for the six-month period. In addition, the majority of the dose was typically given at bedtime.
A key advantage of utilizing clozapine for the management of severe, repetitive SIB is that it can be adopted relatively easily by most correctional systems. Most prison systems already have the staffing and ancillary services (e.g., lab, pharmacy, nursing) in place that are needed to monitor clozapine, making this approach easily protocolized for use in different settings. Setting up a large behavioral-management program requires an ongoing training effort to be sure that all staff are consistent on an ongoing basis, and any such program would need to include both custody and nursing. This commitment may not be realistic in some prisons, given the amount of resources that would need to be devoted to this type of effort. However, use of clozapine may allow individual cognitive or dialectical behavioral therapy and other types of supportive efforts to be much more effective. Opportunities should be pursued to utilize behavioral training in conjunction with medication as the optimal way to maintain the gains produced in reduction in SIB and infractions.
Our results, while preliminary, support the use of clozapine for the treatment of chronic, repetitive SIB and aggression in some male inmates with treatment-refractory personality disorders who did not respond to prior treatment. Nevertheless, this study has several limitations. There was no control group. The sample size was relatively small, and the cohort was limited to male patients who had clozapine initiated in restrictive housing. There were potentially confounding variables, such as inmates' desire to remain in the inpatient hospital, the treatment setting not being uniform before and after treatment, and increased attention from providers, which may have favored clozapine treatment. In addition, no standardized assessment of sedation was obtained, nor were clozapine blood levels routinely measured to assess adherence; the contribution of psychosocial adjunctive therapy was not assessed. Future studies should explore clozapine's effects on SIB, aggression, and infractions in a larger cohort of inmates and across different sites.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2019 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}