Article Text

Abstract
Background Adolescent health problems are more prevalent in families with low socioeconomic position, but few studies have assessed the role of parental health in this association. This study examines the extent to which parental health problems, particularly those related to high-risk health behaviour, might explain the association between parental education and adolescent health problems due to violence, self-harm and substance use.
Methods We used longitudinal register data on a 20% representative sample of all families with children aged 0–14 years in 2000 in Finland with information on parental social background and parental and offspring health problems based on hospital discharge data. We estimated discrete-time survival models with the Karlson-Holm-Breen method on hospital admissions due to violence, self-harm and substance use among adolescents aged 13–19 years in 2001–2011 (n=145 404).
Results Hospital admissions were 2–3 times more common among offspring of basic educated parents than tertiary educated parents. Similar excess risks were observed among those with parental mental health problems and parental health problems due to violence, self-harm and substance use. The OR for offspring of basic educated parents was attenuated from OR 2.73 (95% CI 2.34 to 3.18) to OR 2.38 (2.04 to2.77) with adjustment for parental health problems, particularly those due to violence, self-harm and substance use. Having both low parental education and parental health problems showed simple cumulative effects.
Conclusions The excess risks of hospital admissions due to violence, self-harm and substance use among adolescents with lower educated parents are largely independent of severe parental health problems.
- adolescents cg
- education
- health behaviour
- lifecourse / childhood circumstances
- social and life-course epidemiology
Statistics from Altmetric.com
- adolescents cg
- education
- health behaviour
- lifecourse / childhood circumstances
- social and life-course epidemiology
Background
Although early youth has been suggested to be a life period of relative equalisation in health,1 numerous health outcomes, including injuries and poisonings, violence and self-harm, mental health problems, self-rated health and health behaviours, show clear associations with social background from childhood through adolescence to adulthood.2–7 Relatively little is still known on the role of parental health and health behaviours behind the higher occurrence of health problems among adolescents from socially disadvantaged families. Parental health may predict offspring health not only due to genetic liability,8 but also because parental health problems or engagement in high-risk health behaviours affect the psychological and social adjustment and functioning of children.9–12 Severe parental illness may entail considerable decreases in parental availability and affect parenting, inducing stress and increased responsibilities for offspring.9 13 Parental modelling may also induce parent–offspring similarities in health behaviours, particularly in hazardous substance use.14–16 As the less educated and less earning parents are more likely than better-off parents to have health problems and engage in high-risk health behaviours,17 18 parental health problems could explain some of the associations between parental social characteristics and offspring health.
A large literature on adverse childhood experiences has documented cumulative effects of exposure to multiple risk factors on various health outcomes and high-risk health behaviours in adolescence and adulthood.19–22 Going beyond the general finding that more adversities predict worse outcomes, some studies have also observed the highest risks among offspring with specific combinations of exposures such as childhood poverty and parental mental illness.23 According to a recent review on pathways between family socioeconomic status and adolescent psychosocial outcomes, numerous studies have identified family-level factors such as parental distress and depression as important mediators in the associations.24 Studies that focus on parental health problems remain nonetheless few, and evidence that extends beyond specific conditions such as parental depression is lacking.24 25
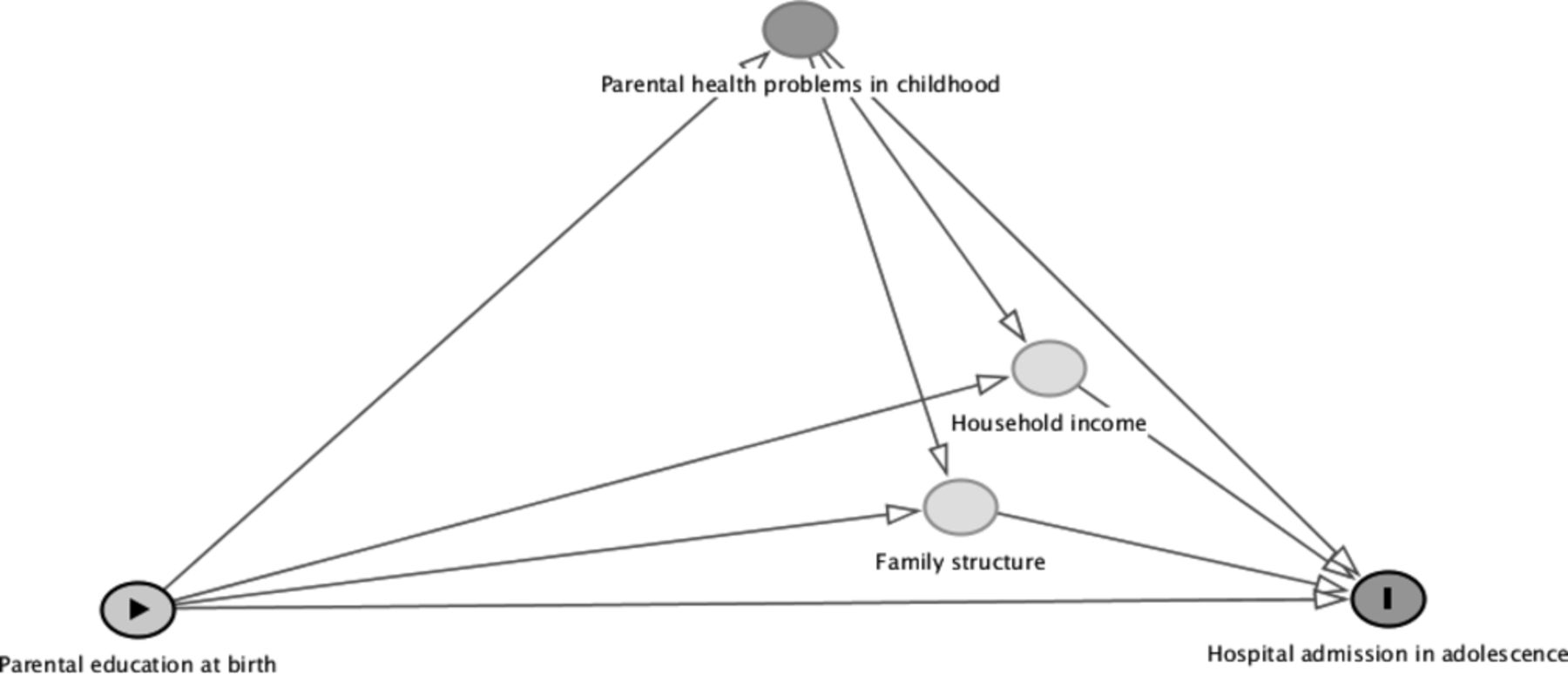
Adolescence is an important period for onset and establishment of health behaviours,26 and previous research has shown high-risk health behaviours and adversity-related hospital admissions in youth to predict later excess morbidity and mortality.27–30 In this prospective population-based cohort study, we examine the role of parental health problems in the association between parental education and a severe offspring health outcome that reflects high-risk health behaviour in adolescence: hospital admissions due to violence, self-harm and substance use. First, we focus on the potential mediating role of childhood exposure to severe parental health problems: we expect to find a strong gradient by parental education in adolescent hospital admissions and assess the extent to which parental health problems, particularly those due to high-risk health behaviours such as substance abuse, might explain the educational differentials. Second, prompted by previous evidence on multiple adverse childhood experiences, we examine potential aggravation of risk among adolescents with cumulative childhood disadvantage: we expect to find highest admission rates among adolescents with both low educated parents and childhood exposure to parental health problems. Although our focus lies on the role of parental health, we include in our analyses childhood family structure and household income that are presumed to act as pathways through which both parental education and parental health problems may influence offspring health (figure 1).

Diagram of the assumptions of this study on the causal relationships between parental education at birth, parental health problems during childhood (0–12 years) and adolescent (13–19 years) hospital admissions due to violence, self-harm and substance use.
Data and methods
Study population
The study is based on a 20% representative sample of all households with at least one child aged 0–14 years in the year 2000 in Finland. For all the children, their household members and their non-coresident biological parents, annual population census and employment data were linked with hospital discharge records using personal identification numbers. In this study, we included native-born children from birth cohorts 1987–1998 (n=148 298) who were 13–19 years of age during follow-up in 2001–2011. We excluded children with incomplete data between ages 0–12 (n=1106) and those with missing data on their biological mother and father (n=1788). The follow-up for the final sample of 145 404 adolescents started from the year of 13th birthday, and subjects were censored at first hospital admission, death, emigration, when reaching age 20 or at the end of 2011.
Study outcome: hospital admissions due to violence, self-harm and substance use at ages 13–19
Data on hospital admissions came from the Finnish Hospital Discharge Register that covers all institutions providing hospital care. The coding of diagnoses and external causes of injuries was based on the International Classification of Diseases (ICD-10). We included all care episodes of mental and behavioural disorders due to psychoactive substance use, poisoning by drugs, medicaments and alcohol, intentional self-harm and assaults (ICD-codes in online appendix A). There were 1619 first hospital admissions due to violence, self-harm or substance use in the data, of which 33.3% were due to substance use-related mental and behavioural disorders, 38.4% accidental poisonings, 18.3% intentional self-harm and 10.0% assaults. Self-harm and poisonings were more common among girls, and assaults and substance use-related mental and behavioural disorders among boys. We considered only first admissions as the number of individuals with multiple care episodes during the follow-up was small (n=147) and sensitivity analyses on single and multiple episodes produced highly similar findings (results not shown). The rates of hospital admission by age of occurrence ranged between 1.2 (per 1000) at age 13 and 3.0 (per 1000) at age 19.
Supplemental material
Parental education and parental health problems
Parental characteristics refer to the biological parents. Parental education, based on the highest completed degree by either parent, was measured at the child’s birth and classified into tertiary (≥13 years), secondary (11–12 years) and basic education (<10 years). Parental health problems were measured by hospital care episodes when the child was aged 0–12 years. We assessed separately hospital admissions due to (1) violence, self-harm and substance use (identical to the measurement of the study outcome, but also including substance use-related somatic diseases); (2) mental and behavioural disorders other than those included in the first category; and (3) somatic diseases excluding care episodes due to complications of medical and surgical care, pregnancy and childbirth, and those related to substance use (see online appendix A for ICD codes for categorisation of parental health problems). In the analyses, each category of health problems was included as a dichotomous variable indicating the presence/absence of parental hospital admission during childhood. One parent could thus contribute to estimates in more than one category although the diagnoses in each category were mutually exclusive.
Other family characteristics in childhood
Household income, based on the Tax Administration’s database, consists of wages, salaries, entrepreneurial income, pensions, unemployment benefits and some of the other social security benefits. Household income was divided by the weighted sum of household members according to the modified OECD equivalence scale and divided into annual quintiles. Family structure was based on the child’s living arrangements and classified into (1) intact two-parent family, (2) continuous single-parent family or one change in family structure and (3) multiple changes in family structure or unknown living arrangements at least once. Both household income and family structure were used as time-varying covariates until the age of 16. To ensure consistent measurement of childhood family characteristics, the covariates were fixed for the rest of the follow-up as home-leaving becomes increasingly common at ages 17–19.
Study analysis
We calculated hospital admission rates and used discrete-time survival models with 1-year time intervals and logit link to examine the associations between parental education at birth, parental health problems during childhood (ages 0–12) and hospital admissions due to violence, self-harm and substance use in adolescence (ages 13–19). The incidence of hospital admissions peaked at ages 15 and 19, but as the associations between both parental education and parental health problems and hospital admissions were consistent across adolescence with no significant age interaction, we present overall estimates adjusted for age of occurrence (follow-up divided into 1-year periods by age at year-end). To estimate the extent to which the coefficients for parental education could be explained by parental health problems, we used the Karlson-Holm-Breen method31 that allows comparison of regression coefficients in nested non‐linear models by fixing the residual variance on the same scale in each model. As the data included siblings (44% had one sibling, 19% two and 7% three or more), the SEs were clustered at the family level. We present ORs for each independent variable (model 0) adjusted for sex and hospital district (n=20), parental education adjusted for the different categories of parental health problems (models 1–4) and model 5 that is further adjusted for family structure and household income to capture some of the pathways through which parental education and parental health problems may influence adolescent hospital admissions. To assess potential cumulative disadvantage of lower parental education and parental health problems, we tested for interactions between parental education and parental health problems in models 1–5.
Results
Hospital admissions due to violence, self-harm and substance use were 2–3 times more common among adolescents with basic educated parents than those with tertiary educated parents (table 1). The rates were also doubled among those with parental mental health problems and tripled among those whose either parent had been hospitalised due to violence, self-harm and substance use. Hospital admissions were more common among girls than boys (2.44 vs 2.05 per 1000), but the gradients by parental education and parental health problems showed no major differences between the sexes. Fathers had been more often hospitalised for violence, self-harm and substance use than mothers (3.7% vs 1.7%), but both maternal and paternal health problems showed largely similar associations with girls' and boys' hospital admissions in adolescence. As there were no notable interactions by offspring or parent sex in the associations between parental education and health problems and offspring hospital admissions (p>0.08), we present further results for both sexes together and focus on health problems of either parent.
Rates (per 1000 person-years) of hospital admissions due to violence, self-harm and substance use by parental education and parental health problems, girls and boys aged 13–19, 2001–2011
Parental health problems were more common among the lower educated parents. Fourteen per cent of adolescents with only basic educated parents had a parent hospitalised due to violence, self-harm and substance use during their childhood as opposed to 2% among those with tertiary educated parents. The differences in somatic (72% vs 65%) and mental health problems (9% vs 3%) were less pronounced, but clear (table 2).
Proportion with childhood experience (ages 0–12 years) of parental health problems
Despite the clustering of health problems among the lower educated parents, the higher odds of hospital admissions among adolescents with lower parental education were only modestly attenuated when parental health problems were included in the model (from OR 2.73 (95% CI 2.34 to 3.18) to OR 2.38 (2.04 to 2.77)) for basic parental education). The attenuation was mostly due to adjustment for parental hospital admission for violence, self-harm and substance use, whereas adjustment for parental somatic health problems had practically no effect on the educational gradient (table 3, 95% CIs for models 1–3 in online appendix B). There was no significant interaction between parental education and any of the parental health problems (p>0.51): having both lower parental education and parental health problems showed simple cumulative effects, with a similar educational gradient within each category of parental health problems (unadjusted rates shown in figure 2). Compared with the overall rates among offspring of tertiary educated parents, the rates were over fivefold for adolescents with basic parental education and parent hospitalised for mental health problems, or for violence, self-harm or substance use.
Supplemental material

{kind=link}
{kind=link}
Rates (per 1000 person-years) of hospital admissions due to violence, self-harm and substance use at ages 13–19 by parental education and parental health problems, 2001–2011.
ORs of hospital admissions due to violence, self-harm and substance use at ages 13–19 by parental education and parental health problems, 2001–2011
Finally, we adjusted the model with time-varying household income and family structure (model 5, table 3), which attenuated the educational gradient, as well as the higher ORs among those with parental hospital admissions due to mental health problems, or violence, self-harm and substance use. Nevertheless, both parental education and all parental health problems retained direct associations with adolescent hospital admissions, with >70% higher odds among adolescents with only basic parental education, or either parent hospitalised for violence, self-harm and substance use during their childhood.
Discussion
Lower parental education, only basic level in particular, was a strong predictor of adolescent hospital admissions due to violence, self-harm and substance use. We hypothesised childhood exposure to parental health problems such as substance abuse to be a plausible, yet unexplored mechanism mediating this association. However, although hospital-treated health problems were clearly more common among the lower educated parents, parental health played a relatively modest part in the higher rates of hospital admissions among their offspring. The attenuation of the educational gradient was almost exclusively due to high-risk health behaviour-related parental health problems whereas mental and somatic health problems had a negligible impact. Corroborating previous literature on multiple adverse childhood experiences, adolescents with both low parental education and parental health problems had the highest admission rates, but there was no interaction beyond simple cumulative effects. Even when adjusted for time-varying family structure and income, parental education and parental health problems remained independent predictors of adolescent hospital admissions, underlining the importance of acknowledging the specific associations of different social risk factors for adolescent health problems.
Previous research on the pathways between parental socioeconomic background and adolescent outcomes is characterised by high heterogeneity of the study populations, outcomes and measures of childhood family characteristics,24 which makes direct comparisons to existing evidence difficult. A Swedish study on young adult psychotropic medication use concluded that parental education was less important after accounting for adverse childhood experiences: among individuals with no childhood adversities, there were no differences in psychotropic medication use by parental education.17 However, the study did not specify the contribution of parental health from other types of adversities such as social assistance recipiency or parental criminality. In another Swedish study that focused on the effects of parental externalising behaviours with no adjustments for other socioeconomic factors, parental education retained a direct association with young adult alcohol use disorder.32 A recent US study based on The National Survey of Children’s Health highlighted a nuanced pattern of adverse childhood experiences on child health outcomes (ages 0–18) with differences in clustering of risk factors and the harmfulness of specific combinations of exposures.23 In our study, however, parental education and parental health problems showed simple cumulative effects and parental education predicted adolescent hospital admissions regardless of parental health problems, and vice versa.
Both socioeconomic disadvantage and parental health problems may impair the quality of parenting and parent–child relationships, inducing early life stress with lasting effects on offspring.12 24 33 Disentagling their effects is, however, challenging. One motivation for our analyses was the assumption that parental education affects parental health problems: the lower educated parents are more likely to suffer from health problems and engage in high-risk health behaviours than higher educated parents. However, although education is usually attained early in the life course, there is a degree of health-based selection into lower education.34 35 Moreover, early life health problems and high-risk health behaviours such as substance abuse may not only affect educational attainment, but also partnering and childbearing.36 37 The gradient by parental education is thus likely to contain influences of earlier health-related life-course processes. In this study, low household income and family instability appeared as important pathways through which both low parental education and parental health problems exert their influence on offspring hospital admissions. It should be acknowledged that some of the described associations may be due to unmeasured factors; however, further adjustment (results not shown) for childhood experience of parental death, maternal age, maternal and paternal occupational social class, and parental long-term unemployment introduced no major changes.
Strengths and limitations
Using administrative register data, we were able to conduct an 11-year follow-up study on a population-representative sample of 145 000 adolescents with information on parental social background and parental health problems covering all childhood years (0–12). Our measurement of parental and offspring health was based on hospital records with full national coverage. The overall quality of the data in the Finnish Hospital Discharge Register has been estimated to be high,38 and as we only included cases severe enough to require inpatient care, we have no reason to believe that selective hospital admission or differences in seeking treatment would seriously bias our results. Selective under-reporting of external causes of injuries could produce bias if care episodes among offspring of higher educated parents would be less likely to be coded as self-harm or assaults. However, a previous study on injury morbidity among young adults found no evidence of such systematic bias.39 Childhood exposure to parental health problems was assessed with reference to the biological parents. However, not all children live with their parents and the health problems of a non-coresident parent might play a lesser role in their children’s life. Sensitivity analyses that only included parental health problems of coresident parents showed nevertheless highly similar results.
Both the study outcome and childhood exposures to parental hospital admissions due to mental disorders and violence, self-harm and substance use were relatively rare. A long follow-up of administrative hospital discharge data allows population-level studies with sufficient numbers, minimal attrition and no self-report bias, but as a drawback inpatient care captures only the most severe outcomes of high-risk health behaviour and thus represents a conservative estimate of the occurrence of health problems. The observed associations between parental social background and parental and offspring health problems were strong and highly consistent, and inpatient care can be considered the tip of the iceberg of harm caused by high-risk health behaviours.40 It is, however, possible that measures of less severe and more prevalent parental health problems and high-risk health behaviours would have explained a larger part of the educational gradient in adolescent health problems, but further research is needed to confirm this.
Conclusions
Adolescent hospital admissions due to violence, self-harm and substance use showed a strong gradient by parental education with more health problems among offspring of less educated parents. Childhood exposure to parental health problems explained only a modest part of this gradient, <10%. Parental health problems relating to high-risk health behaviours among the lower educated parents appeared most important in this respect, while somatic and mental health problems had a negligible role in explaining the educational gradient. The largely independent associations of different childhood family characteristics and the highest rates of adolescent hospital admissions among offspring with both low parental education and parental health problems highlight the accumulation of risk factors among the most disadvantaged families.
What is already known on this subject
Many health problems and high-risk health behaviours are more common in lower educated families, both among parents and their children.
A large literature on adverse childhood experiences has also documented multiple family-level risk factors for worse adolescent health outcomes and high-risk health behaviours.
What this study adds
Based on large population-representative data, low parental education and severe parental health problems were strong predictors of adolescent hospital admissions due to violence, self-harm and substance use.
Childhood experience of parental health problems, although more common among offspring of lower educated parents, explained <10% of the educational gradient.
The attenuation was mostly due to high-risk health behaviour-related parental health problems whereas mental and somatic health problems had a negligible impact.
Policies designed to tackle high-risk health behaviour related morbidity among youth need to recognise the cumulative risks of socioeconomic disadvantage and parental health problems.
References
Footnotes
Patient consent for publication Not required.
Contributors HR participated in the conception and design of the study, performed statistical analyses and wrote the first version of the manuscript. HM, LK and PM participated in the conception and design of the study and read and revised the draft versions of the manuscript.
Funding The study was supported by the Academy of Finland, grant number 294861.
Competing interests None declared.
Ethics approval Statistics Finland Board of Statistical Ethics has approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.