Article Text

Abstract
Background: Despite growing inmate populations in the USA, inmates are excluded from most national health surveys and little is known about whether the prevalence of chronic disease differs between inmates and the non-institutionalised population.
Methods: Nationally representative, cross-sectional data from the 2002 Survey of Inmates in Local Jails, 2004 Survey of Inmates in State and Federal Correctional Facilities and 2002–4 National Health Interview Survey Sample Adult Files on individuals aged 18–65 were used. Binary and multinomial logistic regression were used to compare the prevalence of self-reported chronic medical conditions among jail (n = 6582) and prison (n = 14 373) inmates and non-institutionalised (n = 76 597) adults after adjusting for age, sex, race, education, employment, the USA as birthplace, marital status and alcohol consumption. Prevalence and adjusted ORs with 95% CIs were calculated for nine important chronic conditions.
Results: Compared with the general population, jail and prison inmates had higher odds of hypertension (ORjail 1.19; 95% CI 1.08 to 1.31; ORprison 1.17; 95% CI 1.09 to 1.27), asthma (ORjail 1.41; 95% CI 1.28 to 1.56; ORprison 1.34; 95% CI 1.22 to 1.46), arthritis (ORjail 1.65; 95% CI 1.47 to 1.84; ORprison 1.66; 95% CI 1.54 to 1.80), cervical cancer (ORjail 4.16; 95% CI 3.13 to 5.53; ORprison 4.82; 95% CI 3.74 to 6.22), and hepatitis (ORjail 2.57; 95% CI 2.20 to 3.00; ORprison 4.23; 95% CI 3.71 to 4.82), but no increased odds of diabetes, angina or myocardial infarction, and lower odds of obesity.
Conclusions: Jail and prison inmates had a higher burden of most chronic medical conditions than the general population even with adjustment for important sociodemographic differences and alcohol consumption.
Statistics from Altmetric.com
Little is known about chronic diseases among US jail and prison inmates despite the large size of these populations and their growth over the last 30 years.1 2 3 At mid-year 2006, more than 2.2 million people were in jails and prisons in the USA,4 and many more people interact with the criminal justice system over the course of a year.5 National surveys tracking the health of the US population—such as the National Health Interview Survey—typically exclude individuals living in institutions, including jails and prisons. Jails generally hold individuals awaiting trial or serving short-term sentences for misdemeanours, and are usually run by counties and municipalities. Prisons are often run by state or federal governments and hold individuals convicted of crimes and receiving sentences of a year or more. Better understanding of the relative prevalence of chronic conditions, including conditions designated as national priority areas for improvement in healthcare quality by the Institute of Medicine,6 is necessary to address effectively the needs of the growing inmate population in the USA.
Inmates may be at increased risk of poor medical outcomes compared with the general population due to circumstances before and during incarceration. Inmates often come from disadvantaged backgrounds and have low levels of education; report high levels of smoking, drinking and illicit drug use before incarceration; have poor nutrition and limited physical activity in jail or prison; report mental health and neurological disorders such as schizophrenia, depression and epilepsy that may complicate efforts to prevent or treat chronic health conditions; are exposed to infectious disease through risky drug injection or sex practices; have high levels of stress, anxiety, sleep deprivation and depression; and have lower levels of self-efficacy as a result of the stigma and loss of social ties associated with being incarcerated.7 8 9 10 11 12 13 Studies have documented worse health and increased risks of death, including death from cardiovascular disease and cancer, among inmates after release than the general population,14 15 16 suggesting the prevalence of underlying chronic disease may be higher among inmates than the general population. Recent work on the prevalence of selected conditions in inmates suggested higher prevalence of diabetes, hypertension, asthma and HIV than the general population,7 17 but estimates did not adjust for possible confounders, including sex,12 race/ethnicity, education and other factors known to affect the prevalence of disease.
We quantified differences in prevalence of major medical conditions, including cardiovascular risk factors and disease, pulmonary disease, arthritis, cancer and hepatitis among inmates within the non-institutionalised US adult population. We determined whether age, sex, race, education, employment, USA as birthplace and alcohol consumption—key predictors of health and mortality18 19—accounted for differences in medical conditions across jail inmates, prison inmates and non-institutionalised adults.
Methods
Data
Three data sources were used to address our aims. The 2002 Survey of Inmates in Local Jails (SILJ)20 is the most recent cross-sectional survey of a nationally representative sample of jail inmates (data released for analysis in 2006). Interviewers from the Bureau of the Census, under supervision of the Bureau of Justice Statistics, conducted hour-long, structured, in-person interviews of 6982 inmates in 417 jails. Out of 465 jails selected to participate, 417 (89.7%) were available (39 refused and 9 were closed or had no inmates). Among inmates selected to participate, 263 refused, 407 were released after sampling and 98 were not interviewed due to medical, security or other administrative reasons.20 Based on criteria by the American Association for Public Opinion Research (AAPOR)21 and taking both sampling stages into account, the total response rate was 84.1%. Study methods are described in greater detail by the Bureau of Justice Statistics.22
The 2004 Survey of Inmates in State and Federal Correctional Facilities (SISFCF) provided data from the most recent cross-sectional, nationally representative survey of state and Federal prison inmates (data released for analysis in 2007).23 The SISFCF largely resembled the SIJL in format and content. Prison facilities of all security levels were eligible. Of 297 state prisons selected, two refused and 12 were out of scope. Four reserve female prisons were added for a total of 287 participating state prisons. One of the 40 sampled Federal prisons did not participate. Based on AAPOR criteria,21 and response rates among both prisons and inmates, the total response rate was 89.1% for state prisons and 84.6% for federal prisons.23 Both jail and prison inmates were told verbally and in writing that participation in the survey was voluntary, answers were confidential, the survey was for statistical purposes and individuals would not be identified in the results.
The 2002, 2003 and 2004 waves of the National Health Interview Survey-Sample Adult File (NHIS-SAF) provided a nationally representative sample of non-institutionalised adults aged 18 and older over the same time period as the inmate surveys.24 The NHIS-SAF comprises data from in-person interviews with a randomly selected adult from sampled households who provides detailed information on his or her health. In 3 years of NHIS-SAF data, 14 071 of 122 732 eligible households did not participate, 1364 of 112 237 eligible families did not participate and 17 477 of 110 699 eligible sample adults did not participate. Based on criteria,21 the final response rate was 73.9% for the 3 survey years (74.6% in 2002, 74.5% in 2003 and 72.7% in 2004). NHIS-SAF respondents were told verbally and in writing that responses were confidential and they were free to not answer any question.
Individuals aged 17 or younger were excluded because they were not surveyed in the NHIS-SAF, as were individuals aged 66 or older because there were too few older adults in the inmate surveys. Our analyses included 6582 jail inmates, 14 373 prison inmates and 76 597 non-institutionalised adults.
Variables
Key demographic variables were self-reported and assessed similarly across surveys. We grouped respondents into three, 16-year age categories: 18–34, 35–49 and 50–65. Race/ethnicity was self-reported and coded as non-Hispanic white, non-Hispanic black, Hispanic, American Indian/Alaska Native, Asian and other/multiple race. We were interested in racial and ethnic differences in prevalence of chronic conditions because non-Hispanic black people and Hispanics are over-represented in correctional institutions. Nativity contrasted US- and foreign-born individuals. Marital status was coded as married, widowed, divorced, separated and never married. We categorised education as 8 years or less, 9 or more years but no high school diploma, high school diploma or GED (ie, high school equivalency certificate), and any college or more. Employment was coded as employed (had a job or business) in the month prior to arrest (among inmates) or in the week before the interview (among NHIS-SAF respondents). Alcohol consumption was categorised as: never, less than weekly or weekly in the year before the offence for which individuals were incarcerated (among inmates) or in the last year (among NHIS-SAF respondents). Data on smoking were available in the prison survey and NHIS-SAF, but not in the jail survey. Respondents were categorised as never (fewer than 100 cigarettes in entire life), former (100 or more cigarettes in lifetime but not current smokers) or current smokers.
We selected chronic medical conditions identified as priority areas for improvement in healthcare quality by the Institute of Medicine (hypertension, ischaemic heart disease, asthma, diabetes, obesity and cervical cancer)6 or had particular significance in correctional settings (viral and alcoholic hepatitis and arthritis)11 25 26 and that were assessed with similar questions across data sets (appendix). We were unable to examine conditions, such as depression, psychotic disorders or epilepsy, that were not assessed in one or more of the surveys, or that were not assessed in similar ways.
Cardiovascular risk factors included self-reports of hypertension or diabetes. Self-reported height and weight were used to calculate body mass index (BMI) as weight in kilograms over height in meters, squared. BMI was categorised following World Health Organization standards as underweight (BMI<18.5), normal weight (18.5⩽BMI<25.0), overweight (25.0⩽BMI<30) and obese (BMI⩾30.0).27 Chronic diseases included self-reports of angina, heart attack/myocardial infarction, asthma, arthritis, any cancer or malignancy, or cervical cancer. The question for hepatitis did not distinguish among causes of acute or chronic hepatitis (eg, viral, alcoholic or autoimmune hepatitis; see appendix).
Analyses
Based on sample sizes, we had a power of 0.93 to detect differences in a condition occurring in 1% of those not institutionalised but in 1.5% of those in jail (the smallest of our three samples), with a two-sided α of 0.05. All conditions exhibited an unadjusted prevalence of greater than 1%. After pooling the data, we used multinomial logistic regression to model BMI categories (with underweight, overweight and obese compared with normal weight individuals) and logistic regression to model other conditions. BMI was the dependent variable with the greatest level of missing data (4.8% in the NHIS-SAF data), and in models that included all of our covariates we dropped 9.5% of jail inmates, 6.3% of prison inmates and 6.8% of non-institutionalised adults. The Bureau of Justice Statistics used hot-deck methods to impute missing race/ethnicity for jail inmates. Hot-deck methods draw values for missing data from respondents with non-missing data who are matched on key characteristics, such as the type of facility, age, sex or other factors. Hot-deck methods typically reduce the variability in the data and lead to CIs that are too narrow.28 Because the public release data did not flag the imputed observations, we could not compare estimates that included the imputed observations from estimates that excluded those observations.
Estimated regression models adjusted for the three age strata, sex and variables indicating jail or prison inmates, then calculated the predicted probability of each condition for each group. Three models were used to examine the odds of each condition. Model 1 estimated ORs and 95% CIs for jail inmates and prison inmates compared with non-institutionalised adults, while adjusting for sex and age as a linear variable. Model 2 further adjusted for race, education, employment, USA as birthplace, marital status and alcohol consumption, in addition to variables from Model 1. Model 3 further adjusted for smoking status to examine whether it accounted for differences between prison inmates and non-institutionalised adults (smoking questions were not asked of jail inmates). We also tested for interactions between inmate status and sex and race.
After pooling the data, we weighted each source accounting for survey non-response and ensuring representative estimates of each population. We used ‘svy’ commands in Stata Statistical Software: Release 10.029 to produce Taylor linearised standard errors that account for the stratified, multistage sampling frame used by each survey (ie, non-independence of inmates within prisons or jails, or of non-institutionalised adults in primary sampling units in the NHIS-SAF). We followed the method described by Korn and Graubard30 when pooling surveys with different sampling frames. We specified our weights as “probability weights” in Stata to ensure standard errors were estimated appropriately. Preliminary analyses adjusted for survey year in addition to covariates mentioned above, but final models excluded survey year due to lacking evidence of temporal trends.
Results
Mean age was 40.0 years (standard error (SE) 0.9) for non-institutionalised adults, 32.1 years (SE 0.2) for jail inmates and 35.6 years (SE 0.2) for prison inmates. Non-institutionalised adults were less likely to be male (n = 34 646; weighted prevalence 49.1%; 95% CI 48.6% to 49.5%) than jail (n = 4629; weighted prevalence 88.3%; 95% CI 87.0% to 89.5%) and prison (n = 11 040; weighted prevalence 92.6%; 95% CI, 90.1% to 94.5%) inmates (table 1). Non-Hispanic Blacks were over-represented in jails (n = 2560; weighted prevalence 39.7%; 95% CI 36.7% to 43.8%) and prisons (n = 5386; weighted prevalence 38.1%; 95% CI 35.7% to 40.6%) compared with non-institutionalised adults (n = 10 894; weighted prevalence 11.8%; 95% CI 11.3% to 12.4%). Hispanics were also over-represented in jails (n = 1159; weighted prevalence 18.5%; 95% CI 16.1% to 21.2%) and prisons (n = 2835; weighted prevalence 19.7%; 95% CI 17.8% to 21.8%) compared with non-institutionalised adults (n = 14 464; weighted prevalence 12.8%; 95% CI 12.2% to 13.3%).
Weighted estimates of characteristics of non-institutionalised adults, jail inmates, and prison inmates (2002–4)
Jail and prison inmates had a higher prevalence of hypertension, diabetes, myocardial infarction, asthma, arthritis, cervical cancer and hepatitis than non-institutionalised adults (n = 76 597) across all three age strata, after adjustment for sex (table 2). In contrast, obesity was less prevalent among jail inmates than non-institutionalised adults or prison inmates. The prevalence of underweight was lower among prison inmates than non-institutionalised adults. Angina was similarly reported across populations.
Weighted prevalence (%) and 95% CIs of chronic conditions at three age strata, adjusted for sex
Inmates had significantly higher odds of hypertension, diabetes, myocardial infarction, asthma, arthritis, cervical cancer and hepatitis than non-institutionalised adults, after adjusting for age and sex (table 3, Model 1). After further adjustment for race, education, USA as birthplace, marital status, employment and alcohol consumption (Model 2), jail and prison inmates had persistently elevated odds of hypertension (ORjail 1.19; 95% CI 1.08 to 1.31; ORprison 1.17; 95% CI 1.09 to 1.27), asthma (ORjail 1.41; 95% CI 1.28 to 1.56; ORprison 1.34; 95% CI 1.22 to 1.46), arthritis (ORjail 1.65; 95% CI 1.47 to 1.84; ORprison 1.66; 95% CI 1.54 to 1.80), cervical cancer (ORjail 4.16; 95% CI 3.13 to 5.53; ORprison 4.82; 95% CI 3.74 to 6.22) and hepatitis (ORjail 2.57; 95% CI 2.20 to 3.00; ORprison 4.23; 95% CI 3.71 to 4.82) compared with non-institutionalised adults, but differences in diabetes (ORjail 1.06; 95% CI 0.98 to 1.28; ORprison 1.12; 95% CI 0.98 to 1.26) and myocardial infarction (ORjail 1.22; 95% CI 0.89 to 1.67; ORprison 1.07; 95% CI 0.86 to 1.32) were no longer significant. Jail inmates had no increased odds of cancer (ORjail 1.19; 95% CI 0.97 to 1.45) whereas prison inmates had higher odds of cancer than non-institutionalised adults (ORprison 1.22; 95% CI 1.03 to 1.44). Jail inmates had lower odds of obesity (ORjail 0.45; 95% CI 0.40 to 0.51) or overweight (ORjail 0.45; 95% CI 0.40 to 0.51), and prison inmates had lower odds of obesity (ORprison 0.80; 95% CI 0.72 to 0.88) than non-institutionalised adults. These differences were larger or changed direction from those estimated in Model 1.
ORs for chronic conditions in jail inmates compared with non-institutionalised adults and prison inmates compared with non-institutionalised adults
Jail and prison inmates had somewhat different disease profiles. Prison inmates had significantly higher odds of obesity or being overweight and reporting hepatitis, but lower odds of being underweight than jail inmates (table 3, Model 2). After adjusting for smoking status (table 3, Model 3), all-cause cancer was not significantly higher among prison inmates (ORprison 1.13; 95% CI 0.94 to 1.35) than non-institutionalised adults. We found significant interactions between jail or prison inmate status and sex and race for each medical condition in models that were also adjusted for education, USA as birthplace, and marital status, alcohol consumption and employment, and were age standardised at 45. Although women had similar or lower prevalence of each condition than men in the non-institutionalised population, they had a higher prevalence than men in jails and prisons. Figure 1 illustrates these findings with two chronic conditions common among inmates: hypertension and hepatitis.

Adjusted* prevalence (%) and 95% CIs of Selected conditions for men (x) and women (o) in non-institutionalised adults, jail inmates, and prison inmates. *Adjusted for race, education, USA as birthplace, and marital status, alcohol consumption and employment at age 45.
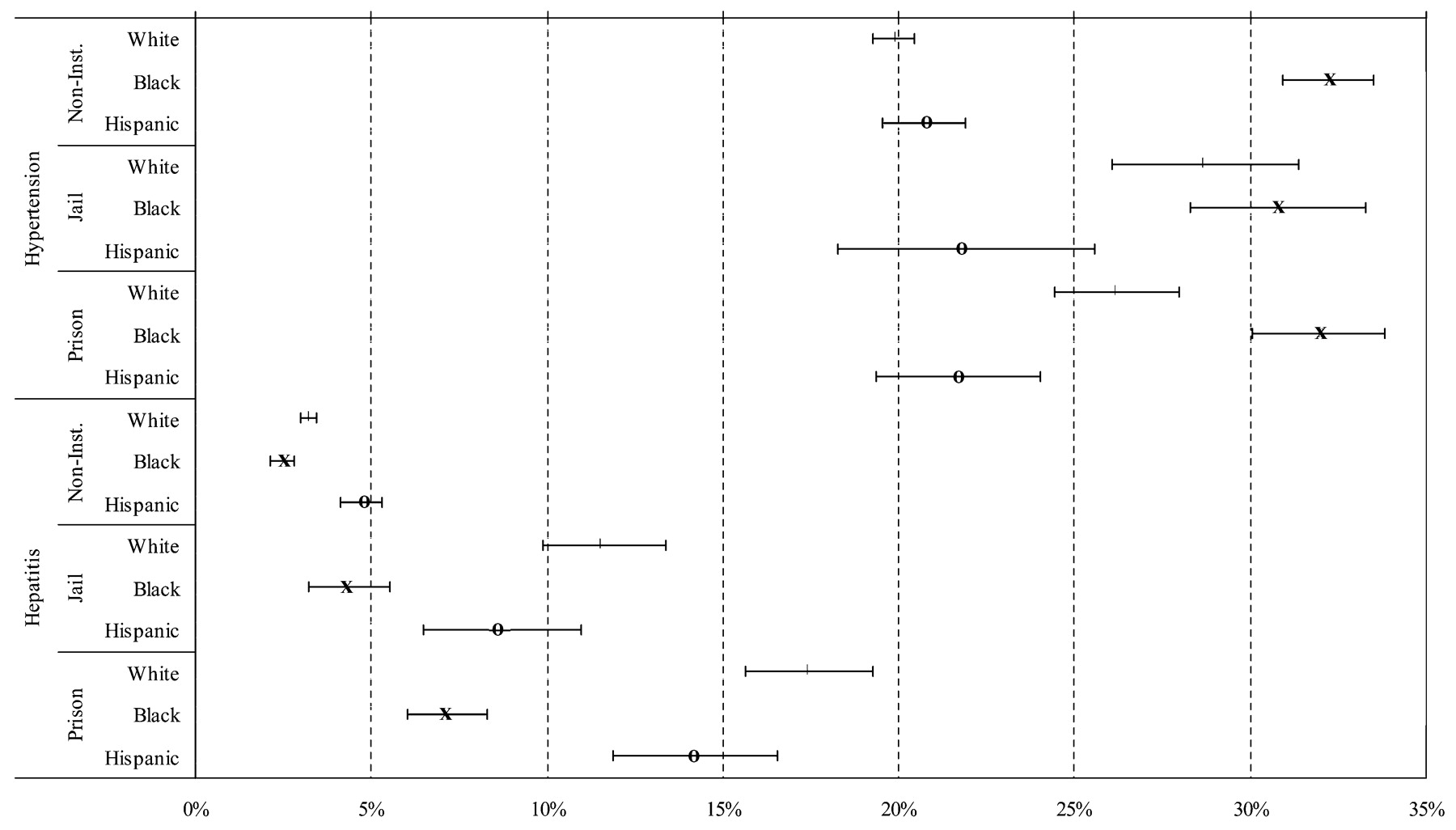
Being incarcerated was associated with a greater prevalence of each condition among non-Hispanic Whites than non-Hispanic blacks or Hispanics compared with non-institutionalised adults. Figure 2 illustrates that non-Hispanic whites and Hispanics had a lower adjusted prevalence of hypertension than non-Hispanic blacks in the general population. However, in jails, non-Hispanic whites had a similar prevalence of hypertension compared with non-Hispanic blacks, and in prisons non-Hispanic whites had a prevalence of hypertension between the prevalence for Hispanics and non-Hispanic blacks. For hepatitis, non-Hispanic whites had a lower adjusted prevalence than Hispanics in the non-institutionalised population, but not in the inmate populations, where the prevalence was similar among Hispanics and non-Hispanic whites.
{kind=link}
{kind=link}
Adjusted* prevalence (%) and 95% CI of Selected conditions for whites (|), blacks (x), and Hispanics (o) among non-institutionalised adults, jail inmates and prison inmates. *Adjusted for sex, education, USA as birthplace, marital status, alcohol consumption and employment at age 45.
Discussion
Prevalence of many chronic medical conditions was higher among jail and prison inmates than in the non-institutionalised population. After adjusting for a range of sociodemographic factors and alcohol consumption, inmates had lower odds of obesity, but higher odds of hypertension, asthma, arthritis, cancer, cervical cancer and hepatitis, and comparable odds of diabetes, angina and myocardial infarction. These results can be used to guide correctional health providers and administrators in allocating limited resources towards chronic health conditions most likely to cause adverse events and benefit from early treatment.
Increased odds of hypertension, hepatitis and cancer among inmates may partly explain excess mortality from cardiovascular, liver disease and liver cancer among former inmates.14 Incarceration was associated with greater prevalence of hypertension, hepatitis and cancer among women than men. Consistent with findings from England and Wales,12 and in contrast to findings from Australia,31 we found more modest race/ethnic differences in health within jails and prisons than in the non-institutionalised population. Specifically, we found that incarceration was associated with greater prevalence of chronic medical conditions among non-Hispanic whites than non-Hispanic blacks or Hispanics. These findings are also consistent with prior research indicating that the relative risk for death among whites released from prison compared with whites in the general population was greater than the relative risk among African–Americans released from prison compared with African–Americans in the general population.14 Our findings contradict the common perception that poor health among inmates is driven solely by the high concentration of racial/ethnic minority men in correctional systems.
This study has several limitations. Because inmates are typically young, we were unable to examine conditions that are rare among younger adults, such as colon cancer. Self-reporting of chronic diseases among inmates has not been validated with confirmatory testing, but reports of disease prevalence increased by age group in the expected direction. Inmates may be less likely to be screened and diagnosed with certain conditions, such as diabetes, compared with community counterparts and, therefore, under-report these conditions. For instance, incarcerated women with high cholesterol were less likely to be aware of their condition than non-incarcerated women in a study from North Dakota.32 On the other hand, inmates may have greater screening opportunity for other conditions such as chronic viral hepatitis, than individuals in the community. Inmates may also over-report medical conditions intentionally or due to recall bias or may interpret broad questions about conditions such as hepatitis differently from non-institutionalised populations. Further studies on the validity of self-report among inmates are indicated. Weight may have been misreported by both inmates and respondents in the general population; inmates in particular may not have routine access to scales. Thus, our findings for BMI should be confirmed in studies with measured weight and height. We found, however, better response rates among jail and prison inmates than among non-institutionalised adults, suggesting that the responses of inmates may be more representative of the underlying population of inmates than are surveys of non-institutionalised adults.
We could not determine whether individuals in worse health were more likely to commit crimes and be incarcerated, or whether incarceration led to worse health by exposing inmates to adverse lifestyles, increased risks of infection, or psychosocial stress and stigma; limited research with longitudinal data suggests both processes may be at play.9 33 Greater detail on socioeconomic indicators and mental health disorders might account for observed differences between jail, prison and non-institutionalised populations, or high prevalence of disease among incarcerated white people, relative to incarcerated black people. Further, greater detail on smoking or drinking or information on exercise or nutrition could account for differences across the groups we examined. Income questions differed substantially across surveys and data on the neighbourhood of origin and arrest were unavailable for inmates. However, we adjusted for education and employment, and used separate models (not shown) for receipt of public assistance, which yielded results virtually identical to those presented herein. Drug misuse was not assessed similarly across surveys; if it were available, it might have accounted for of the increased odds of hepatitis among inmates. We propose that related questions be identical in future correctional and national health surveys or that national health surveys be conducted in correctional settings and that the data are released earlier to allow for timely comparisons. Improved coordination of surveillance and survey efforts between institutional and non-institutional settings would lead to better understanding of differences in disease prevalence across populations.
Voluntary correctional accrediting organisations, such as the National Commission on Correctional Health Care, have set quality standards in jails and prisons, but correctional settings are generally excluded from community efforts to improve health outcomes. Since chronic conditions and resulting morbidity are commonly treated after release,34 correctional settings should be a part of local and national quality improvement efforts. Community physicians often provide care to formerly incarcerated individuals. Appropriate management of these chronic conditions will require coordinating health services during incarceration, transition to the community and after release, as well as the development of health policies that support these efforts.
What is already known on this subject
Jail and prison inmates are a growing and disadvantaged population in the USA.
Because inmates are typically excluded from national health surveys, we have little knowledge about the national prevlance of disease among inmates; whether sociodemographic factors account for differences among jail inmates, prison inmates, and non-institutionalised adults; and whether race/ethnic and sex disparities in medical conditions that have been documented among non-institutionalised adults also manifest among inmates.
What this study adds
The prevalence of many chronic medical conditions was higher among jail and prison inmates than among non-institutionalised adults.
After adjusting for a range of sociodemographic factors and alcohol consumption, inmates had lower odds of obesity, but had significantly higher odds of hypertension, asthma, arthritis, cancer, cervical cancer and hepatitis, and comparable odds of diabetes, angina and myocardial infarction.
Being in jail or prison was associated with a much greater increase in the odds of each condition for non-Hispanic whites and women than for non-Hispanic blacks, Hispanics and men, respectively.
These results suggest the allocation of limited resources for health among inmates towards chronic health conditions most likely to cause adverse events and benefit from early treatment.
Acknowledgments
We wish to thank Susanne Felton, MA, Professional Research Assistant, of the University of Colorado Denver for her assistance with the coordination of Institutional Review Board authorisations to conduct this study, and her review of the manuscript. We wish to thank Emily Warren, MA of the University of Colorado Denver for her review of the manuscript.
REFERENCES
Supplementary materials
Web only appendix 63:11;912
Files in this Data Supplement:
Footnotes
Appendix available online only at http://jech.bmj.com/content/vol63/issue11
Funding IAB was supported by the Robert Wood Johnson Foundation Physician Faculty Scholars Program and the Division of General Internal Medicine, Department of Medicine, University of Colorado Denver School of Medicine. PMK was supported by the Population Research Center at the University of Texas at Austin (NICHD R24 HD42849) and the Population Program at the University of Colorado-Boulder (NICHD R21 HD51146). The funders had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Competing interests None declared.
Ethics approval The protocol was approved by the Colorado Multiple Institutional Review Board and University of Texas Health Sciences Center, Houston review board.
Provenance and peer review Not commissioned; externally peer reviewed.