


The use of solitary confinement, particularly with mentally ill prisoners, has become a central focus of prison reform efforts in recent years. Numerous articles in the scholarly literature and popular media have chronicled the experiences of prisoners placed in long-term isolation, shining a spotlight on the growing use of the practice and its detrimental effects.1,–,3 This media attention has served to raise public consciousness about the potential harms of solitary confinement, and, in conjunction with lawsuits filed against prison systems, has formed the basis of the Stop Solitary movement in the United States. By 2013, the movement had grown to involve, not only prisoners and civil liberties advocates, but also corrections officials,4 religious leaders,5 professional organizations,6 and international human rights experts.7
Psychiatrists and psychologists have played an essential role in the Stop Solitary movement, giving legitimacy to what could have been dismissed as frivolous complaints by prisoners. Initial psychiatric studies focused on clinical observations, documenting the feelings of loneliness, confusion, and agitation associated with long-term isolation.8 More recent studies have found a higher incidence of suicide and self-injury in restrictive housing settings,9 as well as a disproportionate number of prisoners with serious mental illness placed in isolation.10 The 2012 publication of an American Psychiatric Association (APA) position statement on solitary confinement reflected a professional consensus that long-term isolation is harmful to prisoners with serious mental illness, either by directly causing clinical deterioration or by depriving them of treatment that would have resulted in improvement.6 Although some scholars debate whether isolation is the cause or effect of the dangerous behavior observed in prisoners housed in isolation,11 it is clear that, at the very least, isolation adds no benefit to the treatment of mental illness in prison.
The mounting body of medical literature documenting the effects of solitary confinement has enhanced the ability of prison reform advocates to bring legal challenges against its use in mentally ill prisoners. Numerous lawsuits and CRIPA (Civil Rights of Institutionalized Personal Act of 1980) investigations have alleged that long-term isolation, typically defined as greater than 22 hours per day of in-cell confinement, violates prisoners' constitutional rights.12,–,14 These legal challenges have been relatively successful, as courts have agreed that placing mentally ill prisoners in long-term solitary confinement violates the Eighth Amendment prohibition against cruel and unusual punishment.12,–,14 As one decision noted, placing mentally ill prisoners in isolation “is the mental equivalent of putting an asthmatic in a place with little air….”12 In another decision, the court stated that “long periods of solitary confinement can have devastating effects on the mental well-being of a detainee.”15
As a result of litigation, conditions in some correctional systems have improved dramatically for inmates with mental illness. States such as Colorado, Maine, Mississippi, Virginia, and Illinois have significantly reduced the use of solitary confinement, while saving money and experiencing no increase in rates of violence.16 Other states are following their examples. While more work undoubtedly remains to be done, legal challenges to solitary confinement have created an important avenue for initiating reforms to improve care of mentally ill prisoners.
Too Narrow a Focus?
A cursory glance at media coverage of prisons could easily lead one to conclude that solitary confinement is the single worst thing that happens to inmates with mental illness in correctional settings. Many articles make no mention of other serious problems with access to mental health care in prisons, such as chronic understaffing, lack of screening for mental illness, inadequate training for corrections officers, and poor coordination between community and correctional health services. Presumably, the stories of individual inmates and their psychological deterioration in solitary confinement are so powerful that they need not be supplemented with additional facts.
This approach has been helpful in building coalitions, as many different groups can resonate with the narratives of individual inmates and come together in support of stopping solitary confinement. However, it has also greatly intensified the focus on one particular topic (the use of isolation) at the expense of other important aspects of improving prison health care. For example, if a prisoner with serious mental illness has never been placed in solitary confinement, but has no access to meaningful mental health care, is he not also worthy of advocacy efforts? Furthermore, would all of the problems of mentally ill prisoners be solved if those inmates were simply removed from isolation units?
To be fair, the focus of media and legal advocates on a particular aspect of prison life is nothing new; past coverage has tackled such concerns as sexual violence or the plight of incarcerated mothers.17,18 Similarly, the focus of prison litigation has undergone cycles in which a particular topic is more or less popular: overcrowding, excessive use of force, and health care. These areas of interest are, of course, based on the goals of the media (to provide interesting content to viewers or the readership) and the legal advocates (to create the strongest case for litigation). The accounts are not meant to be exhaustive renderings of the many harms of prison or even a complete report of the harms encountered by persons with mental illness in prison.
As psychiatrists, we have a different mandate to advocate for improving all aspects of mental health care in correctional settings. We can and should consider the effects of solitary confinement, but we should do so with a goal of integrating changes to isolation practices into larger reform efforts to improve the system of prison mental health care. To date, we have made important progress in this area, particularly with the creation of standards for correctional health care and position statements against the use of prolonged isolation on patients with mental illness.6,19,20 As a profession, we have stated with clarity that persons with mental illness deserve high-quality treatment, regardless of their status as prisoners.19 Furthermore, we have stated that prisoners with mental illness are particularly vulnerable, and the use of the most extreme forms of punishment should be avoided with them.6
Where we must work harder, however, is in delineating the many ways in which solitary confinement harms prisoners with mental illness. Much of our attention has so far been focused on the fairly narrow question of whether a healthy person will develop mental illness (the so-called SHU (special housing unit) Syndrome) if placed in solitary confinement. Studies about this subject have yielded conflicting results, some concluding that long-term isolation causes a delirium-like syndrome21 and others finding that previously healthy people are likely to remain healthy.11,22 In trying to explain these conflicting results, scholars have criticized each other for using flawed methodologies or demonstrating bias, even going so far as to label particular studies as “garbage.”23 The subject remains a hotly contested area of scholarly debate, and further research is being undertaken.
Although the question of whether solitary confinement creates mental illness in otherwise healthy people is certainly important from a scientific perspective, there is also value in taking a step back and considering the harms of solitary confinement in a broader sense. For example, even if we prove conclusively that solitary confinement does not harm healthy individuals, there are still many ways in which persons with mental illness are harmed by those conditions. As psychiatrists, we should study all of the problems associated with the continued use of solitary confinement in prisons, moving beyond the question of SHU syndrome and advocating for the broader needs of our patients.
Reframing the Solitary Confinement Discussion
In considering the broad-based harm of solitary confinement, some legal advocates have made the connection between solitary confinement and other harmful conditions for mentally ill prisoners. Class-action suits alleging constitutional violations typically include the use of solitary confinement as one of the harms, but not the only harm, perpetrated by the prison system with regard to mental health care. For example, in Gamez v. Ryan,24 solitary confinement was identified as one element of a grossly inadequate medical system in Arizona. In Madrid v. Gomez,12 placement of individuals with mental illness in isolation was included as part of a larger effort to eliminate the use of excessive force in California's supermax facilities. These cases demonstrate how legal advocates use solitary confinement as a starting point, but with the ultimate strategy of creating broader changes in prison conditions.
Madrid v. Gomez and Gamez v. Ryan provide a model of integrating the topic of solitary confinement with other prison conditions, and a recent U.S. Department of Justice (DOJ) investigation offers a model for examining the multifactorial harms of solitary confinement itself. In its investigation of a Pennsylvania correctional facility, DOJ created a three-part framework for examining the effects of solitary confinement on individuals with mental illness.25 First, the investigators considered the direct effects of solitary confinement on mental health: both the SHU syndrome and the exacerbation of other mental illnesses. Second, they examined the lack of access to mental health care created by placement in segregation, such as the inability to participate in group or individual psychotherapy. Third, they addressed the combination of isolation with other harsh conditions of confinement, such as the excessive use of force or unclean living conditions. By focusing not only on the narrow question of whether solitary confinement can cause mental illness de novo, DOJ included other important systemic concerns about the prison in its investigation: understaffing, marginalization of mental health staff, inadequate oversight, and others. Solitary confinement was presented not just as a harm in itself, but also as the final common pathway in a grossly inadequate mental health system.
Figure 1 illustrates this concept in more detail. Many factors lead to the increased use of isolation of mentally ill inmates. First, inadequate screening for mental illness allows many inmates to go undiagnosed, and behavior that is related to mental illness will be punished with placement in isolation rather than treated with medication or psychotherapy. Even if inmates are appropriately identified as mentally ill, providing inadequate resources to treat them ultimately leads to the same result. A professional culture in which mental health professionals are encouraged to label inmates as “behavioral” rather than truly ill can also contribute to the increased use of isolation. Finally, an environment in which the concerns of mental health staff are overshadowed by those of security staff can lead to the increased placement of inmates in isolation, either because mental illness is not recognized or as retaliation against mental health staff who are perceived as inmate lovers.
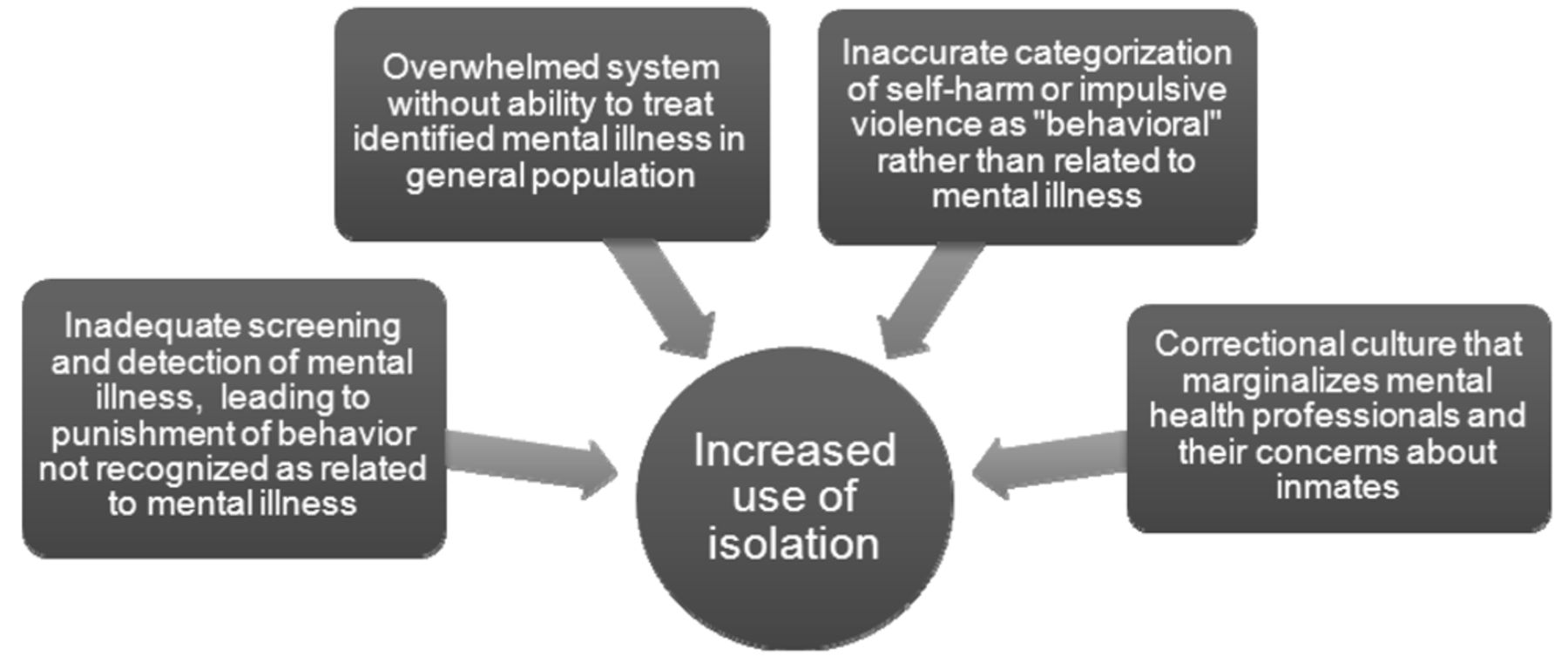
Solitary confinement as a final common pathway in inadequate correctional mental health systems.
The relationship between solitary confinement and mental illness can also be viewed as a cycle. As illustrated in Figure 2, placement in solitary confinement feeds on itself, requiring ever-increasing resources to care adequately for the needs of inmates in that setting. For example, as inmates with mental illness are placed in solitary confinement, they need intensive monitoring to assess whether they are deteriorating. The resources used to perform this monitoring must be diverted from elsewhere, typically from general population services. In addition, in cases where inmates deteriorate in isolation, care must be provided for them in an intensive (typically inpatient) mental health setting. Further resources are used in this endeavor, thereby decreasing once again the ability to provide treatment in the general population. The end result is that preventive and routine services are continually short-changed, with resources only available for a response to crises.

Cycle of solitary confinement and mental illness.
Framing the discussion about the effects of solitary confinement in this larger context is essential, as doing so provides an opportunity to address other serious needs of prisoners with mental illness. Taking such an approach can even appeal to the professional pride of corrections officials, encouraging innovation and program development in mental health care that will ultimately lead to the reduced use of isolation. Finally, expanding the discussion about solitary confinement makes it clear to prison systems that they are accountable for changing the underlying conditions that result in overreliance on isolation as a management tool, not just engaging in a shell game of moving prisoners with mental illness into different (often temporary) housing units.
Stopping Solitary Confinement Is Just the Beginning
As psychiatrists, we must not be myopic in our focus on advocating for our patients in correctional settings. We must acknowledge that, sadly, many appalling things still routinely happen in prison to individuals with mental illness, and placement in solitary confinement is just one of them. Every day, prisoners receive substandard treatment of serious mental illnesses. Correctional systems have inadequate resources to provide necessary care, and health care professionals too often stray from their therapeutic mandates, becoming hardened after years of witnessing prisoners manipulate the system. The unfortunate result is that prisoners are frequently misdiagnosed, denied access to treatment, and punished rather than helped by those responsible for caring for them.
Because of these challenges, many private and public agencies have developed programs to divert persons with mental illness from incarceration in recent years.26 We now have widespread recognition that prison is not the ideal setting in which to treat mental illness, and we take steps to reduce the incarceration of mentally ill people when possible. Nonetheless, a significant section of the prison populations still has mental illness and cannot be diverted to another setting. For those people, we must advocate first for removing them from the harshest forms of punishment, such as solitary confinement, and then for improving their access to treatment more broadly.
As we move forward in promoting improved prison mental health care, we must remember that the use of solitary confinement does not occur in a vacuum; it is almost always related to other systemic deficiencies. By framing the problem of solitary confinement as a final common pathway for prisoners stuck in inadequately developed correctional mental health systems, we can create meaningful systemic change. Simply removing prisoners with mental illness from isolation is insufficient. Real reform requires improving the entire system of mental health care in prisons.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2014 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}