


Abstract
In 1995, the Joint Commission began requiring that hospitals report reviewable sentinel events as a condition of maintaining accreditation. Since then, inpatient suicide has been the second most common sentinel event reported to the Joint Commission. The Joint Commission emphasizes the need for around-the-clock observation for inpatients assessed as at high risk for suicide. However, there is sparse literature on the observation of psychiatric patients and no systematic studies or recommendations for best practices. Medical errors can best be reduced by focusing on systems improvements rather than individual provider mistakes. The author describes how failure modes and effects analysis (FMEA) was used proactively by an inpatient psychiatric treatment team to improve psychiatric observation practices by identifying and correcting potential observation process failures. Collection and implementation of observation risk reduction strategies across health care systems is needed to identify best practices and to reduce inpatient suicides.
In To Err Is Human: Building a Safer Health System, the Institute of Medicine (IOM) estimated that 44,000 to 98,000 Americans die each year as a result of medical errors and that deaths in hospitals due to medical errors are the eighth leading cause of death.1
In 1995, the Joint Commission began requiring that hospitals report reviewable sentinel events as a condition of maintaining accreditation. Since then, inpatient suicide has been the second most common sentinel event (after wrong-site surgery) reported to the Joint Commission.2 Of 5208 sentinel events reported to the Joint Commission from January 1995 through June 30, 2008, 641 (12.3%) were inpatient suicides.
A significant number of inpatient suicides occur while patients are on some type of observation status. There is sparse literature on the observation of psychiatric patients and no systematic studies or recommendations for best observation practices. Opinions on the importance of observation practices vary widely. Some describe observation as the critical element in preventing inpatient suicide.3,4 Others disparage observation as a symptom of nurses’ traditional handmaiden role that interferes with good patient care.5,6 There is not even agreement on what to name or how to describe various patient observation levels.
Rational change to improve patient care and decrease errors requires data. Observation can only prevent inpatient suicides when performed effectively and safely. How can an inpatient treatment team determine the best way to carry out observation and avoid clinical error given the total lack of literature on best observation practices?
Improving systems, rather than focusing on individual provider mistakes, is the most effective way to reduce errors. Human factors analysis is used in the study of the “interrelationships between humans, the tools they use, and the environment in which they live and work” (Ref. 1, p 63). Human factors improvements have already significantly reduced errors in anesthesia practice7–11 and have brought intensive care unit central line infection rates almost to zero.12,13 Observation of psychiatric patients requires a complex, sustained interaction between the patient, observer, psychiatrist, nurse, other treatment team members and the psychiatric unit environment. Analyzing and improving how the observation process works could reduce errors and improve patient safety. One systematic approach, failure modes and effects analysis (FMEA) may be particularly useful for improving psychiatric observation practices.
In Crossing the Quality Chasm: A New Health System for the 21st Century, the IOM described six general goals for improving health care from the patient's perspective: safety, effectiveness, patient-centeredness, timeliness, efficiency, and equity.14 However, unique to inpatient suicide prevention is the conflict between the patient's expressed wish to die and the staff's response. The human factors literature and the IOM's patient-centered approach assume that all of the human actors involved, including the patient, intend that the system work correctly and prevent a negative outcome. Suicide prevention requires that the treatment team override the patient's expressed desire for death and demands that staff directly intervene to prevent patients from carrying out suicidal acts. Systems are generally not designed to prevent deliberate sabotage. For example, the best-designed cockpit control system cannot prevent a pilot from deliberately crashing a plane. Thus, suicide prevention presents unique challenges from the human factors perspective.
Errors in Medical Practice
In 1997, Louis Harris and Associates conducted a nationwide public opinion survey regarding patient safety.15 The public believed that careful, competent providers do not and should not make errors and that only bad providers make mistakes and hurt patients. The public thought that preventable adverse events could be fixed or improved by keeping bad providers from providing care and by improving oversight and training of individual providers. Hence, the general societal response to adverse events has been to punish health providers through malpractice or licensing litigation.
In contrast, the IOM, based primarily on the work of Dr. Lucian Leape, recommended a different approach: medical errors can best be reduced by improving systems, not by focusing on individual provider errors.1 In a series of classic papers, Leape counseled physicians that in medical practice, “Errors must be accepted as evidence of systems flaws not character flaws” (Ref. 16, p 1857). Medical systems design must respect the limits of human functioning.17,18 Jobs should be designed with standardized work processes. Reliance on vigilance and memory should be avoided. Key processes should be simplified.19 Most human errors in complex systems are related to system defects and can be avoided through system modifications.
Based on the work of James Reason,20 the IOM report defined an error as either “the failure of a planned action to be completed as intended (i.e., error of execution) or the use of a wrong plan to achieve an aim (i.e., error of planning)” (Ref. 1, p 28). An adverse event is defined as “an injury caused by medical management,” and an adverse event attributable to error is a “preventable adverse event” (Ref. 1, p 28). The IOM also recommended that preventable adverse event data be collected, analyzed, and shared to improve general medical practice.
The IOM suggested a two-pronged approach to error reporting, with both a mandatory and a voluntary reporting component. A mandatory, public reporting component would hold health care organizations and professionals accountable for serious errors. A voluntary, confidential reporting component would allow health care organizations to report less serious errors and near misses. Both components would encourage organizations to think about how to improve systems to avoid future errors and would encourage analysis to prevent future errors.1 Presumably, such data would then be shared across systems.
The IOM also recommended that Congress pass legislation to extend peer review confidentiality protections to patient safety and quality improvement data that are collected by health care systems and that are shared with others for improving patient care.1 Congress attempted to pass the Patient Protection Act of 1998, which would have provided peer review privilege at the federal level for information shared with accrediting bodies.21 The bill passed in the House but failed in the Senate. Subsequent attempts to pass similar legislation have also failed. Instead, a patchwork of state statutory and case law governs peer review confidentiality and privilege protection. Moreover, a series of federal court appellate rulings has required that state psychiatric hospitals turn over peer review documents, thought to be protected by state law privilege, to plaintiffs during federal cases alleging civil rights violations.22 These difficulties make sharing of information between health care organizations and outside entities problematic. Health care organizations cannot predict in advance whether such sharing might breach state law peer review, confidentiality, or privilege protections.
Currently the Joint Commission is probably the best source of national information on preventable adverse events. The Joint Commission defines a sentinel event as “an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof.”23 A reviewable sentinel event occurs when the event “resulted in an unanticipated death or major permanent loss of function, not related to the natural course of the patient's illness or underlying condition.”23 Certain sentinel events are always reviewable, including suicide in an around-the-clock care setting.23
The goal of the Joint Commission's policy is to improve practice by requiring that institutional leadership respond to sentinel events with a root cause analysis and an action plan. Following the recommendations of the IOM and Leape, a root cause analysis focuses primarily on systems and processes and does not attempt to focus blame or liability on a specific individual. The institution's action plan, based on the root cause analysis, outlines how the institution will modify systems and processes to minimize the risk of future sentinel events. Institutional leadership must report the root cause analysis and action plan for all sentinel events to the Joint Commission.
This reporting requirement could improve knowledge outside the reporting institution.23 The Joint Commission analyzes the reported data and publishes recommendations for improvements in general health care practices. However, the Joint Commission's sentinel event policy precludes the sharing of event-level data outside of itself, to maintain the confidentiality of the reporting organizations and the patients involved (personal communication, Peter B. Angood, MD, Vice President and Chief Patient Safety Officer, Joint Commission, 2008). Researchers outside the Joint Commission can rely only on data that it publishes in aggregate and cannot obtain access even to de-identified data to perform their own analyses and reach their own conclusions.
Inpatient Suicide
The Joint Commission has published one Sentinel Event Alert on inpatient suicide, in 1998.24 That alert reviewed 65 cases of completed inpatient suicides and the associated root cause analyses reported to the Joint Commission between 1995 and 1998. Reporting facilities included psychiatric hospitals (where 52% of the suicides occurred), medical hospitals, and residential care facilities. Root cause analyses found both environmental and staff-related factors, with incomplete or infrequent patient observation commonly cited as causative factors. Risk reduction strategies included updating institutional policies and procedures for patient observations. The Joint Commission emphasized the need for around-the-clock observation for inpatients assessed as being at high risk for suicide. It did not, however, define how adequate around-the-clock observation should be implemented.
Inpatient suicides reported as sentinel events to the Joint Commission have remained fairly steady from 1999 through 2007, varying from 40 to 72 incidents per year.25 The numbers, however, include both inpatient suicides and suicides that occurred within 72 hours of discharge. The Joint Commission has not reported how many of the inpatient suicides occurred while the patient was on intermittent or continuous observation.26
In its latest publication, which highlighted nurses’ roles in sentinel event prevention, the Joint Commission focused attention on sentinel event prevention strategies for inpatient suicide devised through root cause analysis.26 Unfortunately, it has tended to highlight individual nursing errors. When system solutions have been proposed, recommendations usually have been general, without reference to specific best practices found across organizations. For example, when a problem with patient observation level was determined to be a root cause of a suicide, recommendations included the admonition to “help ensure implementation of the appropriate observation level” (Ref. 26, p 127). The authors did not discuss how systems could be put into place to aid staff in attaining an appropriate observation level.
The American Psychiatric Association's “Practice Guideline for the Assessment and Treatment of Patients with Suicidal Behaviors” reviewed the literature and made multiple recommendations for best practices regarding suicidal patients.27 The guidelines emphasized that for inpatient practice, the level of suicide precautions must be based on an adequate risk assessment and a clinical rationale. However, there was no discussion of how to implement and carry out observation practices appropriately on inpatient psychiatric units.
Epidemiology: Inpatient Suicide and Observation
There are only a few studies in which epidemiological data have been collected on inpatient suicides with data on observation practices included. No research groups have looked exclusively at suicides that occurred on inpatient units. All studies have also included suicides that occurred when inpatients were on allowed passes, after elopements, and after inpatient discharges. None of the studies was designed specifically to improve inpatient observation practices.
Martin28 studied completed inpatient suicides at a single Canadian inpatient psychiatric facility. The cohort consisted of over 30,000 patients monitored for more than 30 years. There were five suicides while patients were on the ward, with one ward patient on continuous observation at the time of the suicide.
Gournay and Bowers29 reviewed 12 cases of inpatient suicide across England, which were referred to the authors for expert opinion in the context of legal actions against hospitals or physicians. Six of the suicides occurred while the patients were on some kind of continuous observation level. Staff shortage was a clear contributing factor in two of the suicides. Death occurred in seven cases because nursing staff, for one reason or another, did not adhere to the instruction, with the patient committing the act while out of sight of the nurse. Unfortunately, the authors did not discuss how systems defects might have contributed to these events.
Busch et al.30 reviewed the charts of 76 patients who had committed suicide in the hospital or immediately after discharge from a variety of community, teaching, and state hospitals. Fifty-seven patients were on an inpatient unit at the time of the suicide, and of those, researchers were able to determine observation levels for only 45 patients. Four patients were on one-to-one observation, 28 were on intermittent observation, and 13 were on no observation at the time of their suicides. The authors did not describe how those patients on one-to-one observation were able to commit suicide.
Dong et al.31 used coroners’ data to examine inpatient suicides in Hong Kong in a case-control study. All public hospitals in Hong Kong participated in the study (there were no private psychiatric hospitals in Hong Kong during the study period). Ninety-three inpatient suicides were identified. Seventy-five of the inpatients were on authorized leave and 12 patients were on unauthorized leave at the time of the suicide, leaving only 6 patients on inpatient wards at the time of the suicide. Three of the six ward patients were on continuous observation at the time of the suicide.
Meehan et al.32 collected coroners’ data from England and Wales on all deaths ruled suicide or undetermined cause from April 1, 1996, through March 31, 2000. Researchers then determined which patients had had mental health contacts within one year of the suicide. They sent these patients’ consultant psychiatrists a questionnaire covering demographic data, clinical data, and details of the suicide. Five hundred ninety-five inpatients committed suicide, 236 of them while on inpatient units (the remainder of the patients either were on leave, were off ward with staff agreement, or had eloped). Seventeen patients died while on one-to-one observation, and 139 died while on intermittent observation. Seventy-four of the patients who died had eloped from the hospital while on either one-to-one or intermittent observation. The authors did not describe how the patients under observation were able to commit suicide on the ward or were able to elope. Hanging was by far the most frequent suicide method used by inpatients.
The language used to describe observation practices and procedures has not been standardized in the literature or even in the same health system. The literature shows that wide varieties of terminology for different levels of observation are used at different facilities (Table 1). A distinction must be made between intermittent and constant observation. Constant observation must be refined further. For example, the language should describe whether one nurse can observe more than one patient continuously, whether the observation can be line-of-sight but at some distance or within arm's length, and whether staff must observe the patient while the patient uses the toilet or shower. Sometimes the same term may mean intermittent observation in one facility and constant observation in another. This nonuniform terminology makes it particularly difficult for physicians, nurses, and other health care team members to apply observation policy consistently when they change practice settings.
Terminology Used for Inpatient Observation Levels Across Health Care Systems
Doughty,47 a researcher with the Suicide Working Group of the New Zealand Guidelines Group, identified studies that assessed best practices for inpatient seclusion and patient observation. She employed a systematic search strategy of multiple medical and psychological databases. Inclusion criteria included English language studies from 1990 to 2002 that collected data for patients placed in seclusion or placed under observation for suicide risk. One hundred forty-seven papers were initially identified. Only one paper met final inclusion criteria. That study was assessed to be of poor quality, as it did not use standard case-control methodology.
There were 12 papers that described psychiatric observation practices by using a variety of qualitative methods. Common themes were:
Staff tended not to follow observation policies and covertly modified observation practice without discussion among the treatment team.3,4,40–42,48
Observation terminology and practice varied widely, even in the same health system, and were not uniform in the same facility across shifts and units. Personnel in the same facility had very different perceptions of purposes and procedures for observation.37,41–43,49,50
Observation was considered a low-level task that was not clinically useful.5,6,42,48
Observation practices can empower3,4 or disempower nurses.5,6
Standardizing and Improving Psychiatric Observation Practices
I became interested in inpatient suicide and observation practices both through my clinical practice, in which I am attending physician on an inpatient psychiatric unit at The Johns Hopkins Hospital, and through my forensic practice in which I am asked to review cases of inpatient suicide. A significant decrease in the use of seclusion and restraint on our unit appeared to correlate with an increase in the use of constant observation. Observation practices in the forensic cases I reviewed varied widely. After I reviewed the literature and found no good published practice standards existed for observation, I thought it would be useful to look at data where a failure of observation practice was found to be a root cause of inpatient suicide. I contacted the Joint Commission and asked the agency to consider sharing event level data of the root cause analyses and action plans they had collected for inpatient suicides. I intended to review the data and to use expert panels to devise best observation practices. The Joint Commission refused to release even redacted event level data because of confidentiality and privilege concerns. I then looked for other methodologies.
Unlike root cause analysis, which is used after an adverse event occurs, failure modes and effects analysis (FMEA) is used proactively to identify and prevent human process errors before they occur. Teams familiar with the process being studied describe process steps, failure modes (what could go wrong), failure causes (what could cause the failure to happen), and failure effects (what would happen if the failure occurred). Probabilities of occurrence (5 = very common), detection (5 = remote likelihood of detection), and severity (5 = high) are assigned through team consensus for each failure mode. Risk priority numbers (RPNs) for each failure mode are calculated by multiplying the scores. Improvement efforts can then focus on the failure modes with the highest RPNs.51 A detailed, step-by-step method for performing the FMEA can be found at the Institute for Health Care Improvement web site.52
FMEA is well suited to describe and improve psychiatric observation practices, which involve multiple human process steps, each vulnerable to error. Knowledge derived from such analyses on a single nursing unit can migrate across other nursing units at the same institution and then across health care systems. The Institute for Health Care Improvement also provides a tool to aid in FMEA development, and allows individuals to share their FMEA analyses on the Web.53
The treatment team on my psychiatric nursing unit at The Johns Hopkins Hospital performed an FMEA analysis of the unit's observation practices. The nursing unit cares for 22 voluntary and involuntary patients, largely admitted from the impoverished community surrounding the hospital. The average length of stay for patients on the unit was 6.8 days for fiscal year 2008. Nurses on the unit follow a professional practice model, in which nurses agree to provide patient care on the unit in exchange for unit self-management. Nurses take the initiative to improve patient care. Physicians, nurses, staff nursing assistants, and agency nursing assistants all may act as patient observers. The nurse in charge of each shift has the authority to call a nursing agency for extra agency nurse observers when needed.
Johns Hopkins Psychiatry has one level of intermittent observation and three levels of continuous observation. The physician, in consultation with the patient's nurse, decides and orders which level of observation is appropriate. Physicians assess the need for observation and the appropriate observation level at least twice a day, and registered nurses assess the level at least twice a shift. Any staff member may initiate or increase an observation level in an emergency, but only physicians may decrease or terminate an observation order. Patients’ family members may not act as observers.
During Q 15-minute checks, the intermittent observation level, the patient's presence, and safety are assessed every 15 minutes.
During constant observation, one observer may observe more than one patient. Staff providing constant observation must keep the patient in constant view, unless modified by physician order to exclude toileting.
Patients who require a higher level of observation are placed on one-to-one accompaniment (1:1). During 1:1, one staff member must remain within close proximity of the patient at all times, with no physical barriers between the patient and staff member.
Patients requiring the highest level of observation are placed on intensive psychiatric observation (IPO). IPO, used very infrequently, is an intense direct observation requiring staff to keep their eyes on the patient and remain within arms reach of the patient at all times in an adequately lighted area. Only nursing staff and staff nursing assistants may assume this level of observation. Assigned staff may have no other responsibilities (including reading and charting), except for observation of the patient. IPO must continue during all patient activities, including direct observation during the patient's hygiene and toileting activities.
A security detail may also be assigned to patients on all observation levels who are a risk for seriously injuring staff or other patients. Security personnel may not perform independent observation of the patient, but may assist the observer and protect the observer and other patients.
A quality assurance professional trained in FMEA facilitated the entire process. The facilitator spent time on our unit taking note of our observation practices. A small group of clinicians then identified 42 observation process steps. These steps were then combined into larger process groups of ordering, observation, observer activities, assessment, and handoffs. A larger clinical group then identified 91 potential failure modes. The groups included participants from all levels of the treatment team, including senior and junior physicians, nurses, and experienced staff nursing assistants who carried out the majority of actual observation across all three nursing shifts. The nursing assistants’ participation was critical in determining potential failure modes, which we discovered varied across day, evening, and night nursing shifts due to variations in practice. Failure modes that had combined high scores for severity (high), frequency (very common), and detection (remote likelihood of detection) were identified as potential critical observation process failures.
Most critical observation failure modes were caused by communication failures between physicians, nurses, and observers. The team identified causes of these potential communication failure modes, which included: nursing workflow interfering with regular communication with the observer; inconsistent observer comfort in communicating changes in patient behavior to nursing staff; inconsistent level of observer engagement with the patient and the treatment team; inconsistent nurse-observer interaction over a shift; unclear documentation requirement for the observer; and inconsistent nurse-observer expectations.
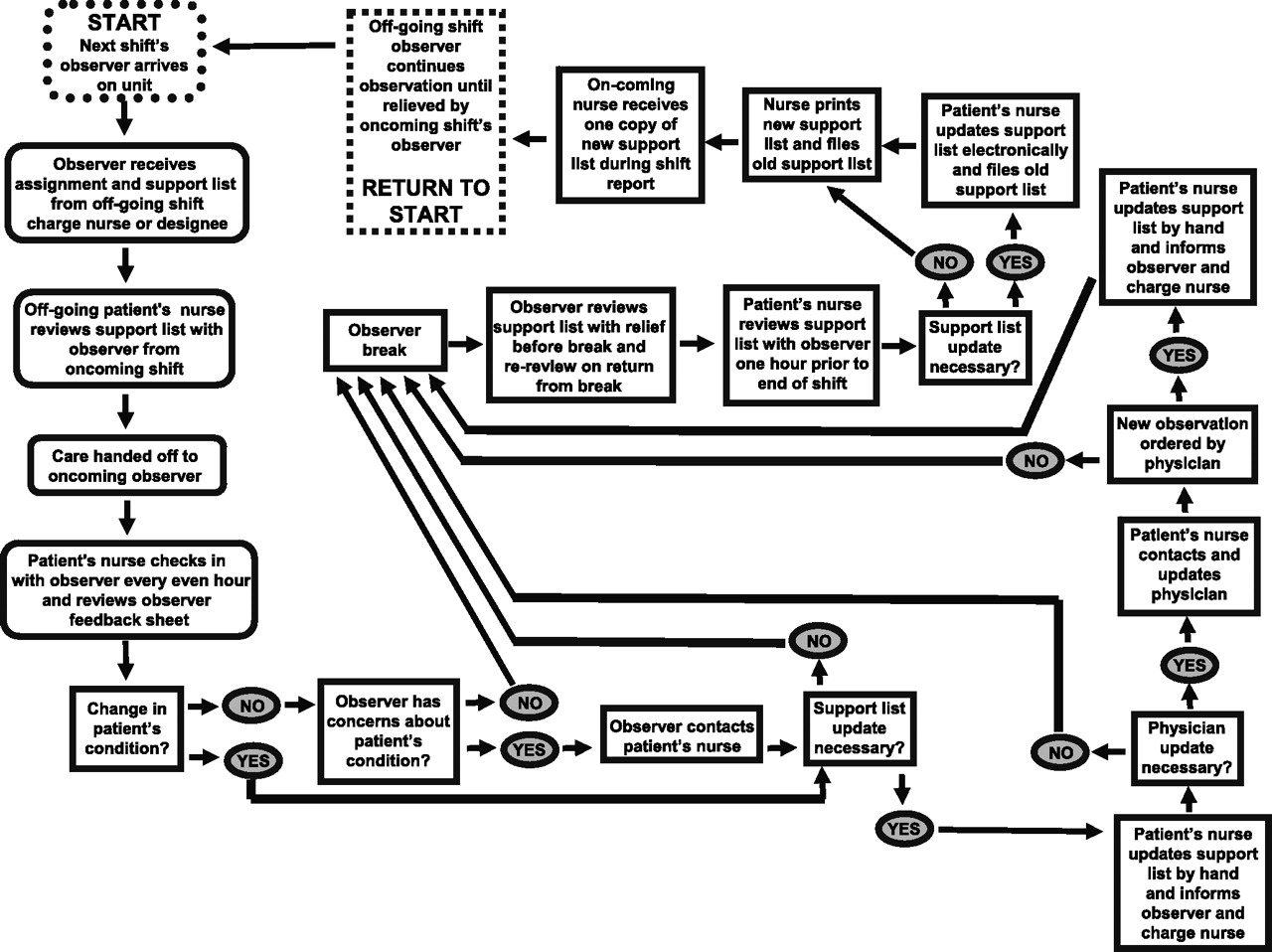
Solutions adopted and piloted included documentation and improvement of nursing-observer-physician workflow for every shift, empowering the observer by developing an observer feedback form that allows observers to document and review behavioral observations of their patient with the patient's nurse every shift, and modification of an existing support list for observer and nursing use (Fig. 1).
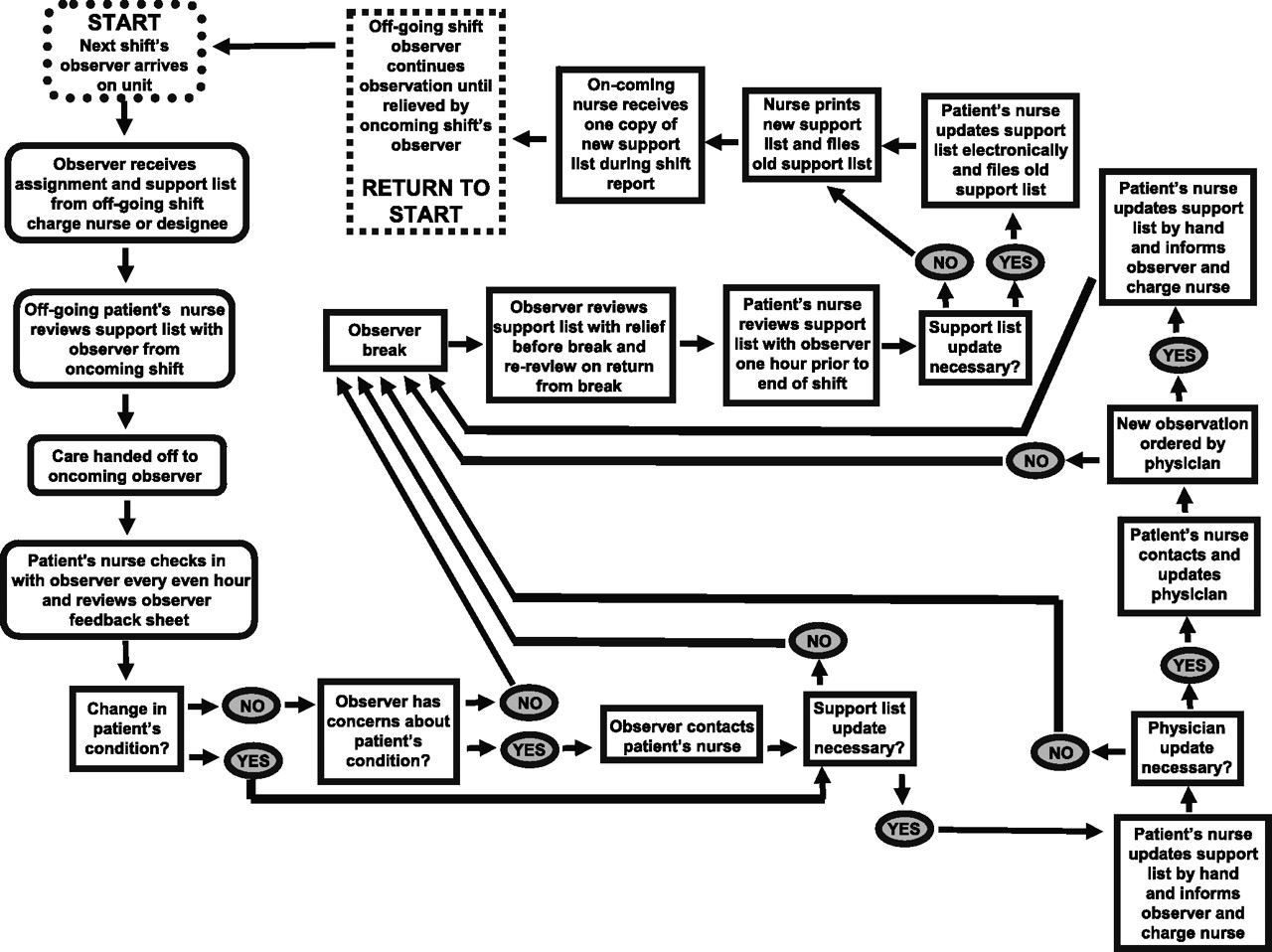
Ideal observation workflow.
The observer feedback form allows the observer to document any inappropriate behaviors or symptoms the patient is experiencing, what helped to improve those behaviors, and what did not work. For example, one patient with paranoid symptoms who was on constant observation was noted by her observer to be “…in dayroom for dinner. Got agitated. Stated people were watching her.” The observer found that the patient's agitation could be effectively reduced: “Redirected to alcove by her room to eat alone.”
At the beginning of every shift, the nurse reviews the support list with the observer. Nurses check in with the observer every other hour and review patient behavior and the observer feedback form. The observer support list includes the patient's current observation level, whether the patient's bathroom door is to be open or closed, the patient's symptoms or behaviors, what the observer needs to do to help the patient, and when the observer should contact the patient's nurse. Support list entries for a typical patient can be found in Table 2.
Typical Patient Support List Entries
Nurses, with observer input, update the support list at the end of every nursing shift. Formal handoffs occur when an observer takes a break and at every shift change. Physicians review the patient's observation status with the treatment team twice daily. Nurses contact physicians whenever there is a significant change in the patient's condition.
We also identified unclear physician or nurse decision-making regarding when to start or stop constant observation as another critical observation failure mode. We chose not to address the problem directly in our current FMEA improvement process. A major unanswered question is at what point a particular patient should be placed on constant, intermittent, or no observation. An inpatient with psychotic depression who tells her clinician that she intends to commit suicide on the unit, has delusions that she is a horrible person, and has a high-lethality inpatient suicide plan should certainly be placed on some type of constant observation. The hard cases are the gray-area ones, patients who are at only medium inpatient suicide risk or patients previously at high risk who are now improving. There are no agreed upon best practices and no research data that provide clinicians with the necessary information to determine at what point these patients should be moved from constant to intermittent to no observation. Physicians and nurses must rely entirely on clinical judgment to make these decisions.
Conclusions
Human factors analysis through FMEA gives every psychiatric inpatient treatment team the tools to map out processes, to discover potential critical errors, and to find best-practice improvements for their own institution's psychiatric observation practices. Our group created clear expectations for constant observation processes, communicated those expectations to the treatment team, and considered other failure modes for improvement.
To avoid error and to foster discussion about best practices, I recommend standardization of the terminology used for observation status. Terms for observation status should immediately reflect, to anyone, whether the patient is being intermittently or continuously observed. I suggest that any observation status where the patient is being continuously watched be termed constant observation, and that any observation status where the patient is being checked at some interval be termed intermittent observation.
At my own institution, the FMEA process itself made it clear that clinical leadership was interested in obtaining information and clinical improvement ideas from all levels of the treatment team. Observation of patients was identified as the crucial element in the safekeeping of inpatients at risk for suicide, and clinical staff at all levels were empowered to improve the process. Our analysis of observation practices found that most potential critical process failures revolved around possible miscommunications and handoff problems between staff members. Other institutions may find similar or different potential critical process failures. Only by sharing detailed process improvement data across institutions can our field come to a consensus about best observation practices.
Although inpatient suicide has been the second most frequent sentinel event reported to the Joint Commission, the actual number of inpatient suicides is small, and the number of patients who commit suicide while on constant observation is even smaller. Given these very small numbers, it is impossible for any one institution to detect whether specific changes in observation practice are effective in decreasing the actual inpatient suicide rate. Concerns over confidentiality make it impossible for the Joint Commission to share root cause analysis event-level data with interested clinicians outside of the Joint Commission. In contrast, FMEA risk reduction strategies and actions can be discussed and shared in detail across institutions without such concerns. Collection and implementation of specific and effective observation risk reduction strategies across health care systems will be necessary to discover best observation practices and to reduce inpatient suicide.
As a next step, we intend to begin discussion of a methodology, other than clinical judgment, to determine at what point an inpatient should be placed on or removed from intermittent or constant observation. Similar discussions should occur at psychiatric institutions and accrediting and regulatory agencies across the United States.
Acknowledgments
The author wishes to acknowledge the substantial support provided by Hilary Sporney, QTIL, who facilitated the FMEA analysis; Geetha Jayaram, MD, MBA, physician advisor for psychiatric risk management at The Johns Hopkins Hospital; Patricia Sullivan, RN, MS nurse manager; Karin Taylor, RN, MS, APRN-PMH Clinical Nurse Specialist; and the entire Meyer 3 Johns Hopkins Hospital nursing and nursing assistant staff.
- American Academy of Psychiatry and the Law





{kind=link}