


Suicide deaths in jails and prisons have been a focus of concern and litigation for several decades. The 1980 Fifth Circuit Court of Appeals case Ruiz v. Estelle1 mandated that correctional facilities screen for inmates at risk of suicide and offer treatment for them. The main accreditation agency for correctional facilities, the National Commission for Correctional Health Care, requires facilities to have a suicide prevention program as an essential element for accreditation. More recently, the International Association for Suicide Prevention formed an international Task Force focused on the prevention of suicide in prison. The Task Force published a suicide prevention guideline in 2007 that outlined the key components of a model suicide prevention program.2 The key components of this program were training, screening, observation, communication, modification of the physical environment, and mental health treatment.
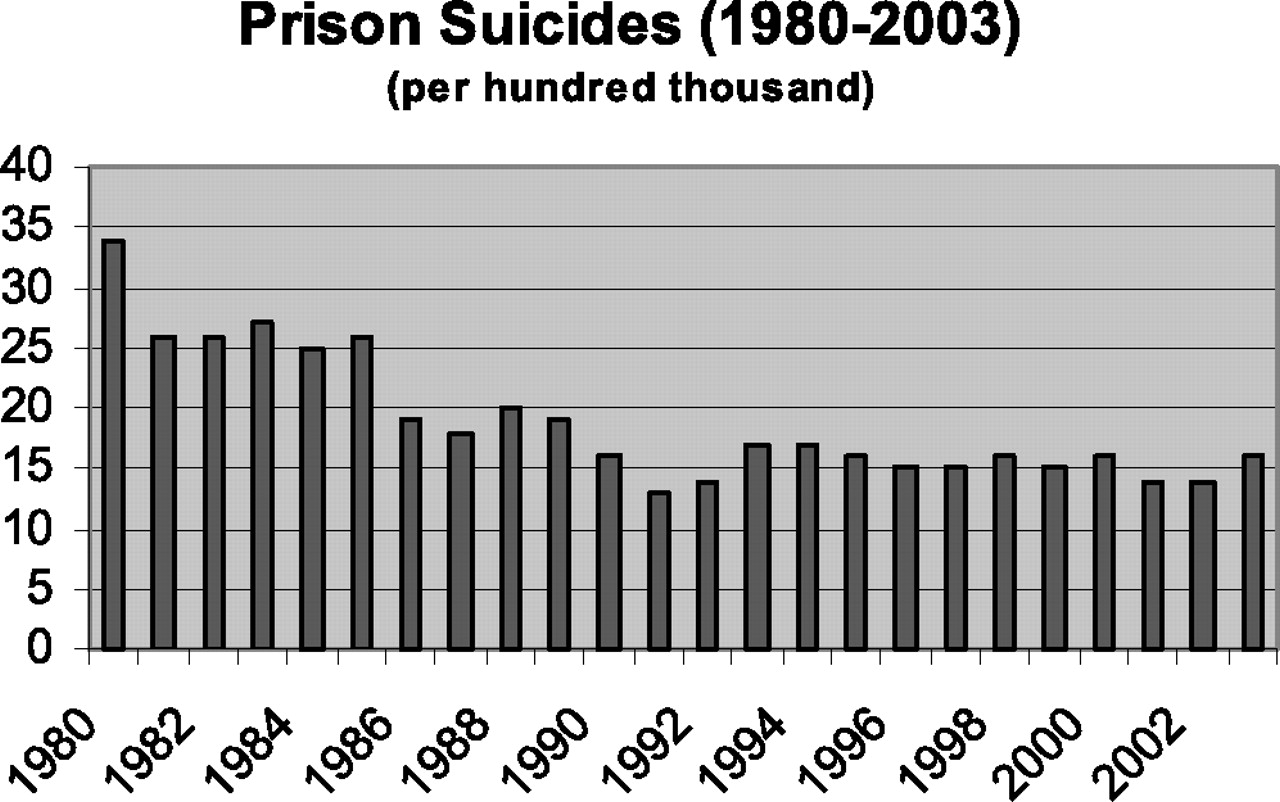
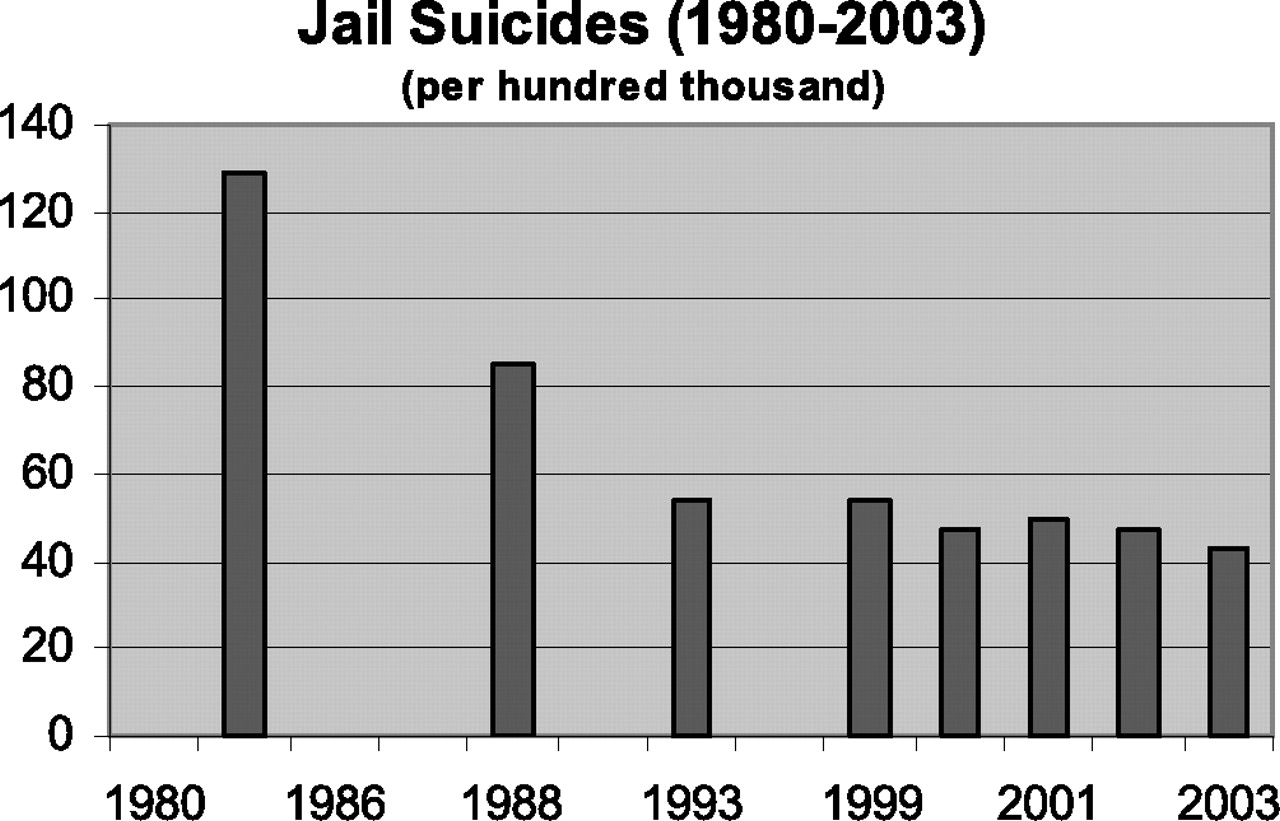
These measures have been effective. Correctional suicide rates decreased by over 50 percent in the years following the Ruiz decision. Between 1983 and 1999, the rate of suicides in American jails dropped to 54 per 100,000 from 129 per 100,000. The suicide rate in prisons decreased to 15 per 100,000 from 27 per 100,000 over the same time period. This reduction is particularly impressive, given the high patient volume and multiple complicating diagnoses found in the average correctional clinic.
However, recent data from the Bureau of Justice Statistics suggest that we may be reaching a point of diminishing progress in suicide prevention. As Figure 1 shows, the rate of jail suicides has remained fairly constant at around 47 per 100,000 since 2000. Similarly, the prison suicide rate appears to have stabilized at around 15 per 100,000, a rate only slightly higher than the national average of 11 per 100,000 over the same time period (Fig. 2 ).
There are many factors that may be involved in the failure to reduce suicide rates further, but one may be the passage of the Prison Litigation Reform Act (PLRA) in 1996. Adopted as an amendment to an appropriations bill, the intent of the PLRA was to curb frivolous pro se suits filed by prisoners. It required proof of indigence to waive filing fees and banned additional suits by inmates who were found to file repeated, baseless claims. The PLRA also had implications for class action reform.3 The law required that any corrective action ordered by the court be limited in scope, addressing only the civil rights violation. Courts were also required to consider the impact that the corrections would have on public safety and the burden that would be placed on the criminal justice system. The PLRA allowed defendants to request immediate termination of any consent decree if these criteria were not met. Correctional systems, some of which had been under judicial supervision for decades, quickly moved to terminate their consent decrees. In addition to ending old litigation, the PLRA has had a chilling effect on new constitutional claims. Between 2000 and 2007, the number of federal claims based on deficient prison conditions dropped by 31 percent (Fig. 3 ).
The era of court-mandated mental health care reform is ending just as the cost of health care provision is rising. The total correctional health care dollar is being stretched to cover organ transplantation, renal dialysis, end-of-life care, hepatitis C treatment, and other expensive medical services, in addition to mental health care. Specific data are lacking regarding the costs of psychotropic medication and other mental health expenses in correctional health care, but it is likely that increasing use of atypical antipsychotic medication has added as much to the cost of correctional health care as it has to the cost of the public mental health system. Without continued judicial oversight and intervention, state correctional systems are unlikely to keep up with these rising costs. The effect on future suicide rates remains to be seen.
Recent research also highlights a change in the characteristics of prisoners who commit suicide. In the June issue of the Journal, a study of suicides in the Texas prison system by Baillargeon et al.4 documented that half of the prisoners who committed suicide had no known history of psychiatric illness, a significant increase from the number of incidents in previous studies of correctional suicide. A 1978 study of suicide deaths in the New York prison system showed that only about one-quarter of the prisoners had no known psychiatric history.5 Similarly, He et al.6 found that in 1996, about one-quarter of the suicide deaths were by prisoners without known mental illness. There appears to have been an increase in suicide deaths committed by previously healthy prisoners.
It is possible that these inmates were not recognized as mentally ill at intake and that they represent false-negative results in mental health screening. Intake screeners are usually not trained mental health professionals, and inmates who are fearful of stigma or harassment may withhold pertinent psychiatric history. However, these possibilities do not fully explain the apparent increase in negatively screened suicides over the past 10 years. It is unlikely that mental health screeners have become less accurate over the years, given the emphasis that has been placed on suicide prevention and the liability risks associated with completed suicide. Other explanations should be considered.
A possible cause of the increase in “clean” suicides (suicides among prisoners with no prior psychiatric history) is that our current suicide prevention efforts have been effective in identifying and preventing the deaths of inmates with known disease. Clean suicides are committed by prisoners who experience their first episode of mental illness after incarceration. This finding is not surprising, given that first episodes of many psychiatric disorders occur in the young adult age group, the most common age among prison inmates. Also, life stressors such as incarceration, job loss, divorce, or the death of a spouse can precipitate first episodes of affective disorder. We have no systematic, policy-driven means of identifying newly affected prisoners at the onset of disease. Our current suicide prevention policies should be modified to address this deficit.
The field of public health provides a framework for understanding disease prevention efforts. These efforts are classified as primary, secondary, or tertiary interventions. With regard to the prevention of suicide, most early prevention efforts are tertiary interventions—measures used to prevent mortality after an actual suicide attempt. One example of a tertiary intervention is training all custody and civilian staff in cardiopulmonary resuscitation (CPR). Another example is requiring each tier in a facility to have a tool available to assist staff in rescuing a prisoner who attempts suicide by hanging. Morbidity and mortality conferences are tertiary interventions in the sense that they are held following an inmate suicide to complete a root-cause analysis of the death. Finally, many facilities have crisis debriefing sessions with responding staff and inmates after a suicide death, to address mental health concerns that arise after the fact.
Secondary prevention efforts are designed to intervene early in the disease process to prevent future complications. As this pertains to suicide prevention, the goal of a secondary intervention would be to identify and treat mentally ill, at-risk prisoners to prevent a suicide attempt. Examples of secondary suicide prevention are the use of screening tools to identify affected inmates at intake and the use of suicide observation for inmates considered high risk. Table 1provides an overview of current suicide prevention measures.
In public health, primary prevention efforts usually involve altering environmental factors associated with disease or taking steps to enhance human resistance to disease. Improved public sanitation and the fluoridation of water are two examples of environmental intervention. Vaccinations and improved nutrition are examples of how human resistance to disease can be improved. Public education is also employed to address behavior that increases the risk of disease and to increase the likelihood that an affected individual will seek treatment. In some cases, new laws are adopted to enforce public health standards.
When applied to correctional suicide, the primary prevention model requires consideration of environmental and individual factors that predispose to suicide and the design of interventions around those risk factors. Several aspects of the correctional environment have been implicated in jail suicides: overcrowding, violence, and institutional unrest. Unfortunately, many of these environmental factors are beyond the control of the individual institutional psychiatrist. It behooves our professional organizations at the state and national level to advocate for humane prison conditions and for institutional clinicians to call attention to the need for improvements.
Correctional clinicians can also advocate for changes in policies or practices that deter prisoners from seeking care or that erect barriers to mental health care. Inmates will be reluctant to seek care if the institution has a policy of denying institutional jobs to inmates who are on psychotropic medications. Some correctional systems deny work release to psychiatric patients. A prisoner on psychotropic medication also may be denied transfer to low-security programs such as home detention or boot camp if on-site psychiatric services are not available, even if the inmate's psychiatric condition is in stable remission. Psychiatric patients are also less likely to be granted parole than are inmates without a mental health history.7 Some inmates are reluctant to seek treatment because they fear they will be transferred to a specialty mental health tier where they will be easily identified as psychiatric patients. In a worst-case scenario, inmates may actually withhold their suicidal ideation completely if an overly aggressive suicide prevention policy requires that they be automatically stripped and placed in a suicide observation cell before mental health assessment. Finally, protective housing should be available on request for vulnerable inmates, such as sex offenders and transgendered prisoners.
Education is an important element in preventing clean suicides. Educating staff and prisoners about mental illness can decrease the stigma of treatment and engender sensitivity to the cultural or ethnic barriers that affect the decision to seek mental health care. Staff awareness will improve case identification, since correctional officers have around-the-clock contact with prisoners and substantial opportunity to observe inmates who may be symptomatic. Case identification can also be improved by teaching inmates about the symptoms of clinical depression and about available treatments. Prisoners should be encouraged to seek care for themselves and to refer cellmates who appear troubled. Cellmate referral is a form of the “buddy system” of suicide prevention, which has been used in military and juvenile suicide prevention programs to improve case identification.8 Institutional libraries should contain materials about matters related to mental health written in language that is accessible to the average inmate. Finally, for prisoners serving long felony sentences, most facilities have a policy that requires an annual physical. Screening tools such as a general health questionnaire and the Prime-MD survey9 can be employed by somatic physicians to identify new cases of mental illness during routine health care appointments.
In addition to formal psychiatric screening tools, correctional clinicians can expand their assessments of suicide risk to include factors related to personal safety and vulnerability. Drug use or the presence of gambling debts may make inmates vulnerable to threats and intimidation by their peers. Gang activity is becoming an increasing risk factor for violence in prisons and may lead to inmate suicide. Inmates who are pressured to join a gang or to participate in gang-run contraband activities, may choose to commit suicide if they feel the institution cannot provide sufficient protection. Prison patients can be asked general questions regarding their relationships with cellmates and officers and about their perceptions of overall safety within the facility. With the patient's permission, this information can be transmitted to institutional security staff. Examples of safety and vulnerability questions are presented in Table 2.
Clinician prescribing practices can make inmates vulnerable to their peers.10 Sedating medications, such as tricyclic antidepressants, are valued both for the treatment of insomnia and for treatment of opiate withdrawal symptoms. Stimulants prescribed for attention deficit disorder are valued among inmates for their abuse potential. Psychiatric patients who are prescribed these medications are at risk of being threatened by other inmates who want to obtain them. Use of the less sedating serotonin reuptake inhibitors or atypical neuroleptics can circumvent this problem. Close regulation of psychotropic medications through watch-take procedures or liquid medication can also prevent such abuse.
In summary, the increasing number of clean suicide deaths requires a change in current suicide prevention policies. Prevention can be improved by addressing environmental threats to the inmate and assessing the inmate's level of vulnerability and by modifying clinical practice to protect the inmate from peer intimidation.

Prison suicide rates since Ruiz v. Estelle.
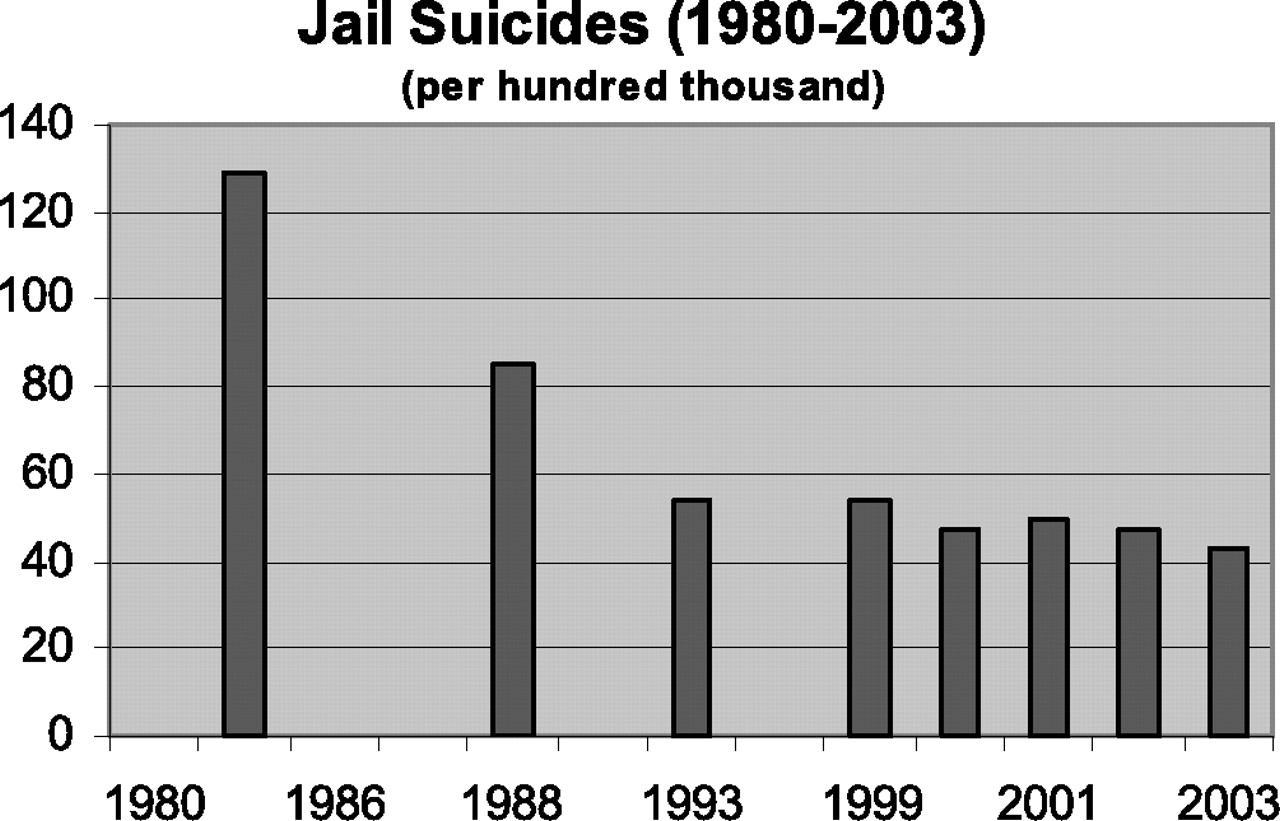
Jail suicide rates since Ruiz v. Estelle.
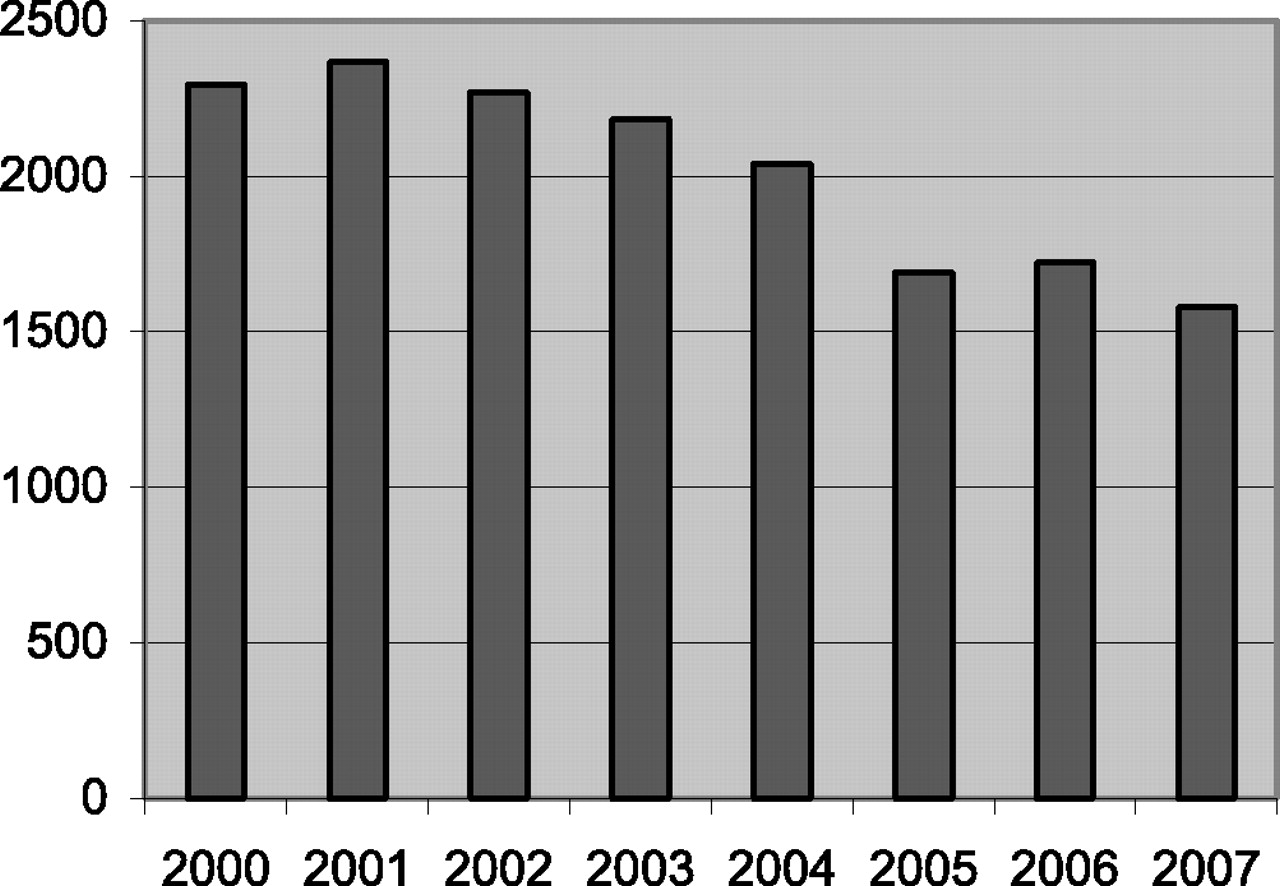
Federal claims based on prison conditions (Administrative Office of the U.S. Courts).
Public Health Interventions for Suicide Management
Sample Environmental Safety and Inmate Vulnerability Questions
Footnotes
-
Disclosures of financial or other potential conflicts of interest: None.
- American Academy of Psychiatry and the Law





{kind=link}
{kind=link}
{kind=link}