


Abstract
Clinical information on parricidal offenders has accumulated in recent decades. The purpose of this study was to examine and compare the mortality of matricidal and patricidal offenders in detail by using a comprehensive national data set with follow-up ranging from 3 to 24 years. The sample included forensic psychiatric examination statements and mortality data of 99 matricidal, 113 patricidal, and 111 control male violent offenders evaluated in a forensic psychiatric examination from 1973 to 2004 in Finland. The Standardized Mortality Ratio among parricidal offenders 25 to 49 years of age was increased compared with that of the general population. One-third of deaths among parricidal offenders were attributable to suicide. The matricidal males who committed suicide had a significantly shorter survival time after the offense than did the patricidal and control offenders who died by suicide. The results of the present study are compared with the previous study findings on parricidal offenders and offenders in general.
The association between criminality and excess mortality is a well-documented finding. It has been demonstrated by several research groups with different methods and samples: offenders subject to forensic psychiatric examination,1 severely mentally disordered offenders,2 antisocial offenders,3 prisoners and ex-prisoners,4,5 homicidal offenders,6 habitually violent offenders,7 and delinquent adolescents observed up to 65 years of age.8 For example, researchers in a recent large-scale epidemiologic study found that the standardized mortality ratio (SMR) was 3.7 among males with a history of imprisonment compared with the population at large.9 High offender mortality has been particularly associated with deaths of substance-related causes and of unnatural causes, such as suicides and accidents.1,9–11
Parricide (i.e., the killing of a parent by his or her child) is an infrequent form of domestic violence offense predominantly committed by sons.12–16 Because of the distribution of parricidal offenders between the sexes, study samples include almost solely male offenders. Those who have attempted parricide are often included in the samples, too, as few differences have been found between completed and attempted parricides.14,17 Previous studies have reported a high prevalence of severe mental disorders among parricidal offenders.12–15,17–20 However, the background factors of parricidal offenses are multifactorial, often featuring a chronically disturbed relationship between the offender and the victim.13,20–23
Information on the overall mortality of parricidal offenders is limited. In only one study has the mortality rate of parricide offenders been investigated by using the standardized mortality ratio.24 In this study, it was found that, among mentally disordered male parricide offenders discharged from high-security care, the SMR was almost four times that of the general population. It has been suggested that the uniqueness of the relationship between the parricidal offender and the victim may complicate psychological processing of the act by the offender, which may lead to post-offense depression with an increased risk of suicide.13,25 However, there are also indications that adolescent parricide offenders who kill a parent as a consequence of long-term familial abuse by the victim may recover and adjust.26–29 The support given by the rest of the family and a relatively low amount of severe psychiatric impairment improve the long-term coping of adolescent offenders.27–29 Most studies presenting data on the suicidality of parricidal offenders have dealt with suicidal thoughts and attempts before and immediately after the offense. In a study with 64 adult parricidal offenders, 11 percent attempted suicide immediately after the offense. Most of those who attempted suicide were later assessed as not guilty by reason of insanity.17 Among 39 mentally ill adult parricidal offenders, 18 percent attempted suicide before and 5 percent after the offense.14 Of the parricidal offenders in a high-security hospital (n = 55), 19 percent of the adult and 8 percent of the adolescent offenders made suicide attempts before the offense, while 7 and 9 percent of the adult and adolescent offenders, respectively, behaved suicidally after the offense.30 In a study by Green,12 11 (19%) of 58 matricidal offenders attempted suicide soon after the offense, and two completed suicide later while still in the hospital. Among 17 female parricide offenders, three psychotic subjects committed suicide during the period ranging from 1 month to 10 years after the offense; one offender died of natural causes during the follow-up.31
Earlier studies reported more suicide attempts and completed suicides among matricidal offenders than patricidal ones, although this difference has not been systematically studied.12,15,18,19,26 In a study of 15 matricidal offenders, 3 attempted suicide immediately after the offense, and 1 made several attempts during the months following the offense,18 whereas no suicide attempts were registered among 10 mostly schizophrenic patricidal offenders in the same hospital.19 Among 56 parricidal offenders, 15 percent attempted suicide after the offense, and 7 percent ultimately died by suicide.15 In this study, of the total 24 male matricide offenders, 17 percent (4/24) attempted and 13 percent (3/24) committed suicide, whereas there were three (8%) attempts and three (8%) completed suicides among the 37 male patricide offenders. These data include the double-parricide offenders who seemed most liable to display suicidal behavior.
Given the particular relationship between the parricidal offender and the victim, the psychological aspects of these offenses, and the high psychiatric morbidity among the offenders, we were interested in exploring the rate of dying among parricidal offenders. The purpose of this study was to examine mortality rates and causes of deaths among parricidal offenders in a national comprehensive data set with follow-up ranging from 3 to 24 years. First, our purpose was to compare the mortality rates of matricidal and patricidal offenders with each other and with that of the general population of the same age. Second, we investigated the mortality rates of matricidal and patricidal offenders in relation to criminal responsibility. Further, interest was focused on investigating whether matricidal offenders are particularly subject to suicidality because of the greater prevalence of major psychopathology among matricidal offenders and the different underlying dynamics of the offenses. The mortality rate of the parricidal offenders was also contrasted to that of a matched sample of violent offenders whose victims were other than their parents. Mortality rates among the general Finnish male population of the same age were used as a reference as well.
Materials and Methods
This study forms part of a research project on parricidal offenders, with a particular focus on matricidal offenders, comprising information on all males who underwent a forensic psychiatric examination in Finland from 1973 to 2004 subsequent to committing a violent offense against one parent. The established practice in Finland is that a large proportion of all homicidal offenders and others who have committed serious violent offenses undergo a thorough forensic psychiatric examination as a part of a trial procedure.32 The National Authority of Medicolegal Affairs arranges forensic psychiatric examinations at the request of the court. During the past decades, approximately 200 examinations have been conducted each year, mainly on offenders charged with homicides or other serious violent offenses.32,33 The examination is an extensive inpatient psychiatric investigation in special hospital settings lasting a maximum of two months. It contains data collected from various sources, interviews by a multiprofessional team, a comprehensive psychiatric evaluation with diagnostic procedures, standardized psychological tests, examination of the offender's physical condition, and observation of the offender by the hospital staff. The conclusions include diagnoses as well as the assessments of criminal responsibility and the need for psychiatric hospitalization.
In Finland, the minimum age of criminal liability is 15 years. In our study, a violent offense was defined as homicide or attempted homicide, aggravated assault, common assault, robbery, illegal threatening behavior, harassment, arson, or any sexual crime. In cases in which the victim was a stepparent or foster parent, only those were included in which the step- or foster parent had joined the family when the son was under the age of eight years. The 15 subjects who had offended against both parents during the period were excluded, as our purpose was to characterize differences between the offender groups subdivided by the sex of the victim. In this study, the terms matricidal and patricidal are used for all violent offenses against a parent, as the terms matricide and patricide refer only to the cases in which the parent died. The study sample includes 99 matricidal offenders and 113 patricidal offenders. A control group for the patricidal offenders, matched for the violent act, sex, and age of the offender was gathered from the mental state examination report archives (n = 111). Table 1 presents the distribution of the offenses among the offender groups.
Distribution of Offenses Among Matricidal, Patricidal, and Control Offenders Subject to Mental State Examination in Finland from 1973 to 2004
The mean age of the matricidal group (30 years) was significantly higher than that of the patricidal group (27 years, p = .014) and the control group (26 years, p = .002). Six matricidal offenders and six patricidal offenders committed the offense while under the age of 18 years. Forty-two percent of the matricidal offenders, 27 percent of the patricidal offenders, and 17 percent of the control subjects had a psychotic disorder (p < .001), while a personality disorder was diagnosed in 51, 64, and 79 percent of the matricidal, patricidal, and control offenders, respectively (p < .001). Fifty-nine percent of the matricidal offenders, 46 percent of the patricidal offenders, and 69 percent of the control subjects had an alcohol or drug-related disorder as the primary or secondary diagnosis (p = .003).
The forensic psychiatric examination reports of the offenders were retrospectively analyzed for several variables regarding offender and offense characteristics. The background variables used in this study were index offense, age at death, psychiatric diagnosis, and criminal responsibility. Accurate information on all the subjects’ mortality was collected in November 2007 by record linkage with the Cause of Death Register at Statistics Finland, using personal identification numbers assigned to all residents in Finland. All subjects were followed up until the end of November 2007, or earlier in the event of death. The official death register includes personal information on the deceased and the date and cause of death, classified according to the International Classification of Diseases, according to the eighth revision (ICD-8) until 1986,34 ICD-935 between 1987 and 1995, and ICD-1036 from 1996 onward. In this study, the deaths were classified in the following way: natural, unnatural, or unknown; accidental (yes/no); and suicide (yes/no); and method of suicide (hanging, intoxication, or other). In each of the three groups studied, there were two cases without exact information on the cause of death. The number of deaths and the causes were compared with mortality data for the general Finnish population, obtained from Statistics Finland.
The original study protocol was approved by the Ethics Committee of Oulu University Hospital on August 19, 1996. The National Authority of Medicolegal Affairs and the Ministry of Social Affairs and Health and Statistics Finland approved the study. The permission to make a register link to causes of death was obtained from the Cause of Death Register.
The statistical significance of group differences in categorical variables was assessed with the Pearson chi-square test or Fisher's exact test when appropriate, and the differences in continuous variables with Student's t test; p < .05 was defined as the limit of statistical significance. We calculated standardized mortality ratios by comparing the observed number of deaths in the study subjects with the expected number of deaths as predicted by the age- and sex-specific mortality rates of the general population. The result was expressed as the SMR, together with its 95 percent confidence interval (CI). The age-specific SMRs were determined for four age groups (15–24, 25–49, 50–64, and 65–79 years). A Cox proportional hazards model was used to estimate the survival time from the date of offense to the date of death of the groups studied in the subcategories of natural deaths, suicides, and unnatural deaths other than suicide, separately. All data were entered on computer in the SPSS Program for Statistical Analysis.
Results
Mortality
Twenty (20%) of the matricidal, 33 (29%) of the patricidal, and 28 (25%) of the control offenders had died by the end of the follow-up period. Of the deaths with a determined cause (in each offender group, two cases with undetermined causes were excluded), unnatural causes of deaths accounted for 9 (50%) matricidal, 18 (58%) patricidal, and 19 (73%) control offender deaths. No statistically significant differences in mortality were found between the offender groups.
The mean (standard deviation; SD) ages at death among the matricidal, patricidal, and control offenders were 43.4 (13.3), 42.7 (13.4), and 44.5 (11.0) years, respectively. At the end of the follow-up, the mean age (SD) of the live subjects was 47.9 (10.1) years for the matricidal, 46.5 (10.4) years for the patricidal, and 46.1 (10.6) years for the control offenders. The age of the deceased and live subjects did not differ significantly between offender groups. Furthermore, the difference in mean age at death from natural causes of the matricidal (mean, 49.9 years; SD 9.0), patricidal (mean, 50.1 years; SD 14.0), and control (mean, 49.0 years; SD 6.4) offender groups was not significant. In unnatural deaths, however, the age at the time of death was lower in the matricidal offenders (mean, 32.8 years; SD 8.5) than in the control offenders (mean, 39.9 years; SD 6.7; t test, t = −2.40, df = 26, p = .024), but not when compared with that of the patricidal offenders (mean, 37.2 years; SD 10.9).
Standardized Mortality Ratio
All-cause mortality of both the matricidal and patricidal offenders was increased in the 25- to 49-year age group when compared with that in the general Finnish male population of the same age (matricidal: SMR 3.4; 95% CI, 1.9–6.0; patricidal: SMR 3.9; 95% CI, 2.3–6.4). Among the age groups 15 to 24 years, 50 to 64 years, and 65 to 79 years the overall mortality rates were not significantly increased in comparison to the general same-age population.
Mortality and Criminal Responsibility
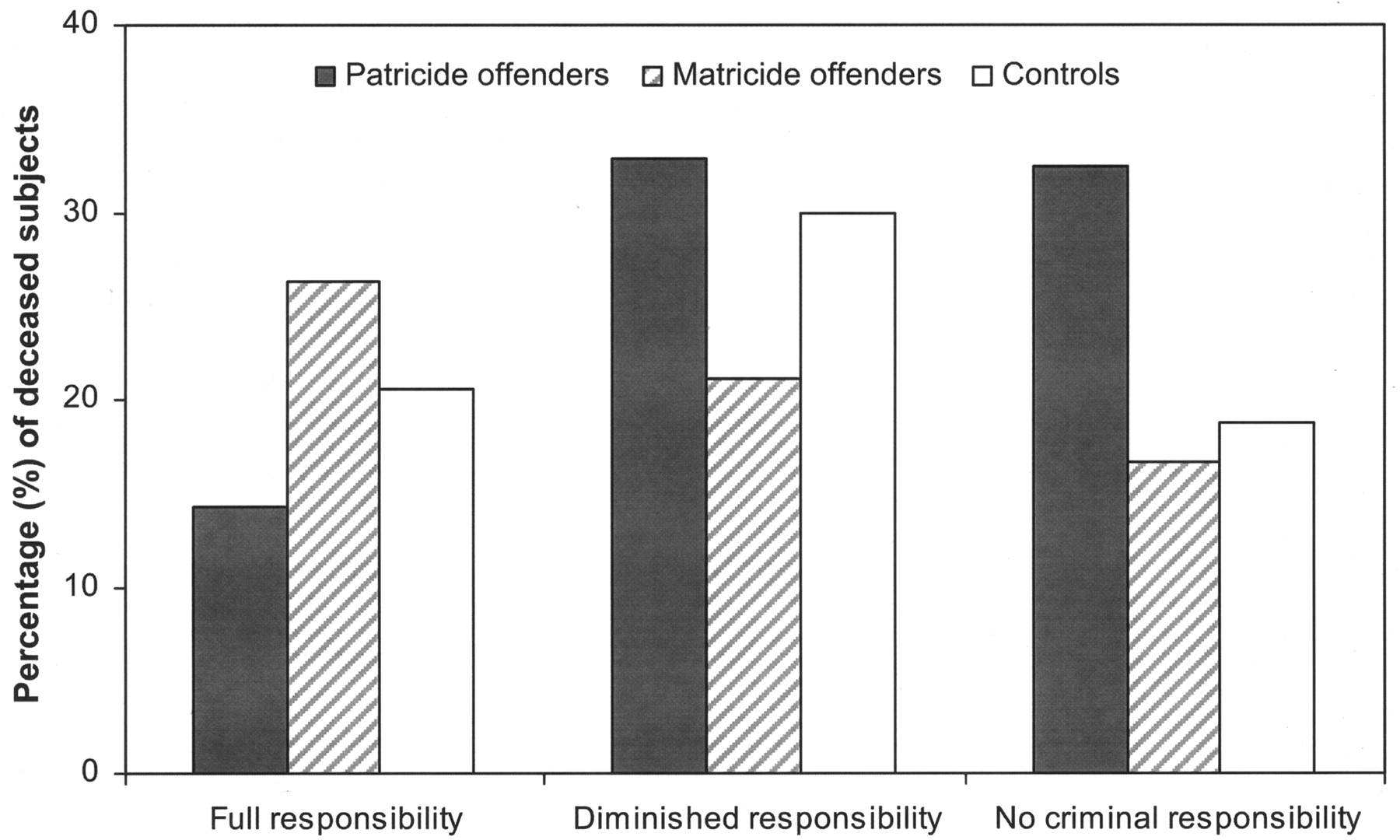
During the follow-up, 26.3 percent of the matricidal and 14.3 percent of the patricidal offenders with full responsibility had died, compared with 21.1 percent of matricidal and 32.8 percent of patricidal offenders with diminished responsibility. The proportions of the dead subjects in the groups defined as not guilty by reason of insanity were 16.7 percent in the matricidal and 32.4 percent in the patricidal groups. Figure 1 illustrates the proportions of deceased subjects in the parricidal offender groups according to criminal responsibility. No statistically significant differences were observed between the offender groups in any category of criminal responsibility.

The proportion of deceased subjects according to criminal responsibility among 99 matricidal, 113 patricidal, and 111 control offenders who underwent a mental state examination in Finland from 1973 to 2004.
Suicide Mortality
Of all unnatural causes of deaths, suicides accounted for six (66.7%) of the matricidal, nine (50.0%) of the patricidal, and five (26.2%) of the control offender deaths. The proportion of suicides among unnatural deaths in the matricidal group was significantly higher than that in the control group (χ2 = 4.169, df = 1, p = .041), but no difference was found when the matricidal offenders were compared with the corresponding patricidal offenders. The age (SD) at death from suicide was 29.6 (8.8) years in the matricidal, 34.1 (10.2) years in the patricidal, and 42.3 (6.9) years in the control offenders. The matricidal offenders were found to be significantly younger at the time of suicide than were the control offenders (t test, t = −2.62, df = 9, p = .028), whereas no age differences were found in other pair-wise comparisons.
Among the matricidal offenders, hanging was the most common method of suicide (50%), but among the patricidal offenders, there were as many suicides by hanging as by intoxication (both 44%). In the control group, most of the suicides were committed by hanging. No statistically significant differences were found between the groups when the methods of suicide were analyzed. There was no significant association between the completed suicides of the offenders and whether the victims of the parricidal acts died.
Survival After the Date of the Crime
When the Cox proportional hazards model was used, no association of matricidal, patricidal, and control offender groups with survival time was found among the offenders who died due to natural causes or unnatural causes other than suicide. In the case of suicides, however, the matricidal offenders had a significantly shorter survival time (mean, 5.1 years; SD 2.8) after the offense than did the patricidal (mean, 8.9 years; SD 8.1) or the control (mean, 13.1 years; SD 7.9) offenders. After adjustment for age at date of offense and status of victim (died, survived) the hazard ratio (HR) of death by suicide was higher among the matricidal (HR = 4.8; 95% CI, 1.11–20.86; p = .035) but not the patricidal offenders, when compared with the control offenders (Fig. 2).
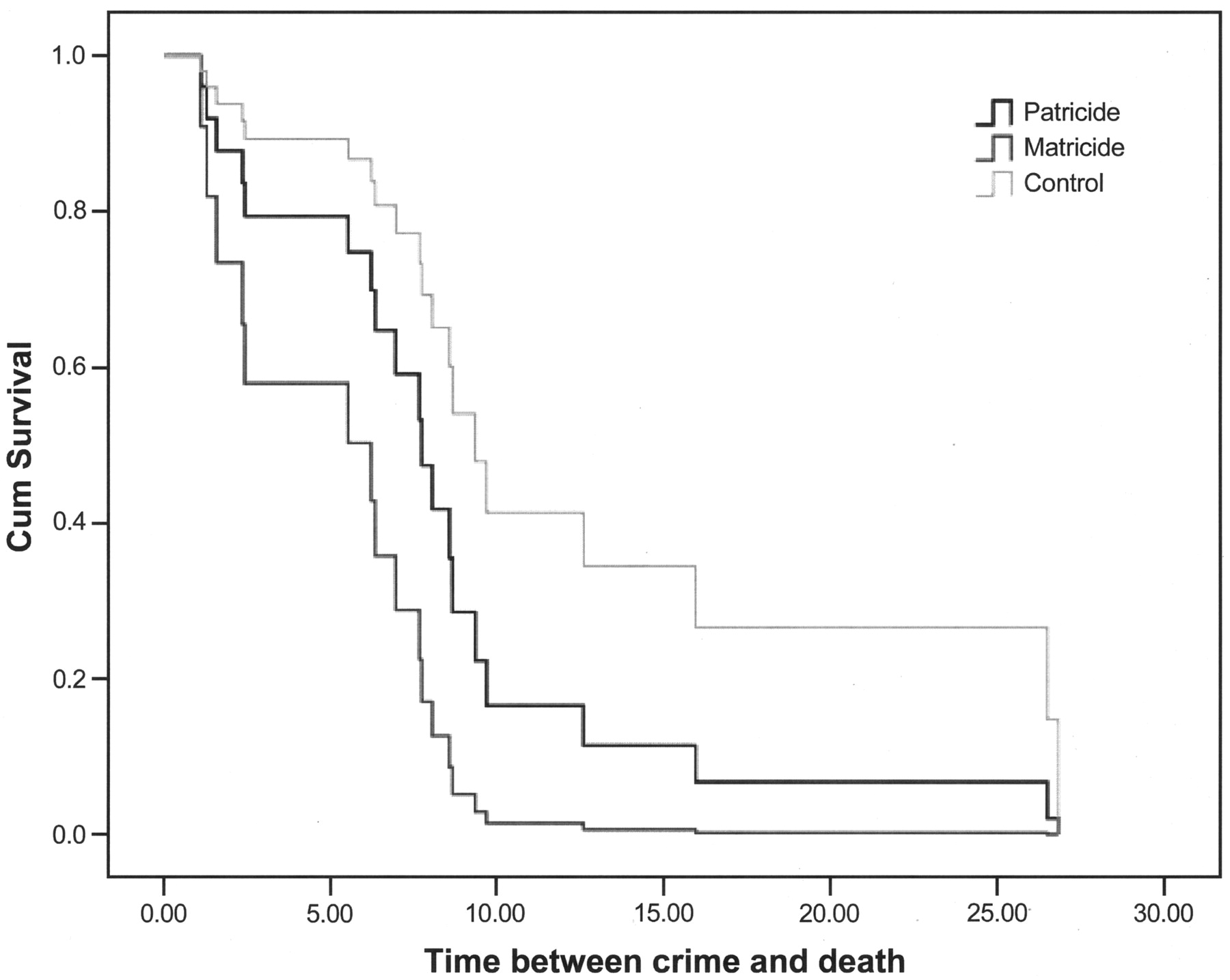
Survival time after the offense in cases of offender suicides among 99 matricidal, 113 patricidal, and 111 control offenders.
Discussion
This study provides systematic information on mortality among parricidal offenders. We used a nationwide sample of parricidal males who had undergone a mental state examination. The SMR of the parricidal offenders aged 25 to 49 years was higher than that of the general population.
A novel finding was that the matricidal males who died of suicide had a significantly shorter survival time after the offense than did the patricidal and control offenders who died of suicide.
It is a well-known fact that the mortality rates among offenders and psychiatric patients are elevated compared with those of the general population.4,37–42 In our study, 20 to 30 percent of the parricidal offenders died during the follow-up of 3 to 24 years. In a study with a sample of 53 mentally ill parricide offenders discharged from high-security care, 17 percent died during follow-up, as the mean length of follow-up was 7.2 years.24 Also, the proportion of deceased offenders in our study is in accordance with the mortality rates presented in studies of offenders in general, when taking into consideration the different follow-up periods. For example, in a Swedish study concerning offenders who underwent a forensic psychiatric examination, a total mortality of 17 percent was determined during a follow-up ranging from 13 to 16 years.1 Of Swedish homicide offenders, almost half died during the follow-up of 22 to 32 years.6 In our study the mean age at death was low in every offender group, being slightly over 40 years, which is consistent with the data in earlier studies.3,43
In our study, the all-cause SMRs were increased three- to fourfold, respectively, among the matricidal and patricidal offenders of the 25- to 49-year age group compared with that of the general population of the same age. This result is in accordance with that of a study of mentally disordered parricidal offenders, in which the researchers found an almost fourfold increase in mortality among male offenders compared with that of the general population.24 In comparison with offenders in general, the overall mortality rate has been estimated to be 4-fold among ex-prisoners,4 5-fold among habitually violent offenders,7 3-fold among homicide offenders,6 and up to 13-fold among mentally disordered offenders,2 compared with that of the general population. A recently published study of patients discharged from a medium-security care unit showed a sixfold increase in all-cause risks of death compared with that of the general population.43 Thus, parricidal offenders have a moderately increased mortality risk, similar in magnitude to that presented in most of the studies in which different offender samples were used. In general, offender mortality rates tend to be proportionately higher among the younger age groups when compared with the general population.3,9–11 One explanation for this may be that antisocial behavior, risk-taking, and impulsiveness tend to diminish with increasing age, which may account for our results, as well.
Overall, the proportion of deaths due to unnatural causes (suicides, accidents, and homicides) was high, constituting approximately 50 percent of the total deaths among the matricidal and patricidal offenders. One-third of deaths among the parricidal offenders were attributable to suicides. Kullgren et al.44 reported that among male offenders referred for forensic psychiatric examination and followed up for four to eight years, 56 percent of the total deaths were unnatural: 37 percent from suicide and 19 percent from accidents and homicides. In a large cohort of males with a history of imprisonment, accidents accounted for 22 percent, suicides for 17 percent, and drug overdose for 18 percent of all mortalities.9 With respect to the general population, among the Finnish working-age males in 2006, 13.3 percent of total deaths were due to accidents and 8.9 percent to suicides.45 In our study, 6.0 percent of all matricidal offenders (n = 99) and 7.9 percent of all patricidal offenders (n = 113) committed suicide, which exceeds the suicide rate in the general population. The percentage of suicides among the parricidal offenders in our data set is in accordance with the completed suicide rate of 7.1 percent found by Bourget et al.15 among parricide offenders.
The challenge for the health care and criminal justice systems is to recognize those at risk. It is known that prisoners and released prisoners, as well as those discharged from forensic psychiatric units, have increased risk of committing suicide.4,5,43 The suicide risk of released prisoners seems to be at its highest during the weeks following the release.5 Parricidal offenders have many factors that may increase the suicide risk (e.g., high psychiatric morbidity, social disadvantages, being stigmatized by the community, and guilt over the parricidal offense). Those responsible for the treatment and follow-up of parricidal subjects should be alert for the risk of suicide, and particular attention should be paid to the period after the offender is discharged from the institution. More information is needed on the specific risk factors for suicide.
Of unnatural deaths, suicides predominated in the matricidal group, whereas accidents constituted most of the unnatural deaths in the control group. These proportional differences may reflect the differential psychopathology and lifestyles among the matricidal and control offender groups. An interesting finding was that the matricidal offenders who died of unnatural causes and suicides were also younger at death than were the corresponding control subjects. Those matricidal offenders who committed suicide died a shorter time after the offense than the corresponding patricidal or control offenders. On the basis of the shorter temporal relationship between the offense and the suicide, it may be speculated that suicide is associated more strongly with the offense among matricidal offenders than among patricidal and control offenders. It is probable that the guilt and shame caused by the offense decrease in the course of time, having less impact as a factor that contributes to the suicide.
The briefer survival time after the offense among the suicidal matricidal offenders may illustrate the different underlying dynamics of the offense and perhaps the emotional connection to the mother. Although the study also includes offenses that did not result in the death of a parent (attempted homicides and other violent offenses), the psychological break in the relationship with the mother may have resulted in the nonsurvival of the offender. According to the attachment theory, the child's tie to the mother is the most fundamental in the psychological development of the child and the tie usually continues to be significant into adult life, more strongly for some individuals than for others.46 Green12 found that many of the matricidal males had failed to outgrow the attachment and dependence on their mothers. The killing of a mother has emotion-laden meanings, as it is committed within a mother-child bond that is usually the first relationship of the child and remains strong throughout the course of life.
As shown in previous work with the same study sample as was used in this study, the motives for the patricidal offenses included more interpersonal conflicts and confrontation with the victim than did the matricidal offenses, which may reflect the relationship with the victim—for example, abuse of the son by the father.47 A limitation in the current study is that specific variables regarding the quality of the parent-child relationship are not available. This question should be investigated in further studies.
Our previous work on the present data showed that the matricidal offenders had psychotic disorders more commonly than did the patricidal offenders.47 In addition, paralleling the major mental psychopathology found in this group, homicidal matricidal offenders were more commonly found to be criminally irresponsible. According to Finnish legislation, offenders without criminal responsibility are not sentenced but are committed to a mental hospital as criminally insane.32 Thus, nearly all offenders with psychotic disorders are ordered to be admitted to a forensic hospital for intensive treatment. In our study, the degree of criminal responsibility was not associated with mortality. Similarly, mortality was not associated with psychiatric diagnosis or disposition (prison or inpatient forensic psychiatric care) among Swedish homicide offenders.6 On the other hand, the mortality of mentally disordered offenders discharged from forensic psychiatric care has been estimated to be remarkably high when compared with that of the general population.2,43 The long hospitalization probably had a preventive effect on unnatural deaths in the psychotic group, and therefore the mortality of the offenders with no criminal responsibility did not exceed the death rates of offenders with nonpsychotic disorders.
The main methodological weakness of this study is the inevitable small sample size, which causes a loss of statistical power. For example, due to the small number of subjects, it was not possible to calculate cause-specific SMRs for the matricidal and patricidal groups. Because parricide is a rare phenomenon, a large sample is difficult to acquire, and statistical analysis remains restricted. Hillbrand and Cipriano48 have recently illustrated difficulties in accessing a statistically relevant nonbiased sample of parricidal offenders. In Finland, during the years 1998 to 2006, from one to eight parents per year (altogether 26 mothers and 21 fathers) died in parricides.49 Violent offenses other than homicides were included in our data, on the basis that studies comparing parricides and attempted parricides have not found major differences.14,17,48 The proportion of offenses other than homicides or potentially lethal offenses was small. On the other hand, this was a study with access to a nationwide database, containing all male parricidal offenders who had been admitted to undergo a forensic psychiatric examination. The study sample lacked those offenders who committed suicide immediately after the offense. Homicide followed by immediate suicide is an infrequent phenomenon, however. In a recent Finnish study covering one year, there were 10 homicide-suicides altogether, with the homicide victim being the spouse, or children, or both in every case.50 It may be assumed that the data set includes almost all offenders with psychotic disorders and most offenders with severe personality disorders, as some offenders with less severe mental disorders may not have been thoroughly examined and were not included in the study.51 The data set probably covers almost all homicides, as the more severe offenses lead more commonly to the mental state examination, but for less severe offenses, the coverage may be of a lower level.
The advantage of our study is that all deceased offenders could be traced reliably via the national death register system. The availability of high-quality mortality data for the general population ensures the validity of comparisons.52 In comparisons with the general population, one has to bear in mind that parricidal offenders differ from the general population in many variables that we were not able to control in this study.
Conclusions
The present study illustrates the vulnerability of parricidal offenders in terms of mortality. Mortality rates of parricidal offenders were found to be moderately increased compared with that of the general population in the age group of 25 to 49 years. The results suggest that parricidal offenders frequently die of unnatural causes and suicides, as do violent offenders in general. Suicides of matricidal offenders appear to be temporally more closely associated with the offense than the suicides of patricidal and control offenders. Several risk factors (e.g., mental morbidity and social disadvantages) contribute to the increased risk of death among parricidal offenders. The risk of suicide as an ultimate consequence of a long-term process should be recognized and taken into consideration during treatment. Appropriate interventions to prevent suicide should be provided within the health care system and prisons. On the basis of this study, matricidal offenders in particular seem to be at risk during the years after the offense. In the future, it is important to investigate the factors that influence the recovery and psychological survival of parricidal offenders.
Footnotes
-
Disclosures of financial or other conflicts of interest: None.
- American Academy of Psychiatry and the Law





{kind=link}
{kind=link}