


Abstract
The purpose of this retrospective study was to illustrate the differences in maternal and paternal filicides in Finland during a 25-year period. In the sample of 200 filicides [neonaticides (n = 56), filicide-suicides (n = 75), other filicides (n = 69)], the incidence was 5.09 deaths per 100,000 live births: 59 percent of filicides were committed by mothers, 39 percent by fathers, and 2 percent by stepfathers. The mean age of the maternal victims (1.6 y) was significantly lower than that of the paternal victims (5.6 y), but no correlation between the sex of the victim and the sex of the perpetrator was found, and the number of female and male victims was equal. The sample of other filicides (n = 65) was studied more closely by forensic psychiatric examination and review of collateral files. Filicidal mothers showed mental distress and often had psychosocial stressors of marital discord and lack of support. They often killed for altruistic reasons and in association with suicide. Maternal perpetrators also dominated in filicide cases in which death was caused by a single episode or recurrent episodes of battering. Psychosis and psychotic depression were diagnosed in 51 percent of the maternal perpetrators, and 76 percent of the mothers were deemed not responsible for their actions by reason of insanity. Paternal perpetrators, on the other hand, were jealous of their mates, had a personality disorder (67%), abused alcohol (45%), or were violent toward their mates. In 18 percent of the cases, they were not held responsible for their actions by reason of insanity. During childhood, most of the perpetrators had endured emotional abuse from their parents or guardians, some of whom also engaged in alcohol abuse and domestic violence. The purpose of this study was to examine the differences between maternal and paternal filicides in a sample of 200 cases in Finland. This report also provides a psychosocial profile of the perpetrator and victim in 65 filicides and a discussion of the influence of diagnoses on decisions regarding criminal responsibility.
Filicide, neonaticide, and infanticide are the murder of a child committed by a parent or a stepparent. Neonaticide refers specifically to the killing of a child on the day of birth, whereas infanticide is the killing of a child younger than 12 months.1
The rate of child homicide in Finland is higher than that in other developed nations: 7.31 in female and 6.54 in male children younger than 1 year per 100,000 live births in a study by Gartner2 (1965–1980); during the same period, the rate in Sweden was five times lower.
Several investigators studying the reasons for filicide have developed categories of the crime to aid in understanding the characteristics of this heterogeneous phenomenon. Most studies, however, have samples only of maternal filicides.
Resnick and Hatters Friedman3,4 have proposed a classification based on the motive for the filicide, and suggest categories of altruism, acute psychosis, unwanted child, accident or child maltreatment, and spousal revenge. Altruistic filicide is committed with the motive of relieving the child of real or, most often, imaginary suffering, and usually involves a suicide attempt by the parent. Acute psychosis involves severely mentally ill parents who kill their children while in a psychotic state. In the unwanted-child category, the victim is born unwanted and is a burden to the uncertain and incapable parent, whereas accidental deaths, later termed fatal maltreatment filicides are unintentional, due to a single episode or recurrent episodes of battering.
Later, Scott5 and d'Orban6 categorized maternal filicides with regard to the impulse to kill, on the basis of factors pertaining to the parent, the child, or the situation.
As earlier researchers categorized only maternal filicides, Bourget and Bradford7 were the first to recognize the importance of the sex of the perpetrator by adding paternal filicide as a separate category. The other categories were pathological filicide (perpetrator has a major psychiatric illness), accidental filicide (unintended death caused by abuse), retaliatory filicide (the murder of a child to punish a spouse), and neonaticide (unwanted pregnancy with the child killed within 24 hours of birth). Bourget and Gagné8 included parental motive, intent, and psychiatric illness as additional categories.
Studies on filicides report a higher incidence of maternal filicide,3,9,10,11 which is because neonaticides are almost always committed by mothers,12 as are infanticides in 73 percent of cases.13 Contradictory results have also been reported, however, indicating that filicides perpetrated one week after the birth of the child are often committed by fathers or stepfathers.3,7,13,14,15
It has been suggested that mothers are more likely to kill girls and fathers to kill boys16 and that boys are overrepresented among older filicide victims,10,11,13,16,17 but some studies report an equal number of both sexes among the victims.18,19
Often, parents who kill their children have diagnosed psychosis or major depression,5,7,8,14,15 and many studies report a high incidence of psychiatric symptoms. Resnick,3 for example, found that as many as 75 percent of perpetrators have psychiatric symptoms and, in recent studies by Bourget and Gagné, 85 percent of mothers and 56 percent of fathers were reported to have a diagnosis of major depressive disorder, schizophrenia, or other psychosis.8,14
Furthermore, Hatters Friedman and colleagues20 found that maternal motives for filicide were predominantly altruistic (misguided love) or acutely psychotic (without rational motive), and that 72 percent of mothers had experienced considerable developmental stressors, such as the death of their own mothers or incest. Lack of social and marital support, economic difficulties, family stress, young age, immaturity, and unrealistic expectations of motherhood have also been found to cause psychosocial stress.21
Research on filicidal fathers suggests that they often have a history of drug and alcohol abuse and that they are mostly unskilled or semiskilled and employed in low-wage occupations.10,22,23 Bourget and Gagné14 found that a history of domestic violence, multiple sibling victims, and attempted or successful suicide was also associated with paternal filicide. Classification of fathers who committed filicide found that 64 percent were mentally ill, 25 percent had committed fatal child abuse, and 4 percent had committed retaliatory filicide. The studies are based on different samples, however, and give contradictory results, depending, for example, on the inclusion of neonaticides or whether the perpetrators studied are collected among patients undergoing mental health treatment after committing a filicide.1
Especially regarding women, there has been discussion about the legal procedure applied to the perpetrators24 and about the differences in the legal procedures in each nation as to how perpetrators are held accountable for their actions.26
For example, Laporte and colleagues25 found that women who were sentenced to prison had lower socioeconomic status and, compared with those who received a medical disposition, were more likely to have had a criminal and substance abuse history. Marks and Kumar,9 on the other hand, reported that men committing filicide were more likely than women to be imprisoned for the same offense.
Furthermore, filicide-suicides are a less studied category because of the difficulty in collecting information after the death of the perpetrator. According to Hatters Friedman and colleagues,9 paternal perpetrators often attempt to kill their wives. The motives for filicide-suicide can be altruistic and acutely psychotic.9
Sample and Methods
Ethics approval for the study was obtained from the Ministry of Social Affairs and Health and the National Research and Development Center for Welfare and Health of Finland. The approval allowed a retrospective study of all the health and legal records, including mental state examinations, but no interviews were permitted.
Information concerning all deaths certified as homicide or with an undetermined cause of death in Finland for children 15 years of age or younger was obtained from Statistics Finland (a government agency providing national statistics) for the 25-year period from 1970 to 1994. There were 292 deaths coded by the ICD-9 as E960 to E969 (homicides; n = 207) and E970 to E979 (deaths of unspecified cause; n = 85).
In the Finnish legal system, the police investigate all deaths of unknown cause that occur outside hospitals, and a forensic autopsy is performed. The death certificate is signed after all investigations for the cause of death have been completed. Occasionally, the investigations are not completed when the death certificate is issued, and the final cause of death is recorded as undetermined. In this sample, 28 (33%) deaths certified as undetermined were caused or preceded by intrafamilial violence, according to the ruling of the court of justice. Other causes of undetermined deaths in this sample were accidents or suicide of the child (n = 24), children less than 2 years of age who were found dead at home but showed no signs of injury (n = 20), and other nonhomicide cases (n = 13). Extrafamilial deaths (homicides committed by family members other than a parent or a stepparent; n = 35) were excluded because our main interest was in intrafamilial filicides.
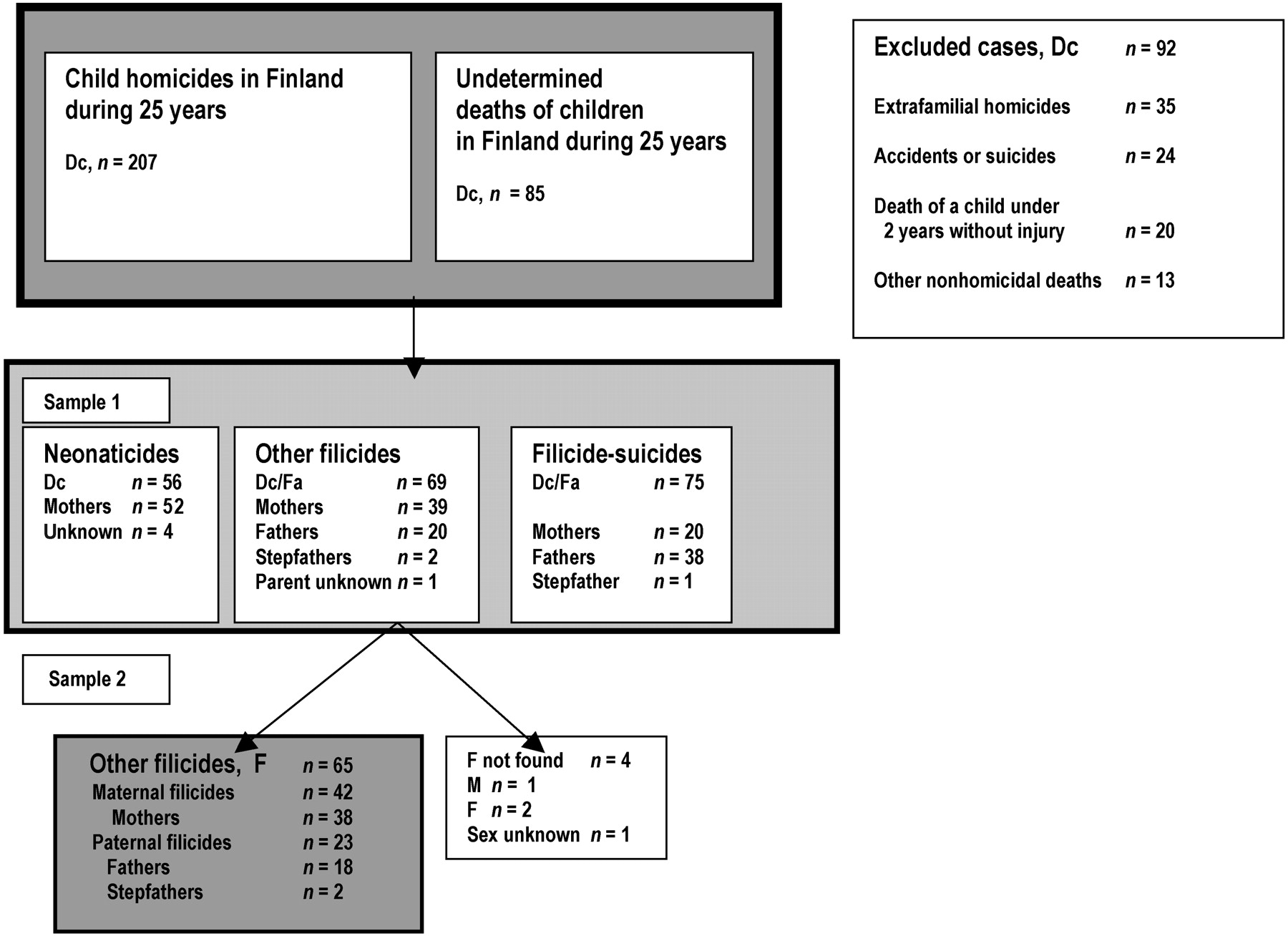
The sample after the exclusions (n = 92) included intrafamilial filicides (n = 200), which were determined to be filicide-suicides (n = 75), neonaticides (n = 56), and other filicides (n = 69).
The data collected from filicide-suicide cases (a parent commits filicide and then suicide; n = 75) were sparse because the court records and mental examinations of the perpetrator were unavailable and the information in the autopsy records was limited. The cases of neonaticides (mother giving birth in secret and killing the infant within 24 hours; n = 56 cases) were investigated only on the basis of the death certificates because the main interest of the series of investigations was in parental behavior and physical abuse. The files were not found in 4 of the remaining 69 cases. The required data were available on 65 homicides committed by 58 perpetrators (see Figure 1 ).

The two samples after the exclusion of cases. Dc, death certificate; Fa, forensic autopsy report; F, court and medical records or medical examination.
The demographic data of the sample of 200 were studied, and a more detailed study was completed on the sample of 65 cases. Data were examined with descriptive statistics (the mean, standard deviation, 95% confidence interval (CI), and percentage of categorical variables); however, because of the small sample size, tests of statistical significance were frequently not feasible.
The sample of 65 cases of filicide was studied more closely by using retrospective case review methodology. Data were obtained from medical and forensic records, which included forensic psychiatric examination when required by the court. In Finland, the perpetrator undergoes a detailed forensic examination that includes physical examination, brain computed tomographic (CT) scan or functional magnetic resonance imaging (fMRI) study, electroencephalogram (EEG), laboratory tests, structured psychological tests, and structured diagnostic interviews during a period of 4 to 8 weeks, usually in a psychiatric or forensic psychiatric hospital. The psychiatric examination includes data obtained by court order from physicians and hospitals, schools, social welfare offices, the military, prisons, and the crime registers, in addition to questionnaires completed by parents, siblings, teachers, and employees. The diagnoses and the responsibility for one's actions by reason of insanity are evaluated by the reports of the diagnostic instruments and the clinical observation.33 The senior psychiatrist of the Forensic Psychiatric Department returned a diagnosis according to the Finnish version of the International Classification of Diseases, ICD-9, and Diagnostic and Statistical Manuals, DSM-III and DSM-III-revised, which were in use in Finland during the period of the review. Demographic data, psychiatric diagnosis, and developmental history were derived from the medical records of the perpetrator if the forensic psychiatric examination was not required.
The history of the victim was obtained from the autopsy report, as well as medical and collateral records. An autopsy was performed in every case and included microscopic and blood samples obtained by an expert in forensic medicine. Furthermore, X-rays were taken if child battering was suspected.
Results
After the exclusion of 92 cases, the sample of 200 included all the filicides of children younger than 15 years committed by parents during 25 years in Finland (75 filicide-suicides, 56 neonaticides, 69 other filicides), which is on average 8 cases per year, and 5.09 deaths per 100,000 live births. The majority (59%) were maternal (n = 117) and the remaining (49%) were paternal (biological fathers n = 75, (38%) and stepfather n = 3, (2%) filicides. The sex of the parent was unknown in five cases (four neonaticides in which the infant was found dead and the parent was unknown).
The mean age of the victims in the sample of 200 was 3.2 years (SD 3.8, 95% CI = 2.6–3.7) and the mean age of maternal victims, 1.6 years (SD 2.7, 95% CI = 1.1–2.1), was significantly lower than the mean age of the paternal victims, 5.6 years (SD 4.0, 95% CI = 4.7–6.5) (t = −8.28, p = .000). Of the victims killed during the first year of life, 90 percent were killed by the mother, whereas 54 percent of the paternal victims were older than 5 years. The relation of the sex of the victim (50% female) and the sex of the perpetrator was not significant (χ2 = 1.6, p = .242).
A family annihilation (killing the spouse and all the children in the family) was committed by 18 percent of the paternal perpetrators.
Neonaticides
Of the 56 cases of neonaticide, 52 were perpetrated by biological mothers. In 4 cases, the perpetrator was unknown. The victim was female in 57 percent of cases. The pregnancy was concealed, and the infant was born at home and killed immediately in almost all the cases. Sixty percent of the cases occurred in the period between 1970 and 1979, and the same percentage took place in rural areas. (In 1995, 64% of the Finnish population lived in urban areas, which is a low proportion compared with other Western countries28).
No other information was available on the death certificates.
Filicide-Suicides
The filicide-suicide sample included 22 cases with 20 biological mothers as the perpetrators (2 mothers killed both of their two children) and 53 cases with 38 biological fathers and 1 stepfather as the perpetrators. Ten fathers killed two children and two killed three children (31% multiple victims). Furthermore, nine fathers killed all the family members (23% of filicide-suicides). The perpetrator groups killed an equal number of male and female victims.
The mean age of the maternal victims was 4.0 years (SD 4.2, 95% CI = 2.2–5.9) and the age of the paternal victims was 6.4 years (SD 3.7, 95% CI = 5.3–7.4) (t = −2,39, p = .019). Shooting with a firearm was the most common cause of death (56%) in paternal filicide-suicide cases, whereas maternal cases had an equal number (25%) of poisonings, drownings, and stabbings. The filicide-suicide occurred in urban areas in 77 percent of the maternal and 43 percent of the paternal cases. No other data concerning the perpetrator and the victim were available.
Other Filicides
Perpetrators
In this sample of 65 filicides (69 cases; the files were found in 65 cases), 38 (66%) perpetrators were the biological mothers of the victims, whereas of the male perpetrators (n = 20; 34%), 18 were biological fathers and 2 were stepfathers. All the perpetrators were white, originating from the Finnish population, except one mother, who was Roma (a small ethnic minority in Finland).
The mean age of the mothers was 27.9 years (SD 6.7, 95% CI = 26–29.7) and the mean age of the fathers, 29.4 years (SD 7.9, 95% CI = 25.7–33.1) (t = −1,25, p = .216).
The distribution of the cases between rural and urban areas was nearly equal: 53 percent of the mothers and 65 percent of the fathers lived in urban areas. Eighty-four percent of the mothers and 70 percent of the fathers were married or cohabiting, and the rest were single parents or divorced. Seventy-one percent of the mothers and 75 percent of the fathers were semiskilled or unskilled workers and of low socioeconomic status.
Psychosocial Stress, Mental Health Distress, and Childhood Traumas of the Parent
When interviewed by a psychiatrist and a psychologist in the forensic psychiatric unit, the maternal perpetrators reported that they had experienced severe stress caused by marital discord and the violence of the spouse, while paternal perpetrators were reported to be jealous in 50 percent of cases. Mental health distress preceding the assault was reported in 74 percent of the maternal perpetrators, but in only 10 percent of the paternal perpetrators. Furthermore, in 45 percent of the cases, the fathers abused alcohol. They were violent to other members of the family in 45 percent of the cases.
Traumatic childhood histories, determined in the mental examination, were frequent among perpetrators. Physical abuse was reported in only 14 percent of maternal and 13 percent of paternal childhood histories; however, emotional abuse was mentioned as a traumatic factor in 67 percent of the maternal and the paternal cases. Alcohol abuse by a parent and domestic violence, as well as mental illness of a parent, were also major factors (55% of the maternal and 74% of the paternal perpetrators). Moreover, the death of a parent experienced in childhood, especially the death of the father among male perpetrators, was frequent (40%). Antisocial behavior in adolescence and adulthood was frequent among the male perpetrators.
Information was missing in two maternal and five paternal cases.
Victims
The sex of the victim was male in 58 percent of all cases; mothers killed their sons in 55 percent and fathers in 65 percent of the cases.
Forty-two percent of the victims were younger than 1 year. The mean age of the maternal victims was 2.2 years (SD 2.1, 95% CI = 1.6–2.9), and the mean age of the paternal victims was 4.2 years (SD 4.4, 95% CI = 2.3–6.1) (t = −2.37, p = .021). The age distribution of the victims in both groups is presented in Table 1.
Ages of the Victims in Filicides
The number of victims among first- and second-born children was equal. Fathers killed the firstborn child in 74 percent of the cases. In three cases of maternal filicide and in two cases of paternal filicide, the child was from the mother's previous relationship. Delay in the development of the child was found in three cases, but none was severely disabled. The victim was born prematurely in two of the maternal and three of the paternal cases. Early separation of the infant from the perpetrating parent, caused by the infant's premature birth or by the child's being taken into care (3%), was found in 10 percent of the maternal and 30 percent of the paternal filicides. Most of these filicides were caused by battering.
Physical abuse preceding the filicide was found in nine (21%) maternal and four (17%) paternal cases, but no sexual abuse was detected. Neglect preceding the filicide was obvious in nine maternal and two paternal filicides, however.
Assault
In 92 percent of the maternal and 80 percent of the paternal assaults only one child died. Two mothers tried to kill all their children, but succeeded in killing only the youngest child, two mothers killed more than one child, and one killed her sister's child simultaneously. In 40 percent of the maternal and paternal cases, the perpetrator clearly intended to kill, and in 34 percent of the maternal and 50 percent of the paternal filicides, the death was said to be accidental. Six fathers in a state of jealousy intended primarily to kill their wives, and three succeeded in doing so. Only one filicide was reported to have been committed in revenge, however. Thirty percent of the fathers and five percent of the mothers were under the influence of alcohol at the time of the filicide.
Mothers killed their children by drowning (33%), strangulation (31%), or banging the child against a hard object (21%). The most common methods of killing by fathers were banging the child against a hard object (36%) and strangulation (28%); a firearm was used by 17 percent of paternal perpetrators.
Diagnosis, Diminished Responsibility by Reason of Insanity, and Legal Proceedings Against the Parent
Psychosis or psychotic depression was diagnosed in 51 percent of the maternal cases and 20 percent of the paternal cases, while personality disorder, most often with borderline features such as immaturity, impulsiveness, and poor control of affect, were the most often diagnosed features, alone or with the comorbidity of depression or alcoholism, in 67 percent of the paternal and 41 percent of the maternal perpetrators. Diagnoses are presented in Table 2.
The Diagnosis by Mental Examination
The intelligence tests revealed that the perpetrators were of average intelligence. Only three mothers and one father had an IQ less than 80.
Not being responsible for one's actions by reason of insanity was recorded for 76 percent of the maternal perpetrators, and 69 percent were not sentenced, whereas fathers and stepfathers were deemed not to be responsible for their actions by reason of insanity in 18 percent of the cases and to have diminished responsibility in 65 percent. The degree of responsibility of the perpetrators and the sentences are presented in Table 3.
Perpetrators’ Responsibility and Sentences
Discussion
The results of this study support earlier findings on the differences between maternal and paternal filicides.1,30,32
In the first sample of 200 cases of neonaticides, filicide-suicides, and other filicides, mothers dominated as the perpetrators. When the sample was divided into subgroups, however, the fathers dominated in the filicide-suicide group and the mothers in the neonaticide and the other filicide groups.
Neonaticides were included only in the first sample, as were filicide-suicides. In those cases, information on the family's circumstances, the victims, and the perpetrators was not available, as often all the family members were killed. The lack of information concerning those cases reduces the comparability of the sample with others.
The results of the sample of other filicides verified differences in maternal and paternal filicides.
Almost all maternal perpetrators reported high levels of stress and lack of support and resources at the time of the filicide. In general, maternal filicides could be divided into two major categories: altruistic motives and maltreatment. Most maternal perpetrators had altruistic motives and had depression or psychotic illness, supporting findings in studies of maternal filicides.10,20,31 Perpetrators of the altruistic type were older, had a higher level of education, and were mostly employed. They were also in contact with the health care system and were even undergoing treatment. Maternal perpetrators of the second category were abusive and had features that are frequently reported in abusive parents: being the primary caregiver, caring for a child that is not biologically related to the present partner, having a low income and education level, being in an ongoing abusive relationship, having conflict with family members, and having limited social support.1,5
These perpetrators often had a diagnosis of a personality disorder. In contrast to other maternal filicides, the victims were neglected or had experienced separation from the mother.
Fathers were violent to family members, abused alcohol, and had personality disorders, as verified in other studies.23,32 The presence of reported significant life stressors included impending marital breakup, jealousy, fear of separation, long-term substance abuse, and low education level and socioeconomic status.
An interstudy comparison is presented in Table 4. Comparability is limited because the studies differ regarding the inclusion criteria of the sample, methods used, and factors studied.
Interstudy Comparison of the Results
Emotional abuse emerged as a frequent childhood trauma, present in as many as 67 percent of the cases. A recent study of traumatic experiences in childhood in patients in Finland revealed that 38 percent of the primary care patients reported neglect by their family, 16 percent reported sexual abuse, and 10 percent described physical abuse.31 The results were obtained by questionnaire and are not directly comparable; nevertheless, they suggest that in childhood, the perpetrators in this sample were exposed more to emotional abuse, neglect, domestic violence, and the mental illness and alcohol abuse of their parents than are nonfilicidal persons. Furthermore, the relationship with the parent of the same sex in the perpetrator's childhood seemed to be an important factor. The relationships between maternal perpetrators and their mothers were reported to be cold and rejecting, whereas paternal perpetrators often had a violent, alcoholic father who died during the perpetrator's childhood or adulthood. The importance of the relationship with the parents in the perpetrators’ insufficient ability to establish a mature and giving relationship with their children was suggested in the very early studies by Harden15 and Rodenburg.15
No sexual traumas were mentioned, but studies have connected sexual victimization with perpetrators’ childhood experiences,20 making such a finding statistically probable. Few perpetrators who repeatedly physically abused their children reported no childhood traumas except emotional abuse.
High numbers of mental illnesses and personality disorders were also reported by Somander and Rammer10 in a Swedish sample. In that study, the perpetrators were examined by a forensic psychiatrist in a forensic inpatient clinic, as in our sample, which may account for the large number of diagnosed mental disorders. Personality disorder was diagnosed in almost all perpetrators in the Swedish study and in 41 percent of the maternal and 67 percent of the paternal perpetrators in the Finnish sample. The fluctuation in results may also be due to the classification system, since, in the past, only one main diagnosis was applied to psychiatric disorders, and in the presence of major mental disorder, personality disorders were not diagnosed. In studies of different diagnostic instruments, researchers have found that diagnosis of personality disorders cannot be based purely on direct questions or diagnostic questionnaires but must include clinical observation and interpersonal interaction over time.
Moreover, culture and legislation affect practices and, for example, studies conducted outside the United States document more mental illnesses in offenders.35
Finland, like many European countries, has legislation similar to that of the British Infanticide Act of 1922, proposing that women who are vulnerable after giving birth often receive no sentence and are referred for mental treatment.4,35
Most mothers were deemed not responsible for their actions by reason of insanity, no sentence was handed down, and in most cases they were sent to psychiatric hospitals. These perpetrators were psychotic, depressed, or too young to understand the consequences of their actions. Borderline personality disorder, unlike other personality disorders, may lead to a finding of diminished responsibility in Finnish forensic psychiatric examinations, as psychological functioning—that is, the ability to control one's behavior and understand the consequences—may be decreased. Nevertheless, each case is evaluated separately by examiners and The National Authority for Medicolegal Affairs.
Mental examination was not required of five male perpetrators who caused their children's accidental deaths in a single battering. These offenses may support the stereotypic picture that fathers are more violent and that no forensic psychiatric examination is necessary to eliminate the possibility of mental disorder.
On the other hand, a recent Finnish study of the mental disorders of male parricidal offenders showed that matricidal offenders were more commonly found to be psychotic and not guilty by reason of insanity than were patricidal offenders. Personality disorders showed up frequently among patricidal offenders.37 Mentally ill perpetrators had been in contact with mental health services or even were in ongoing treatment. Yet, the dangerous condition of the parent was not detected in time, even though they often voiced their concerns over their children or the delusion that the child was unsafe, too weak to live, or in danger of being taken away,38 or they had suicidal intentions, which are sometimes found to parallel filicidal intentions.39,40 Abusive perpetrators, however, were not receiving treatment or in contact with professionals and the signs of the battering or domestic violence were hidden.
Limitations of the Study
Despite the many sources of information used in the forensic psychiatric examinations, we have only the information that people were willing and able to provide, and the records also varied in quality and quantity, including more or less imprecise data and reported experiences about the victims and perpetrator's lives. Furthermore, forensic and forensic psychiatric diagnostic practices have developed during the 25-year study period, and, for example, sexual and physical abuse were either not reported or detected, although statistically they would be probable. Data were also limited on neonaticides and filicide-suicides and thus direct comparison with other studies in which the data were more complete was hindered.
Conclusion and Recommendations
In general, mothers committed more filicides in our sample. Filicidal mothers killed mostly infants, and they showed mental distress and had psychological stressors of marital discord and lack of support, while filicidal fathers had personality disorders, abused alcohol, and were violent.
Clinicians should therefore be aware of depressed parents and directly elicit suicidal or even filicidal ideations. Social support for families and child protection should also be actively offered when parents show an inability to control their lives while taking care of their children.
In Finland, children's psychiatric departments and public health services have developed psychiatric units for children younger than three years and their parents, to support early interaction and offer rapid interventions for families in distress. Domestic violence and child abuse have also been the focus of many national projects in the hope that they will prompt the authorities to identify situations in which children are in danger.
Footnotes
-
Disclosures of financial or other conflicts of interest: None.
- American Academy of Psychiatry and the Law





{kind=link}