


Abstract
Not all males undergoing phallometric testing for assessment of deviant sexual interests respond adequately to test stimuli. As poor response may be linked to hormonal, neurologic, vascular, or psychogenic causes, we studied the ability of sildenafil, an effective proerectile agent, to increase penile blood flow during phallometric testing. Twenty-two males completed this double-blind, placebo-controlled trial of sildenafil (100 mg). Each participant underwent phallometric testing with and without sildenafil. On average, each subject's peak response was 50 percent greater in the sildenafil condition than it was in the placebo condition (p < .05). Correlations between participants' penile response to human stimulus categories, with or without treatment, were all very high (r = 0.77–0.89) and statistically significant, thus indicating excellent reliability between the two test conditions. These results support earlier findings that sildenafil significantly increases phallometric response among middle-aged males. Moreover, pharmacologic treatment did not compromise the reliability of phallometric diagnosis.
While patient-reported symptoms and behaviors are prerequisites for diagnosing virtually all mental disorders, individuals with deviant sexual preferences are rarely forthcoming about their experiences.1,2 Pedophilia is a psychiatric illness found almost exclusively in males and characterized by “recurrent, intense” erotic interest in prepubescent children (Ref. 3, p 572). It has been alternatively defined as the erotic orientation of individuals whose sexual attraction to prepubescent children exceeds their sexual attraction to physically mature adults.4 Less frequently encountered in the literature is the term hebephilia, which denotes a preferential attraction to pubescents. In a recent study, penile plethysmography was used to discriminate hebephiles from pedophiles.5,6 Clinical authorities recognize that not all sex crimes against children are committed by pedophiles or hebephiles.7 Some men who have a sexual preference for adult women may molest children in certain circumstances—for example, while they are under the influence of alcohol or drugs. Differentiating between pedophilic and nonpedophilic sexual offenders has important implications clinically, as sex-drive-reducing medications may be therapeutically warranted in the former group.8
Certain types of sexual offenses, in particular crimes involving younger, male, multiple, and extrafamilial victims, make a diagnosis of pedophilia in perpetrators more likely.9 While these variables increase the probability of sexual reoffending in men with a history of child molestation,10 sexual arousal in response to children as measured by phallometry remains the single best predictor of sexual recidivism.11 Most men presenting for psychiatric assessment following charges or convictions of sexual offending against children deny an erotic attraction to minors.12 In these instances, the patients' accounts of their symptoms and behavior must be weighed against the likelihood of their giving false information to avoid legal prosecution if they have indeed committed a crime. A classification procedure that can reliably determine erotic preference without relying on patient-reported symptoms is therefore a useful adjunct to the clinical assessment of sexual offenders against children.
The phallometric test is a psychophysiological tool used to assess the erotic age and gender preferences of adult males. Volumetric phallometry measures participants' penile blood volumes under controlled conditions in a laboratory setting while they are exposed to a standardized set of sexually themed stimuli depicting adults and children. Increases in penile blood volume serve as markers for the individuals' relative attraction to the different categories of persons. While Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) criteria for pedophilia do not include results of phallometric testing,3 a phallometric classification of pedophilia makes a diagnosis of pedophilia more likely in men who have sexual offenses against children but repudiate any erotic interest in them. Several reviews have addressed the use of phallometric testing in clinical assessment.13–15 Recent studies suggest that phallometry may be able to detect the presence of deviant erotic interests in sexual offenders with developmental disabilities16 and juvenile sex offenders.17
Blanchard and colleagues18 reported that the sensitivity of our phallometric laboratory in classifying as pedophiles men who were accused of committing sexual crimes against prepubescents but claimed a preferential attraction to adult women was 61 percent. This result was predicated on the assumption that males who lacked charges against adults and presented with the greatest number of extrafamilial child victims (≥3) were most likely to be true pedophiles; among the 59 men accused of sexually offending three or more extrafamilial child victims in this sample, 36 (61%) were phallometrically classified as having a pedophilic orientation. The phallometric test detected the lowest rates of pedophilia among males with only one extrafamilial child victim. Data also revealed that 16 percent of their original sample had clinically uninterpretable phallometric test results due to a host of factors, including inadequate penile response. As uninterpretable phallometric results can compromise the test's utility, it is incumbent on researchers to investigate any intervention that could ameliorate an insufficient response.
Sildenafil is a proerectile agent that has been shown to increase penile tumescence through relaxation of the corpus cavernosa smooth muscle. Its mechanism of action involves competitive inhibition of the intracellular metabolic enzyme phosphodiesterase five (PDE5). One of the functions of PDE5 is to degrade the second-messenger molecule cyclic guanosine monophosphate (cGMP), which promotes smooth muscle relaxation. Therefore, sildenafil sustains an erection by minimizing the destruction of cGMP.19 It is a safe medication that is well-tolerated in humans.20
Our research group recently found that low-dose sildenafil increases the peak response during phallometric testing among middle-aged males.21 Participants who received 50 mg of sildenafil before testing showed a significant increase (28%) in phallometric response compared with those tested without the agent. These results prompted us to examine the effect of a larger dose of sildenafil on phallometric response, by utilizing a more rigorous experimental design. Similar to our previous study, we purposely selected a sample with characteristics that would bias against finding a significant association between drug treatment and increased response. For example, we restricted participation to men between the ages of 45 and 60 years, in the knowledge that sildenafil is more effective in treating younger versus older males with erectile dysfunction (ED).22 Participants were largely unemployed men living in shelters who had the leisure time to volunteer for the study. Our study was not designed to test the question of whether sildenafil may cause deviant phallometric responses in the laboratory. Rather, we hypothesized that administering 100 mg of sildenafil before phallometric testing would increase the response, at least to the level observed with the lower dose, even under double-blind, placebo-controlled conditions.
Methods
This study was approved by the Research Ethics Board at The Centre for Addiction and Mental Health. Males between the ages of 40 and 65 years who responded to recruitment advertisements posted in our hospital and other research centers were eligible to participate. The recruitment posters indicated that study investigators were interested in testing the effect of sildenafil on sexual arousal in males. Potential participants were encouraged to contact the lead investigator (N.J.K.) for more information.
We designated the following as exclusion criteria for the study: inability to speak or understand English; presence of psychotic disorder; legal blindness or deafness; IQ < 70; serious cardiac, hepatic, ophthalmic, or renal illness, as determined by history, physical examination, or laboratory investigations; history of priapism; current use of sildenafil or other PDE5s; allergy to sildenafil or other PDE5s; lactose intolerance (both drug and placebo capsules were compounded with lactose); current use of nitrates or other medications known to interfere with the metabolism of sildenafil; and current residence in a household with children. This last criterion was imposed to preclude any obligation on the part of the study investigators to inform the necessary authorities should participants' self-report and phallometric data suggest that they presented a danger to children. Potential participants who cared for other vulnerable populations, including older members of society, were not excluded, as gerontophiles (individuals with a sexual preference for the elderly) are extremely rare and our phallometric apparatus does not include stimuli to test for the presence of gerontophilia.
Two participants reported charges and/or admissions of criminal sexual behavior perpetrated against females age 17 or older. No attempt was made to corroborate the participants' self-reported legal histories by accessing law enforcement agency databases. Participants completed a standardized protocol form used in our laboratory, which included questions about the gender and age of persons to whom participants were most sexually attracted, as well as their lifetime number of sexual partners.
All participants received a complete history and physical by a physician investigator in addition to routine blood work, urinalysis, and electrocardiogram. Participants served as their own controls for the study. Sildenafil 100 mg or a placebo capsule identical in appearance to the compounded drug was dispensed to each participant one hour before the first phallometric testing session; before the second session, the other agent was administered. Although both subjects and study investigators were blind to the identity of the drug or placebo and to the order in which the participants received them, the capsules were delivered to the investigators in randomized batches, such that half of the participants received the drug first and half received placebo first. Testing sessions were separated by at least 48 hours to ensure that drug metabolites were sufficiently cleared from the participant's system. Participants were given the opportunity to discuss their phallometric results and receive counseling from the clinician-investigators if they wished; they were compensated $120 CAD for their involvement in the study.
Our phallometric laboratory was equipped for volumetric plethysmography. The main components included a glass cylinder that fit over the penis and segregated the air inside the cylinder from the outside atmosphere. A rubber tube was attached to the cylinder and connected to a pressure transducer, which converted differences in air pressure to voltage-output changes. Increases in penile volume compressed the air inside the cylinder, producing an output signal from the transducer. The apparatus was calibrated so that known quantities of volume displacement in the cylinder (2 cubic centimeters (cc)) corresponded to known changes in transducer voltage output. This instrument is highly sensitive and can reliably detect changes in penile blood volume much less than 1 cc. Readers are referred to Blanchard et al.18 for specific details on the phallometric apparatus used in our laboratory.
First, the examinee put the glass cylinder over his penis, according to instructions from the test administrator. He then sat in a reclining chair that faced three adjacent projection screens and put on a set of headphones. Following this setup, the examinee's lower body was draped with a sheet to minimize any embarrassment. The examinee's face was monitored by a low-light video camera during the test to detect stimulus avoidance strategies, such as closing the eyes or averting them from the test stimuli. Stimuli included audiotaped narratives delivered through the headphones, which corresponded with slides shown on the projection screens. The visual stimuli included images of nude pubescent and prepubescent boys and girls. These models were photographed circa 1970 after their parents signed written consent forms granting permission for the pictures to be used in clinical and research activities involving penile plethysmography at our institution. These stimuli have been used in over 10,000 phallometric tests in our laboratory. No child or adolescent model has ever returned as an adult requesting the removal of their photos from the phallometric protocol.
There were seven categories of narratives that described sexual interactions with prepubescent girls, pubescent girls, adult women, prepubescent boys, pubescent boys, and adult men as well as solitary, nonsexual activities (i.e., neutral stimuli). All narratives were written in the second person and present tense. The narratives describing heterosexual interactions were recorded with a woman's voice, while those describing homosexual interactions were recorded with a man's voice. Neutral stimuli were recorded with voices of both sexes. The specific test used in this study has been described in detail elsewhere.18
Each trial consisted of one narrative accompanied by photographic slides on three adjacent screens that simultaneously projected the front view, rear view, and genital region of a nude model who corresponded in age and gender to the topic in the narrative. Individual trials included three such models presented for 18 seconds each. The total duration of a trial was therefore 54 seconds, during which the examinee viewed a total of nine slides, three at a time. Neutral narratives were similarly accompanied by slides of landscapes. The full test consisted of four blocks of seven trials with each block containing one trial of each type (e.g., adult female) in pseudorandom order.
Although the length of the trials was fixed, the interval between trials varied, since penile blood volume had to return to its baseline (flaccid) value before a new trial could be initiated. The time needed to complete a test was between one and two hours, with and without sildenafil. Recording of penile blood volume began five seconds before trial onset and ended five seconds after trial offset. The pre- and post-trial data were not included in any calculations; hence, the trial response did not reflect recovery (detumescence) rates. Penile blood volume changes were sampled four times per second. The examinee's response was quantified in two ways: as the extremum of the curve of blood volume change (the greatest departure from initial value occurring during the 54 seconds of the trial) and as the area under the curve.
Each examinee's 28 extremum scores were then converted into standard scores based only on his own extremum data; the same operation was carried out on his area scores. Next, standardized extremum and area scores were combined to yield a separate composite score for each of the 28 trials, using the formula (ziE + ziA)/2, where ziE is the standardized extremum score for the ith trial and ziA is the standardized area score for the ith trial. These operations were performed for two reasons. First, in phallometric work, some transformation of raw scores is generally necessary when combining data from different examinees, as the interindividual variability in absolute magnitude blood volume changes can obfuscate even quite reliable statistical effects. There are numerous sources of such variability, including the examinee's age, his state of health, the size of his penis, and the amount of time since his last ejaculation from masturbation or interpersonal sexual activity. Empirical research has shown the z-score transformation to be optimal.23,24 Second, the highly correlated area and extremum z-scores are averaged to obtain a composite that reflects both the speed and amplitude of response and lessens the impact of anomalous responses, that is, large change from initial value but small area or vice versa.
In the last stage of basic processing, the data were reduced to seven final scores for each examinee by computing the mean of his four composite scores for each of the seven stimulus categories. These seven category scores were then taken as measures of the examinee's relative erotic interest in adult women, pubescent girls, prepubescent girls, and so forth.
Another parameter measured in our laboratory was the amount of penile response (as opposed to the direction of response). This parameter was quantified as the mean of the three greatest penile responses to stimuli in any category (excluding neutral). The observed quantity is called the output index,25 which was expressed in milliliters of penile blood volume increase, beginning at trial onset. In clinical assessment and in some types of research, the output index is used to identify examinees whose penile blood volume changes during the test trials remain within the range typical of random blood volume fluctuations in nonaroused participants, and the phallometric data of examinees who fail to meet the criterion output index of 1.0 cc are excluded. In studies that focus on the absolute magnitude of penile response,26 rather than the relative magnitude of penile response to specific stimuli classes, the output index is used as a key dependent variable, as opposed to a gating criterion, and participants are not excluded on the basis of low output indices.
Statistical analyses were performed with SPSS (version 15.0). Except where noted, Student's t tests were paired and two-tailed.
Results
Twenty-four participants began the study, of which 22 completed the investigation. We aimed for a sample size of 24 participants, double that of our previous open-label trial.21 One participant was forced to withdraw after he ejaculated during the first phallometric testing session; the second individual lost interest in the study and opted not to continue. The average age of the sample was 48.9 ± 6.8 years. An independent-samples t test revealed that age did not significantly differ between heterosexual and homosexual participants (t20 = 1.19; p = .25).
Details of the participants' sexual histories and other demographic variables are summarized in Table 1. Two of the homosexual participants estimated having had 500 lifetime male sexual partners each. While this number may appear excessive compared with the sexual habits of the general homosexual population, research data indicate that a sizeable proportion of gay men frequenting baths, sex clubs, and gay bars report a very high number of indiscriminate and anonymous sexual encounters. For example, a survey conducted of San Francisco gay men in 1983, when the risks of unsafe sexual practices in relation to transmission of HIV had already been widely publicized, found that 61.6 percent of men (n = 400) visiting baths or sex clubs reported having had two or more sexual encounters in the previous month, while 17.3 percent of men (n = 400) socializing in gay bars or clubs similarly admitted to having had at least two sexual encounters in the preceding month.27 Assuming that the monthly frequency of random sexual encounters remained relatively constant for many of these individuals over the intervening years, it would take some gay men less than two decades to accumulate 500 lifetime sexual partners. The mean age of our study participants was nearly 50 years; therefore, a lifetime number of 500 sexual partners among our homosexual participants would not be an unexpected result, especially if these men first became sexually active in their early twenties or younger.
Demographic and Sexual History Characteristics of Self-Reported Heterosexual and Homosexual Participants
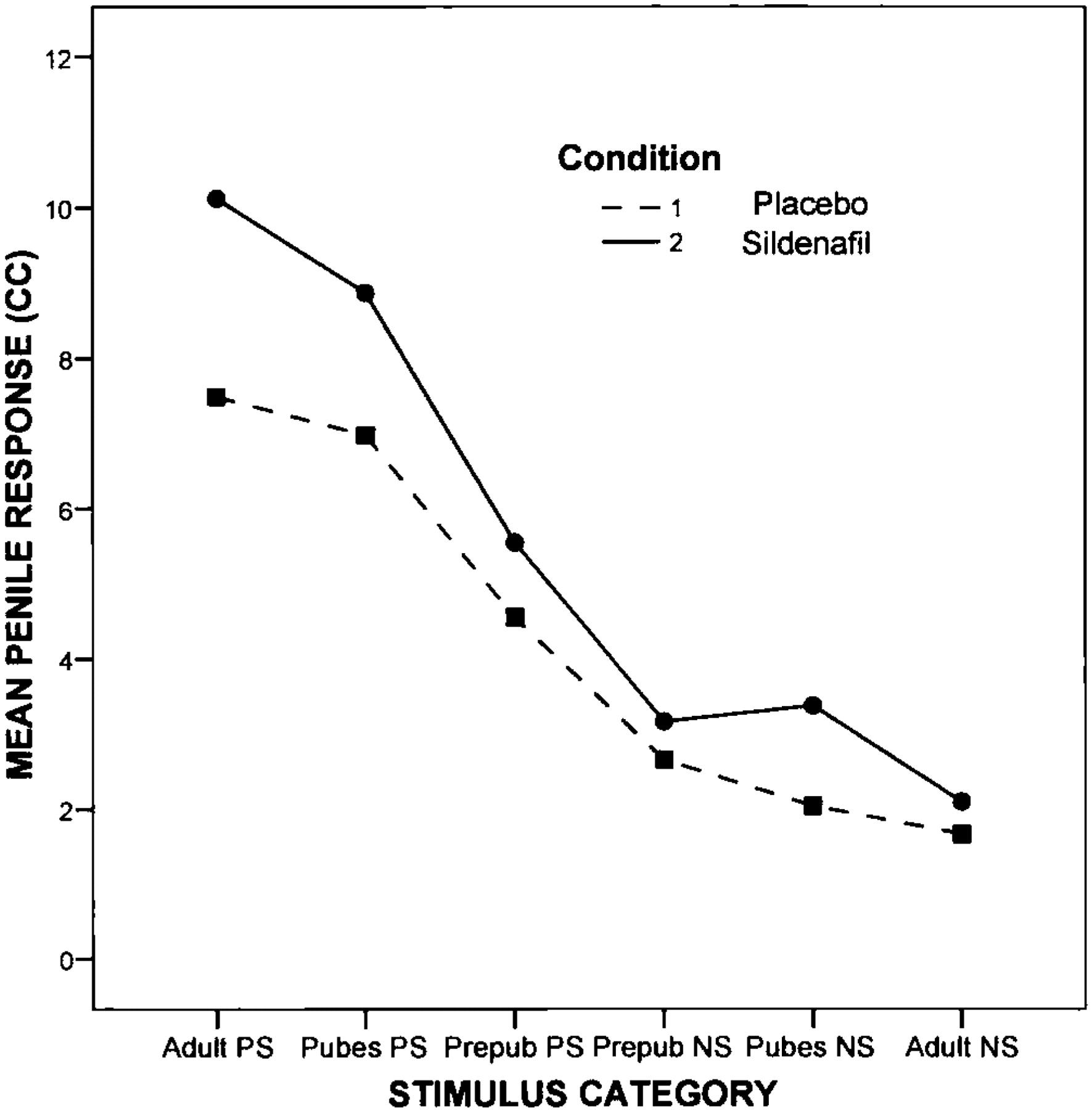
The overall mean output index for all participants in the drug condition was 12.6 ± 9.5 cc, whereas the overall mean output index for participants in the control condition was 10.3 ± 8.3 cc. The difference (2.3 cc) was not statistically significant (t21 = 1.27, p = .22). Figure 1 presents the sample means of the output indices for each stimulus category under both drug and placebo conditions. The stimulus category “adult of preferred sex” referred to the participants' self-reported erotic age preference. All participants had indicated an erotic preference for adults at the outset of the study. Thus, in the case of heterosexual participants, the preferred stimulus category was adult females, while for homosexual participants, the preferred stimuli were adult males. Conversely, the nonpreferred adult stimulus categories for heterosexual and homosexual participants were men and women, respectively. The nonadult stimulus categories were similarly categorized on the basis of whether the target object was of the preferred sex or not. The mean penile response to adults of the preferred sex was 2.6 cc larger in the drug condition than in the placebo condition. This difference was greater than the above-reported difference in output index (2.3 cc); however, it was still nonsignificant (t21 = 1.5, p = .15).

Mean output indices to human stimulus categories under placebo and sildenafil conditions; Adult PS, adult of preferred sex; Pubes PS, pubescent of preferred sex; Prepub PS, prepubescent of preferred sex; Prepub NS, prepubescent of nonpreferred sex; Pubes NS, pubescent of non-preferred sex; Adult NS, adult of nonpreferred sex.
To control for between-subjects variability in output index, treatment effect was expressed as the percentage increase in response for the sildenafil condition relative to the untreated condition. This method of data transformation was used in our previous open-label study of sildenafil and phallometric response.21 Comparing the mean percentage increase against an expected value of zero, we found that sildenafil produced a 50 percent increase in response (t21 = 2.21, p = .038). A 53 percent higher response was observed in the first session compared with the second (t21 = 2.38, p = .027), suggesting that the effect of stimulus novelty (outcomes attributable to the novelty of the initial stimulus) was comparable with the effect of drug treatment.
Table 2includes the correlations between participants' ipsatized penile responses to the seven individual stimulus categories under placebo and their ipsatized penile responses to the same categories under sildenafil. With the exception of the neutral category, all correlations were very high in absolute terms and were statistically significant (p < .001). Participants completed their two phallometric testing sessions on average 5.4 ± 4.2 days apart from one another (range = 2–20 days). An independent-samples t test showed that time to completion of the two sessions did not significantly differ between those who received drug treatment before the first phallometric session or the second (t20 = 1.28, p = .21).
Correlations (Pearson's r) Between Penile Responses to Stimulus Categories With Sildenafil and Placebo
Because our data indicated that there were classification inconsistencies between the results of some participants' two phallometric tests or between the results of one of their tests and their self-report, each participant was classified as pedo/hebephilic or not pedo/hebephilic using the Kurt Freund Laboratory's routine classification rule12,18 for patients or participants undergoing phallometric assessment. Classifying participants as pedo/hebephilic or not involved using each participant's category scores (standardized blood volume changes to each of the seven stimulus categories) to compute a pedophilic index.28 The pedophilic index was calculated as the highest of the four category scores for children (prepubescent girls, pubescent girls, prepubescent boys, and pubescent boys) minus the higher of the two category scores for adults (adult men and women). The cutoff score for dichotomously classifying a participant as pedophilic or nonpedophilic was z > 0.25. That is, participants with a pedophilic index score greater than 0.25 were classified as having pedophilia, whereas those with scores less than or equal to 0.25 were classified as not having pedophilia. This threshold has been the standard in our laboratory for over 15 years. Each participant was classified twice: once using his phallometric data from the placebo condition and once using his data from the sildenafil condition.
There were 15 participants whose phallometric results provided identical classifications for both placebo and drug trials and also confirmed the participants' self-reported teleiophilic orientation (an erotic preference for physically mature adults). Among the remaining 7 participants from the original sample of 22, there were 4 self-reporting teleiophilic participants whose phallometric results obtained under placebo and drug conditions yielded identical deviant classifications. These phallometric classifications were therefore at odds with the participants' self-reported preference for the mature physique. Three of these participants were phallometrically classified as heterosexual hebephiles (individuals with an erotic age preference for pubescent females) with and without sildenafil administration. The fourth participant was twice classified as a homosexual hebephile (an individual with an erotic age preference for pubescent males). Hence, the phallometric results obtained with sildenafil and with placebo were consistent for 19 of the 22 participants. The final three study participants had contradictory phallometric test results: two individuals were classified as teleiophilic under sildenafil and pedo/hebephilic under placebo, while one participant was classified as pedo/hebephilic with sildenafil and teleiophilic with placebo.
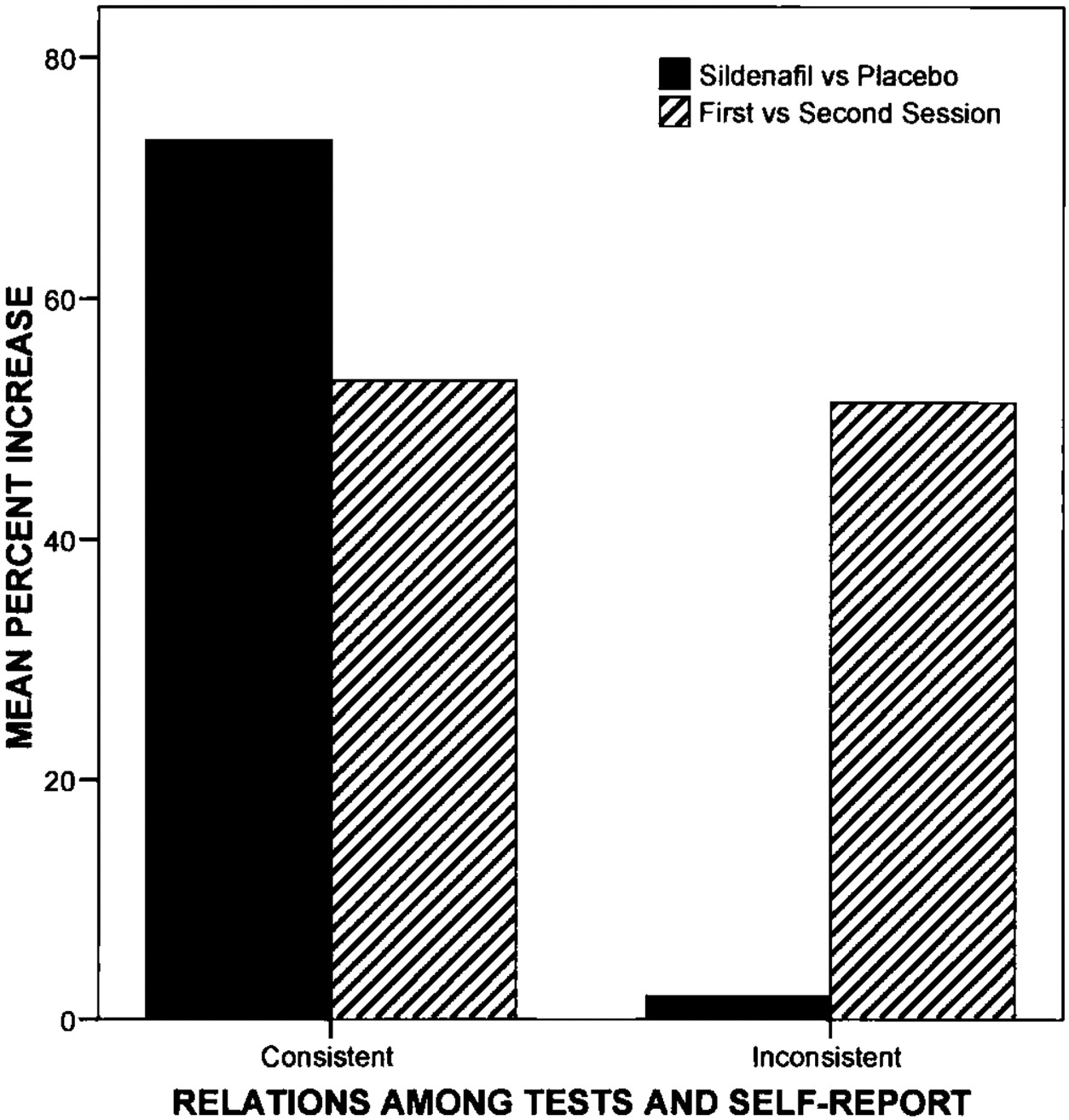
Given the foregoing discrepancy between some participants' self-reported erotic orientation and their phallometric classifications, we evaluated separately the effect of the drug in men whose test results were fully consistent with their self-reported adult preferences (n = 15) and in men whose test results were not fully consistent with their self-reported preferences (n = 7). Similar to our previous analyses, drug effect and stimulus novelty were calculated as percentage increases; observed values were compared against a test value of zero, using one-sample paired t tests. As presented in Figure 2, the consistent participants demonstrated a 73 percent increase in penile response with sildenafil (t14 = 2.42, p = .03). The effect of stimulus novelty, which equated to 53 percent higher penile response during the first testing session, was not statistically significant (t14 = 1.69, p = .11). Among the seven participants whose phallometric results were inconsistent with their self-report, there was a negligible two percent increase in phallometric response under the drug condition (t6 = 0.08, p = .94). This result suggests that sildenafil was less effective in the group of “inconsistent” responders. A 51 percent higher response was observed during the first testing session in this group, which although less than the consistent responders, was marginally statistically significant (t6 = 2.49, p = .047).

Mean percentage increase in peak responses for consistent and inconsistent test responders during sildenafil treatment.
Discussion
The results of the present investigation replicated and expanded on our previous analysis of the effect of sildenafil on phallometric response.21 Participants taking sildenafil in the current study showed a 50 percent increase in phallometric response compared with placebo. In our open-label study, we found that 50 mg of sildenafil citrate increased peak responses by 28 percent. Pharmacodynamic studies indicate that drug dose is the best predictor of functional outcome among patients taking sildenafil for clinical indications.28 That is, higher doses tend to be more efficacious. Indeed, a dose-response study of sildenafil in adult males with ED showed that increased doses resulted in more robust erectile function.29 It was therefore expected that the higher dose of sildenafil used in this study would yield an increased phallometric response in participants compared with that in the earlier investigation. In routine clinical practice, a dose of 100 mg sildenafil is indicated for the treatment of ED.30
Test reliability refers to the consistency of test measures across repeated experiments. If a test is reliable, it will produce similar results in the same participant under identical conditions. Although our study was not specifically designed to assess the reliability of phallometric classification, our data revealed a very high concordance between the phallometric classifications obtained from the two separate tests for each participant. Our confidence in the test's reliability is bolstered by the fact that a high level of agreement between the phallometric classifications obtained from both testing sessions was observed despite experimental manipulation (administration of sildenafil before one of the two tests). The strength of the correlations between penile response to each of the stimulus categories under drug and placebo conditions provides an additional measure of the phallometric test's high reliability. These results indicate that participants responded with similar relative magnitudes to each stimulus category during both tests. The one exception was the neutral category, where the relationship was not significant, because examinees do not respond and are not expected to respond with penile tumescence to photographs of landscapes; where there is no meaningful variability, there can be no meaningful correlation. Both consistent and inconsistent responders showed novelty effects to the phallometric stimuli. Demonstrating reliability of the phallometric classification was a crucial step in this investigation, as any interpretation of the increased penile response occurring under the drug condition hinged on our being able to establish that sildenafil did not distort the participants' classification profiles.
Eighteen percent of our participants self-identified as homosexual. If these individuals had been randomly selected from men in the community, we would expect approximately three percent of the sample to have had a homosexual orientation.31 Although none of our participants indicated an erotic preference for the immature physique, we found that 4 of 22 participants were phallometrically classified as hebephilic from both tests, which appears rather high. While the true prevalence of pedo/hebephilia in the general population is unknown, both conditions are thought to be rare. The high prevalence of hebephilic participants in this study is consistent, however, with that in prior research in men who volunteered to participate in phallometric investigations—men who are very unlikely to constitute a representative cross-section of males in the general population. For instance, Freund and Watson32 reported a 97 percent specificity for obtaining a phallometric classification of pedophilia in men who had sexual offenses against adult women and who also claimed to be gynephiles (individuals with an erotic preference for mature adult women). Yet, the test's specificity for paid volunteers who similarly claimed a preferential attraction to adult women was only 81 percent. The authors surmised that differences in test-taking attitudes between the offenders and volunteers may have accounted for the discrepant results. An alternative explanation posits that the reduced specificity of the test in volunteers was an accurate reflection of an increased prevalence of pedophiles in this group compared with the offender group. Indeed, it has been suggested that the volunteers in Freund and Watson's study produced more pedophilic and hebephilic diagnoses because there were more genuine pedophiles and hebephiles among them.18 Thus, there is good reason to suspect that the four individuals in our study classified as hebephiles did in fact have an anomalous erotic age preference.
Because of the great variability in absolute magnitude of phallometric response among participants, it is probable that the study was underpowered to detect a significant difference between the mean output indices obtained under the control and experimental conditions. However, the absolute magnitude of the increased response observed under sildenafil has potentially important clinical implications. The minimum threshold for making a phallometric diagnosis in our laboratory requires an output index of 1 cc. Recent empirical data from our laboratory have in fact indicated that phallometric classification (deviant or no deviant sexual preference) was no better than chance when a participant's output index failed to reach 1 cc.33 We found that peak response increased by about 2.3 cc with drug treatment. Thus, the amount of blood volume increase observed with 100 mg of sildenafil was more than twice the volume needed to classify participants reliably using phallometry. Placed in a clinical context, these data suggest that men whose output indices fell below the minimum 1 cc level could well be converted to responders with sildenafil pretreatment.
Our investigation was limited to studying older males; furthermore, most of the participants denied having a forensic history. These sample characteristics make generalizing our results to younger, forensic populations difficult. We did not have adequate power to examine a potential order effect of the two conditions on phallometric response, nor were we able to test whether the interaction of phallometric classification and condition (drug versus placebo) influenced response. However, it was never expected that one small study could answer these questions. Future investigations involving larger samples of men with forensic histories would likely be able to overcome these limitations.
Peak response increased significantly during drug treatment in men who claimed a preferential attraction to the mature adult physique and whose self-reported erotic orientations agreed with their phallometric data. Moreover, re-exposure to the identical stimuli did not produce a significant diminution of response. In contrast, sildenafil effected virtually no increase in response among the participants whose self-reported orientations were incongruent with their phallometric results. These findings are consistent with results outlined in a phallometric study of sex offenders that examined the correlation between peak response in individuals with consistent phallometric classification results and those with inconsistent classifications.33 Similar to our investigation, participants underwent phallometric testing on two different occasions. This study did not involve the use of sildenafil. However, the authors found that participants with consistent phallometric test results demonstrated a significantly greater peak response compared with men whose classifications were inconsistent. This result remained significant after controlling for participant response on the first test.
The findings of the present study suggest that the men most likely to benefit from sildenafil pretreatment in phallometric testing may be teleiophiles prone to subthreshold response under normal test conditions. Since the reliability of the phallometric test was unaffected by administering sildenafil to the true teleiophiles, one can appreciate the implications of using this drug to increase the phallometric response in men suspected of being pedophiles but who are in actual fact teleiophiles who have an inadequate response to phallometric stimuli at baseline. Our data also imply that participants with something to conceal, possibly an erotic attraction toward children, may be more likely to resist the effects of sildenafil. This interpretation would, of course, require more research, possibly with instructed faking.
Footnotes
This research was supported by a grant from the American Academy of Psychiatry and the Law Institute for Education and Research to the first author.
Disclosures of financial or other potential conflicts of interest: None.
- American Academy of Psychiatry and the Law





{kind=link}
{kind=link}