


Abstract
Consent to disclosure of confidential information is a cornerstone of the clinician-patient relationship; however, changes in the legal, regulatory, and technological landscape affecting patient confidentiality have brought increasing conflict between ethics-based commitments and the realities of practice. In this pilot study, 119 mental-health clinicians completed a questionnaire that measured levels of disapproval of disclosures of confidential information to various third parties. Clinicians were asked to respond as though they were patients whose information was to be disclosed. Clinicians, taking a patient's perspective, most disapproved of disclosures to anyone who wanted the information and to entities that marketed pharmaceutical, medical, or other products. They were progressively less uncomfortable with disclosures to family members, for educational use without consent but with de-identification, to insurance companies, to pharmacists, to journals, for educational purposes in training other clinicians, and for research. They were least disapproving of disclosures to other clinicians. Based on this initial study of clinicians taking a patient's perspective, clinicians will do well to inform patients about disclosure practices at least as fully as they themselves would want to be informed.
Handling confidential information is addressed early in the course of every clinician's graduate training, but the legal and regulatory landscape changes constantly. Innovations such as The Health Insurance Portability and Accountability Act of 1996 (HIPAA), managed care, and the electronic medical record periodically challenge our understanding of what it means to maintain confidentiality.1,–,3 Keeping pace with externally imposed practice requirements that affect our patients is a perpetual obligation that requires empathic focus and analytic reasoning.4
In this pilot study, we asked clinicians to rate their reactions to hypothetical disclosures of confidential information as if they were patients who were being questioned.5 Results suggest that considering confidentiality in this fashion invokes a reciprocal perspective in which the potential for disclosure is regarded not just in terms of codified ethics, but also with various amounts of personal disapproval. Such experiences remind clinicians that properly managing confidentiality plays a key role in preserving trust, an indispensable component of the treatment relationship.
Three key legal decisions highlight the need for mental health professionals to master the finer points of contemporary confidentiality regulations. In Jaffee v. Redmond,6 a clinical social worker was treating a police officer who was accused of causing the wrongful death of a knife-wielding assailant through the use of allegedly excessive force. Upon discovering this treatment relationship, the plaintiff's attorney demanded the officer's psychotherapy records, which the social worker refused to provide. A federal trial court ruled against the social worker, concluding that there was no “legal justification” for withholding the records; however, the Seventh Circuit Court of Appeals overruled the lower court, maintaining that the records merited protection via a psychotherapist-patient privilege that had been adopted in some form by all 50 states and should also be established in the federal context. The Supreme Court of the United States ultimately affirmed the Seventh Circuit's decision, recognizing that “effective psychotherapy … depends upon an atmosphere of confidence and trust in which the patient is willing to make a frank and complete disclosure of facts, emotions, memories, and fears.”
In Shrager v. Magellan Behavioral Health,7 a health maintenance organization (HMO) instructed a psychiatrist to surrender the complete records of five of his patients, chosen randomly as a part of the HMO's periodic recredentialing process. When the psychiatrist refused to do so without first obtaining his patients' consent, his credentials were not renewed, and he was ultimately dropped as a provider. When the psychiatrist sued the HMO, the trial court ruled that he should be reinstated, with additional provisos that, consistent with state law, the psychiatrist should secure in advance from all patients authorizations for any disclosures to third-party payment sources and that, even when disclosure was subsequently made, the records in question must be redacted with the elimination of such elements as names, addresses, signatures, and other potential identifying information. This finding affirmed the centrality of patient consent as a requirement for releasing protected information.1
In Maryland State Board of Physicians v. Eist,8,–,10 a psychiatrist was fined and threatened with license revocation for refusing to surrender confidential medical records to a state licensing board without the consent of his patients, in the context of highly contested divorce proceedings in which the patients in question were the divorcing mother and two of the couple's children, and in which the complainant was the divorcing father, an attorney. When the psychiatrist sued the board, an administrative judge decided in his favor, and the Maryland Court of Special Appeals, the state's intermediate appellate court, affirmed this decision, maintaining in concurrence with the amicus briefs of 28 professional guilds and patient organizations that the board had failed to meet its burden of establishing an interest in disclosure that outweighed the patients' right to privacy. The board then appealed to the Court of Appeals of Maryland, the state's highest court, which ultimately concluded in a four-to-three decision that the psychiatrist was subject to the board's reprimand and a fine after all. The stated reason for this reversal was not that the lower appellate court had somehow miscalculated the relative importance of disclosure versus privacy, but rather that the psychiatrist, when initially faced with the board's demands, had failed to file, as per advice of counsel, either a motion to quash the board's subpoena or a motion for a protective order—technically the only sources of judicial remedy available to him under Maryland law. At the time that this article was submitted for publication, it was unclear what additional administrative options or appellate relief might be available to the psychiatrist.
For each of the psychotherapists in the preceding cases, a third party was demanding access to confidential information without any opportunity for patients, many of whose personal interests could be quite significantly compromised as a result, either to grant or to withhold their consent for such disclosures. In Jaffee, it was a plaintiff's attorney who was attempting to obtain sensitive information about a criminal defendant. In Shrager, the third party was a private corporation with a fiduciary obligation to its shareholders. In Eist, the demand came from a state agency following, in rote fashion, a policy that ironically was geared toward protection of the patients in question.
In each of these cases, it was a mental health clinician's expressed concern for a patient's welfare—asserted with conviction, and at great professional risk—that forestalled breaches of confidentiality that all three of the deciding courts recognized as constituting a potentially fatal threat to the overall viability of essential mental health services. Clinicians should note that the jurisdictional and topical limitations of each of these decisions ensure that none of them, in and of itself, can be invoked as a universally applicable ban to compel disclosure of medical records. Whether the third party demanding the production of medical records is a plaintiff's attorney, a private corporation, or a state agency, clinicians nationwide face complex and potentially consequential demands from third parties to surrender protected health information (PHI).1,–,3,11
The uncertainty in the law about confidentiality and consent,11 combined with escalating demands for information, drew our attention to the boundary between professional ethics and practices. There is increasing conflict between ethics commitments, such as the Hippocratic Oath (see Appendix I), and the realities of everyday practice.4 We anticipated that the exercise of asking clinicians to think of themselves as patients might broaden their perspectives about psychotherapist-patient privilege, confidentiality, and consent. We hypothesized that clinicians, adopting the patient's perspective, might rate disclosures differently depending on the identified third party. Our instrument measured levels of disapproval with respect to disclosures of PHI to various third parties.
Methods
The instrument was developed by the authors, with modifications suggested by members of the Program in Psychiatry and the Law, Beth Israel Deaconess Medical Center, Harvard Medical School. The Beth Israel Deaconess Medical Center Committee on Clinical Investigations exempted this study from further review.
We presented this pilot study to a group of local psychiatrists, of whom 32 responded. To reach a larger sample we presented the instrument on three list serves: PrograminPsychiatryandtheLaw, PsychiatryandLaw, and PsyLaw-l. Clinicians who subscribed to these list serves were invited to fill out the instrument on the survey website, resulting in 87 more respondents.
Of a total of 119 participants, 47.1 percent were male, and 52.9 percent were female. The mean age was 46.3 years (SD=13.6). The distribution of academic degrees was as follows: MD, 29.4 percent; PhD, 36.1 percent; PsyD, 3.4 percent; MSW, 2.5 percent; JD, 0.8 percent, and “other,” 18.5 percent. We lack more specific information about the type of academic degree held by the respondents who endorsed “other.”
In this pilot instrument, we employed a Rasch analysis to demonstrate the degree of perceived unwillingness to have records about oneself, as a patient, released to various entities.12,–,17 A Rasch analysis locates items conveniently on a linear scale (see Appendix II for details).
A Rasch analysis provides a scale of the discomfort that health care providers in their role as patients have about releasing information about themselves to various third parties. The results of the analysis allow clinicians to benefit from empirical data when confronted with similar situations involving release of their patients' PHI. The Rasch analysis will help determine how great a difference a change in score makes. Consider the difference of one unit between two scores—for example, an item with a score of 1.5 and one with a score of 2.5. For a small range of scores, a difference of 1 would be a big difference, whereas for a large range, it would be a small difference.
The instrument was developed for the purpose of measuring levels of disapproval of disclosures of confidential information to different third parties. Participants rated disclosures to different third parties on a scale of 1 (strongly disagree) to 6 (strongly agree). (See questionnaire instrument regarding disclosures of confidential information in Table 1.)
Summary of Results
Results
Means, standard deviations (SD), t-tests against a neutral value of 3.5 (the mean of possible ratings), and Rasch scores are presented in Table 1. The Rasch scores of the items went from 3.9 (would not authorize strongly) to −1.62 (would agree to authorize), a range of 5.52. That is a wide range for the items, especially when compared with the range of 3.5 for the participants. The Rasch map (Figure 1) shows the extent to which participants do not want information to go to employers on the positive end of the scale, in contrast to their willingness to allow disclosures to pharmacists on the negative end.
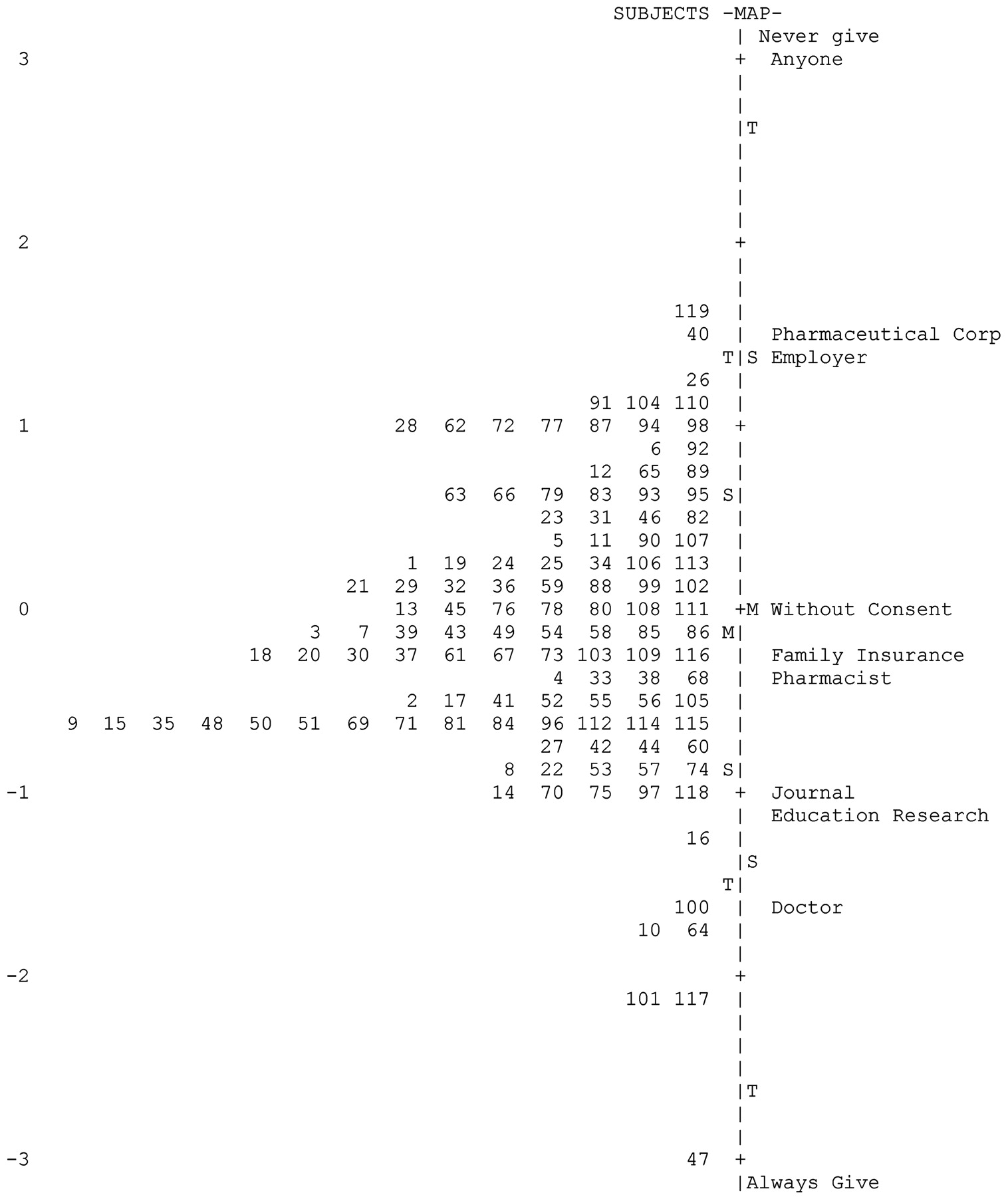
(119 Participants, 11 Items, 6 categories; 3.50 Neutral) The item Rasch scores are on the right side of the y-axis, and the Rasch scores for the participants are on the left. The more the participants were uncomfortable about disclosures, the higher the score appeared on the scale.
Participants most disapproved of releasing information in their clinical record to anyone who might want it. The mean was very far from 3.5, the indifference point (1.07 (SD=0.484); t =−54.538; p < .0005; η=0.981), which is a large effect size. Effect size is a measure of how much of the variability is accounted for by the value in question. Note the extreme value of the Rasch measure of 3.00, meaning that participants were extremely opposed to releasing the information. They were also strongly opposed to releasing information regarding their treatment to companies that market pharmaceuticals, surgical supplies, and other health care products (pharmaceutical: 1.48 (SD=0.913); t =−24.005; p < .0005; η=0.981, Rasch measure=1.50). Participants did not want their clinicians to discuss information regarding their treatment with the participants' employers (employer: 1.61 (SD=0.925); t =−22.198; p < .0005; η=0.899; Rasch measure=1.33).
Participants were less disapproving about having their clinicians use information regarding treatment without obtaining their consent as long as this was for educational purposes and the information was de-identified (M=3.31 (SD=2.033); t =−0.996; p =0.321, which is nonsignificant). The effect size η=0.092 was tiny because the mean was so close to 3.5, the indifference point, with a Rasch measure of only 0.04. Participants were slightly (but nonsignificantly) inclined to disclose information regarding their treatment with members of their family who had expressed concern about their treatment (family: 3.7 (SD=0.691); t =1.306; p =0.194 (NS); η=0.122; Rasch measure=−0.19).
Participants were least disapproving about releasing information in their medical record to their health insurance companies (insurance: 3.83 (SD=1.583); t =1.969; p =.052; with a very small effect size of η=0.206 and a Rasch measure of 0.30). They approved of releasing information in their medical records to their pharmacists regarding medications prescribed for them (pharmacist: 3.92 (SD=1.793); t =2.531; p =.013; with a low effect size of η=0.223; Rasch measure=−0.32).
Participants approved of releasing information about their treatment for purposes of professional articles that their clinicians might write (journals: 4.93 (SD=1.494); t=10.460, p =0.0005; a somewhat large η=0.694; and Rasch measure=1.06). They were in favor of releasing information in their medical record for educational purposes to help train other clinicians (educational: 5.02 (SD=1.420); t =11.652; p =0.0005; with a somewhat large effect size of η=0.731; Rasch measure=−1.14). They were also quite willing to release information in their clinical record as part of research that their clinicians were doing (research: 5.06 (SD=1.355); t =12.551; p =0.0005; and again a somewhat large effect size of η=0.756; and Rasch measure=−1.18). They rather strongly approved of disclosing information in their medical records to other clinicians concerned with their treatment (clinicians: 5.42 (SD=0.964); t =21.589; p =0.0005; with a large effect size of η=0.894, with Rasch measure=−1.67).
A principal component (factor) analysis was also performed. This analysis is a statistical procedure that transforms the possibly correlated variables into a smaller number of uncorrelated variables. These uncorrelated new variables are called principal components. The first principal component accounts for as much of the variability in the data as possible. Three components were extracted. As Table 2 shows, Component 1 accounts for a good deal of the variability of all the items. It consists of research, journals, education without consent, clinicians, family, and pharmacist. Component 2 had much lower factor score loadings and seemed to reflect commercial interests, such as employers and pharmaceutical uses, and the more general release to anyone.
Principal Component Analysis
Discussion
The purpose of this pilot study was to examine clinicians' attitudes about confidentiality when asked to comment from a patient's view. Additional studies will be necessary to determine the extent to which our study population of clinicians is representative of clinicians and of patients in general. Studies involving clinicians from various disciplines, specialties, and subspecialties will be useful. Clinicians with a psychiatry and law background may yield different results than clinicians with little or no forensic background. Further research into the subspecialties of mental health, such as general outpatient treatment, substance abuse, HIV, and genetic studies for early detection of illness, may be important in clarifying the applicability of our findings. Also, the setting of clinical practice may affect attitudes about disclosures. Whether the clinician is in private practice, a community clinic, hospital, correctional facility, or a nursing home may shape attitudes regarding disclosure of PHI.
Such studies can explore whether disapproval about disclosures varies according to discipline, specialty, subspecialty, and setting and whether, regardless of such variables, perspective-taking may enhance awareness about confidentiality and other ethics-based and clinical values, such as informed consent. Ultimately a study involving actual patients who are not clinicians will be useful in determining whether their attitudes are similar to those of clinicians. In a subsequent paper, we will report on the test of a hypothesized correlation among clinicians between the capacity for clinical perspective-taking and sophistication regarding disclosure of PHI and informed consent. Our preliminary results suggest that, just as perspective-taking correlates with awareness about confidentiality, it also correlates with a greater degree of awareness about informed consent. Assisting the patient with the granting of consent for disclosure of PHI is a specific instance of the informed-consent process.
As shown in detail in the Results section, clinicians were most uncomfortable about disclosures to anyone in general who wanted the information. Clinicians were progressively less uncomfortable consenting to disclosures of personal information to family members, education without consent, insurance companies, pharmacists, journals, clinician education, and research. They were least disapproving about disclosures to other clinicians.
Notably, the only disclosure for which consent was not presumed was education without consent. One might expect disapproval of the release of PHI for any purposes without first obtaining consent. The fact that such disclosures are rated in the midrange of discomfort may be understandable on the basis that such information would be de-identified. Clinicians in our study seemed willing to entertain disclosures of PHI without consent, so long as information was sufficiently de-identified. This tolerance may be a function of educational traditions and thus may not extend to other patient populations.
The finding that clinicians regarded themselves as the most trustworthy recipients of PHI may be an artifact of the study sample and should be compared with findings obtained in broader populations of patients who are not themselves clinicians. If the finding were confirmed, it would be evidence of the trust patients still have in clinicians and would underscore the importance of maintaining that trust.
Conclusions
The notion of consent is a fundamental of ethics reflected in the religious doctrines, social conventions, and professional codes of all cultures in which basic human rights are respected.18,–,22 Consent to disclosure of confidential information is one of the cornerstone ethics principles of the clinician-patient relationship in which the dignity and autonomy of the patient are held in the highest regard.4 As clinicians imagine themselves in the intellectual and emotional sphere of their patients, integrating perspectives of their patients with their own, they no longer simply refer to abstract principles regarding disclosures of PHI, but also are informed by their personal experiences and concerns.
Recent developments in health care privacy are in conflict with traditional values regarding consent. These developments include the increasing adoption of interoperable electronic medical records, increasing demands for PHI without patient consent, and HIPAA. Although HIPAA claims to protect privacy, it actually allows disclosure without consent for broadly defined purposes.23
Rather than accepting the deterioration of confidentiality and the erosion of privacy, or acceding to a compromise, clinicians should uphold confidentiality as an unwavering professional value.24 If there is an ethics-based imperative predicated on the trust inherent in the clinician-patient relationship, it is to uphold this value as much as possible by informing patients about changes in disclosure practices, at least as fully as clinicians would want to be informed if they were patients.
Trust is the pre-eminent concern bearing on the decision of whether to release PHI. A patient may consent to disclose confidential information to third parties for legitimate purposes, as a consequence of which that information may then become available to other parties without the patient's knowledge or consent. Clinicians should therefore be circumspect about their medical record entries and observe the principle of parsimony, entering only that amount of information that is necessary for legitimate billing procedures and medical record keeping. Psychotherapy notes are recorded (in any medium) by a mental health professional documenting or analyzing the contents of conversation during a private counseling session or a group, joint, or family counseling session. If kept separately from the rest of the record, they are afforded special privacy protections and cannot be disclosed without the patient's consent, as specified in HIPAA. Private contracting must be preserved as an option for some patients to maximize privacy by bypassing third parties.
Possible technological remedies include the implementation of a patient-centered electronic medical record by which clinical information would be protected and directed only by the patient (or surrogate) to intended recipients. Encryption that the patient controls, the partitioning of protected health information, logging access, and audit trails would provide additional layers of security that would significantly strengthen privacy protections. Security measures in our view should become the centerpiece of health information infrastructure before the adoption of meaningful-use requirements in the Final Rule of The Health Information Technology for Economic and Clinical Health (HITECH) Act.
Clinicians might also consider advocating for stronger state and national laws to protect confidentiality and opposing those laws that eliminate or undermine patient consent. When clinicians are pressured or enticed by state agencies, private health care corporations, a lawyer issuing a subpoena to disclose PHI without the patient's consent, or a judicial order, they should pause and reflect before responding. In these circumstances it may be appropriate to seek consultation from professional organizations, colleagues, and an attorney. Finally, when spectacular violations of confidentiality occur in which thousands of medical records are released into the public domain, as occurs with laptop and hard-drive breaches, such disasters should be cited in favor of stronger confidentiality legislation, advances in privacy technology, and legal redress.
Educators should stress to students the signal importance of confidentiality as a prerequisite of trust in the clinician-patient relationship. They should review applicable laws and commonplace risks involved in handling PHI, including the accidental release of PHI via the loss or theft of electronic media. Clinicians in training should also be exposed to the concept of perspective taking. By developing the capacity to imagine the patient's perspective, clinicians will be in a better position to consider difficult questions about the disclosure of PHI and other clinical and ethics-related judgments.
Acknowledgments
The authors thank Thomas G. Gutheil, Patrice Marie Miller, Archie Brodsky, and researchers and participants in the Program in Psychiatry and the Law, Beth Israel Deaconess Medical Center, Harvard Medical School. We also thank Wilson Shafter Shirley III for his help and scholarly advice.
Appendix
Appendix I: From the Hippocratic Oath
I will respect the privacy of my patients, for their problems are not disclosed to me that the world may know.
What I may see or hear in the course of the treatment or even outside of the treatment in regard to the life of men, which on no account one must spread abroad, I will keep to myself, holding such things shameful to be spoken about.
Appendix
Appendix II: The Rasch Model of Analysis
To understand the methodology of this study and the results obtained, a basic knowledge of Rasch scales is helpful. A Rasch analysis has been used in a variety of disciplines and in a wide range of research.
A Rasch model of analysis produces an objective, additive scale that is independent of the particular items used and of the particular participants tested. The Rasch analysis can be used to analyze a large variety of human sciences data.11,–,16 For example, through the use of probabilistic equations, this model converts raw ratings of items into scales that have equal intervals. This analysis is particularly effective when the raw data are entered as values on a continuous scale (either participants were asked to rate an item on a scale, or nonscale answers were coded with continuous whole number integers). Once the raw data input is coded in a uniform manner (percentages, words, and decimals are all entered, or coded, as whole numbers), the Rasch analysis converts these codes into small numeric values (generally between –4 and +4), according to an order of magnitude. A scale will then be produced, on which each item (which is coded for and entered as a raw data point) is placed according to its Rasch rating or scaled score.
Such a scale can then be used as a type of objective ruler against which to measure the data on items as well as on respondents' ratings. The ruler-like properties of this scale are what provide its advantage over other scaling techniques. For example, the scale is made up of equally spaced, continuous intervals. Doubling the distance from 1 to 2 results in an equivalent magnitude of change as doubling the distance from 2 to 4. Also, from a statistical standpoint, this scale provides a linear interval measure. As a result, a change of 1 in how much a person says he is willing to divulge carries the same weight from −2 to −1 as it does from 0 to +1. As with a ruler, a change in length of one inch, either from two to three inches or from three to four inches, is the same.
Footnotes
-
Disclosures of financial or other potential conflicts of interest: None.
- © 2011 American Academy of Psychiatry and the Law





{kind=link}