


Abstract
State psychiatric hospitals are increasingly populated by forensic patients. In New York State, the growth in the forensic population is largely attributable to increased lengths of stay of patients deemed not guilty by reason of insanity (NGRI). This research was conducted to determine whether longer periods of hospitalization are associated with better outcomes in the community, as measured by re-arrest for any offense and re-arrest for violence. The sample included 386 NGRI patients released into the community in New York State. A Cox regression proportional hazards model was used to assess the unique effects of length of hospitalization on re-arrest. The results showed that the length of treatment had little effect on either measure of re-arrest. Re-arrest was largely explained by demographics and prior criminal histories.
In recent years, state mental health agencies throughout the United States have witnessed an increase in both the number and proportion of persons occupying state-operated inpatient beds who have been referred for hospitalization by the criminal justice system. In state-level data submitted to the Center for Mental Health Services for the period 2002 through 2005, 11 states reported an increase in admissions to state-operated inpatient programs and largely attributed the growth to an increase in forensic admissions.1 As noted by Lamb and Weinberger, over the past few decades a “profound paradigm or model shift in the care of persons with severe mental illness” (Ref. 2, p 529) has occurred, where access to inpatient care is through jails or prisons.
This trend also is occurring in New York State (NYS), with forensic referrals comprising an increasing portion of the state's civil (nonforensic) psychiatric hospital census. Between 1998 and 2008, the percentage of the civil hospital census contributed by forensic referrals increased from 11 to 17 percent. For our purposes, those identified as forensic referrals include persons committed to the care and treatment of the NYS Office of Mental Health (OMH) as Not Responsible for Criminal Conduct Due to Mental Disease or Defect pursuant to Criminal Procedure Law (CPL) § 330.20 (1980) (NGRI), those committed after being found incompetent to stand trial for criminal offenses (both felony and misdemeanor offenses), and persons released from prison and subsequently admitted to a state civil psychiatric facility without any intervening community-based mental health contact. Slightly more than 40 percent of the forensic-referred beds are occupied by persons subject to New York's NGRI statute, and that statistic has remained unchanged over the past decade.
The increased prevalence of NGRI patients within civil hospitals in New York State is a result of their increasing length of stay (LOS) in the hospital. This increased LOS has occurred in both secure and civil hospitals. While the number of NGRI admissions to hospitals in New York State has declined over the past three decades from a high of 77 in 1982 to a low of 22 in 2008, the length of hospitalization of these individuals has increased significantly.3 For example, more than 40 percent of those admitted in the 1980s were released into the community within seven years of admission.3 In the 1990s, only 21 percent of the admissions were released into the community within seven years.3 At the start of the last decade, only eight percent of admissions were released within a seven-year period.3
The increasing LOS of NGRI patients and its associated impact on hospital census raises the question of whether longer periods of hospitalization produce better outcomes in terms of reduced recidivism subsequent to release into the community. Prior research on recidivism among mentally ill offenders has identified numerous correlates of recidivism, but has given relatively little attention to length of hospitalization.
Early research showed little correlation between mental illness and criminal behavior. For example, a 1982 review of research examining the relationship between mental illness and crime concluded that mental illness was unrelated to criminal behavior and that the predictors of crime among the mentally ill were the same static factors that predicted crime within the general population (e.g., age, gender, race, social class, and prior criminality).4 Similarly, the MacArthur Violence Risk Assessment Study, conducted during the early 1990s, found that rates of violence among samples of persons released from acute inpatient facilities were similar to those of the general population in the communities to which the patients returned.5 The MacArthur Study did show a correlation between diagnoses of psychopathy and substance abuse and violence.
More recent meta-analyses have supported the notion that factors that predict violence among the mentally ill are similar to those that predict it within the larger population. A meta-analysis of research on recidivism among mentally disordered offenders found that measures of criminal history, demographics, and deviant lifestyles were more predictive of recidivism and violent recidivism than were clinical measures.6 More specifically, individuals who were young, male, and single recidivated more often, as did those with longer general and violent criminal histories. With regard to criminal histories, it was the culmination of events within the history, rather than the presence of any single type of crime, that predicted future reoffending. Among the measures of deviant lifestyles, family problems and substance abuse were more strongly related to general recidivism than were the measures of education and employment. Clinical variables, as a group, were only weakly related to recidivism. Antisocial personality was positively related to both types of recidivism, as was the number of prior hospital admissions. Notably, a diagnosis of psychosis or mood disorder was either unrelated to or inversely related to the measures of recidivism. Perhaps most relevant to the present research, the authors found that length of hospitalization was weakly and positively correlated with general recidivism and weakly and negatively correlated with violent recidivism.
More recent research from the United Kingdom,7 Sweden,8 Australia,9 and the United States,10 lends further support to the general findings that criminal history, age, gender, and diagnoses of antisocial personality are the strongest determinants of any re-arrest and re-arrest for violence among nonmentally ill and mentally ill populations. While psychosis and other serious mental illnesses may play a part in violence under some circumstances,11 these characteristics do not appear to predict recidivism among an already criminally involved population.
Despite the research findings that show a weak and inconsistent relationship between length of hospitalization and recidivism among mentally ill offenders in general, NYS has exhibited a strong trend toward longer periods of hospitalization for NGRI patients. Several factors may have contributed to the growing LOS for NGRI patients, including a multi-tiered review of the movement of NGRIs through the phases of treatment, emerging case law that has guided those decisions, and the introduction of structured risk assessment coupled with a reduced tolerance for risk. Each of these factors will be briefly summarized, followed by a retrospective analysis of a release cohort of persons found NGRI in an effort to identify correlates of recidivism and to assess the relationship between LOS and recidivism.
NGRI Defendants in New York State
New York's Insanity Defense Reform Act of 1980 introduced a bifurcated process for the disposition and subsequent course of care and treatment of persons found NGRI. Upon a verdict or plea of NGRI, individuals are remanded to the custody of the Commissioner of the OMH at a secure facility to determine whether they require hospitalization in a secure forensic facility (Track I), hospitalization in a civil facility (Track II), or outpatient care in the community (Track III). Most NGRI adjudications result in Track I placements in which the individual begins a course of treatment in a secure hospital and, with court oversight, is gradually stepped down to a civil hospital before being released to outpatient care. Clinical recommendations to advance a patient to the next level of care are proffered by the treating clinicians, reviewed by OMH Central Office, and decided on by the court with jurisdiction. A recommendation to retain an individual at the current level of care or advance him to the next phase is judged based on a preponderance of the evidence standard, is usually agreed to by the trial court, and is rarely overturned at the appellate level. Thus, the recommendations of treating clinicians and OMH Central Office staff strongly influence the length of treatment at each treatment phase.
Treatment recommendations in NGRI cases are, in turn, influenced by case law and the evolving science of risk assessment. In March 1995, the New York State Court of Appeals (New York's highest court) issued what most practitioners serving this population consider to be a seminal decision. In the Matter of George L.,12 the court set forth the criteria for assessing dangerousness that practitioners must address in their recommendations for transferring NGRI patients from a secure to a civil psychiatric hospital. Among the factors to be considered in the assessment are prior relapses into violent behavior, a history of substance abuse or dangerous activities, the need for medication to control violent tendencies, and the nature and recency of the criminal act that led to the original commitment. The court also endorsed a presumption that the mental illness that led to the criminal act continues after the plea or verdict of NGRI and that dangerousness assessments should not be limited to a point in time but rather should be contextual and prospective in nature. This decision had a significant impact on the assessment of risk for Track I patients, as it required not merely showing that the individual is no longer symptomatic, but also that the risk factors that lead to the patient's decompensation are, and will very likely remain, abated.
Coupled with the George L. decision was OMH's administrative decision in 1997 to utilize the HCR-20 risk assessment instrument. The HCR-20 is a structured-judgment risk assessment instrument that is frequently used in forensic populations. It includes a scale of 10 historical domains, 5 clinical domains, and 5 risk management items that the research literature suggests are related to violence in a forensic mental health population. The decision to use the HCR-20 was, in part, an attempt to implement the George L. criteria through a validated risk assessment instrument. Though not a “perfect fit” with the court of appeal's decision, the HCR-20 provides both contextual and longitudinal perspectives on violence risk assessment as well as a focus on risk management strategies that program managers felt was a practical approach to implementing the tenets of case law. The OMH conducted systemwide training on the use of the HCR-20 and incorporated the 20 domains throughout its multi-tiered review process. The net conclusion was that all petitions submitted to court since the adoption of this risk assessment instrument should address all risk factors identified in the HCR-20 assessment.
In summary, the decision to advance a patient from a secure facility to a civil hospital and thereafter to the community became more structured and complex over time. It also occurred within a sociopolitical context in which the system became increasingly risk aversive. The question that heretofore remained unanswered was whether this change affected recidivism upon release into the community. This research was conducted to answer that question and to begin to assess the cost benefit associated with longer periods of hospitalization for the NGRI population.
Participant Selection
The sample included all NGRI patients committed to a secure psychiatric facility in NYS on or after January 1, 1980, and released from hospitalization by March 31, 2007. This research was approved by the OMH Institutional Review Board. Pre-1980 commitments were excluded from the sample because OMH did not have the authority to access criminal history information for adjudications occurring before that period.
There were 440 individuals in the sample, 51 (11.2%) of whom were excluded from the analysis because they could not be linked to the state's criminal history database due to either an inaccurate criminal record identification number or missing or sealed adjudication records in the state's criminal history repository. Another three cases were removed from the sample due to missing data on other variables included in the research. Of the remaining 386 cases, 37 percent had been released during the 1980s, 39 percent during the 1990s, and the remainder in the year 2000 or later. These individuals were first hospitalized in a secure treatment facility and later stepped down to a nonsecure hospital before their release into the community.
Data Sources
Data were collected from the Mental Health Automated Record System (MHARS) and the Legally Oriented Forensic Tracking System (LOFTS) databases maintained by OMH and the State's Computerized Criminal History (CCH) database operated by the NYS Division of Criminal Justice Services (DCJS). The MHARS provides data on all hospitalizations in State-operated psychiatric facilities, as well as corresponding outpatient services. The LOFTS database maintains nonclinical, court-related, and other procedural data on cases admitted to state psychiatric facilities pursuant to an NGRI finding or a finding of incompetent to stand trial (CPL 730). The LOFTS file includes the law enforcement-generated New York State Identification (NYSID) numbers that facilitated the link between the OMH data and records maintained in the CCH. CCH records are maintained on all fingerprinted arrests, which include all misdemeanor and felony-level charges.
Measures
Predictor Variables
The predictor variable of primary interest in this study is the number of years someone was hospitalized as an NGRI admission. Six percent of the releases had more than one hospitalization episode associated with NGRI disposition and, when that occurred, the first episode of hospitalization (from admission in secure to release from civil) was used as the referent hospitalization.
Other predictor variables include demographics (gender and age), prior psychiatric hospitalizations, prior arrest and sentencing histories, arrest while hospitalized, and prerelease diagnoses. Prior psychiatric hospitalization episodes were drawn from MHARS and included only stays in nonforensic, state-operated psychiatric facilities. Preadmission forensic stays were excluded, as they were largely related to the NGRI event and were often intended to restore competence rather than to provide more comprehensive treatment. The hospital stays were summed to create a measure of the total number of years of state-operated psychiatric hospitalization before the NGRI admission.
Prior arrest measures included arrests that occurred before the NGRI admission and thus included the event underlying the admission itself. Prior arrests were measured variously as the sum of all arrests, the sum of arrests for violent crimes, and the number of different types of arrests (a diversity measure). Violent crime was defined through the use of the FBI's classification system and included homicide, robbery, sexual assault (rape and other sexual assaults), arson, kidnapping, and assault (aggravated and simple). The measure of diversity of criminal history was constructed by assigning a point when one of the following offenses occurred in the criminal history and totaling the results to create a diversity scale that ranged from one to eight: homicide, robbery, sex offense, theft, drug offense, driving while intoxicated (DWI), burglary and assault. The seriousness of the criminal history also was measured through a combined count of the number of jail and prison sentences in the criminal history before the NGRI admission.
The criminal history record was similarly used to measure arrests that occurred during the course of NGRI hospitalization. While such arrests are relatively rare, they may occur when the patient commits a particularly violent act, such as a serious assault on a staff member or other patient. These assaults always present treatment quandaries, given that assaultive behavior can be a symptom of active mental illness. This arrest measure was distinguished from the preadmission arrests, as it is arguably qualitatively different from arrests that occur in the community.
Measures of prerelease diagnoses included diagnoses of antisocial personality disorder, psychosis, and substance abuse any time before release into the community (including diagnoses from pre-NGRI admissions). Primary and secondary diagnoses associated with all hospital admissions and discharges were reviewed to create the diagnostic measures.
Dependent Variables
Two measures of recidivism served as the dependent variables, including whether the individual was re-arrested for any offense and a violent offense, subsequent to being released into the community. The definition of violent offense was identical to that used for the criminal history measure.
Results
Profile of Subjects
More than 80 percent of the subjects were males and approximately two-thirds were between the ages of 30 and 54 at the time of their NGRI admission (Table 1). They averaged more than three arrests before the admission, but the distribution was skewed, with 43 percent showing a single arrest (presumably the offense for which they were later hospitalized). Approximately half of the prior arrests involved violence and one of every six arrests resulted in a term of incarceration.
Profile of Sample
Nearly half of the subjects had a diagnosis of substance abuse disorder before their release into the community and almost one-fourth had a diagnosis of antisocial personality disorder. Most (83%) also carried a diagnosis of a psychotic disorder. These diagnoses either emerged during their course of inpatient treatment as an NGRI or during an earlier hospitalization. The subjects averaged almost a year of hospitalization before the NGRI admission, though 44 percent showed no prior hospitalization.
These NGRI admissions were hospitalized for an average of 6.33 years before release into the community. The length of hospitalization was strongly and positively associated with the time of release. While this association is partially an artifact of the exclusion of subjects admitted before 1980, as noted infra, the actual LOS of admission cohorts did increase over time.
The follow-up period for the recidivism measure ranged from less than a year to more than 26 years, with an average of 14 years. Eighty-seven percent of the sample had been released more than three years before the extraction of re-arrest data from the state's central repository. Twenty-one percent of the study participants had one or more arrests in the postrelease period, and 11 percent had one or more arrests for violence.
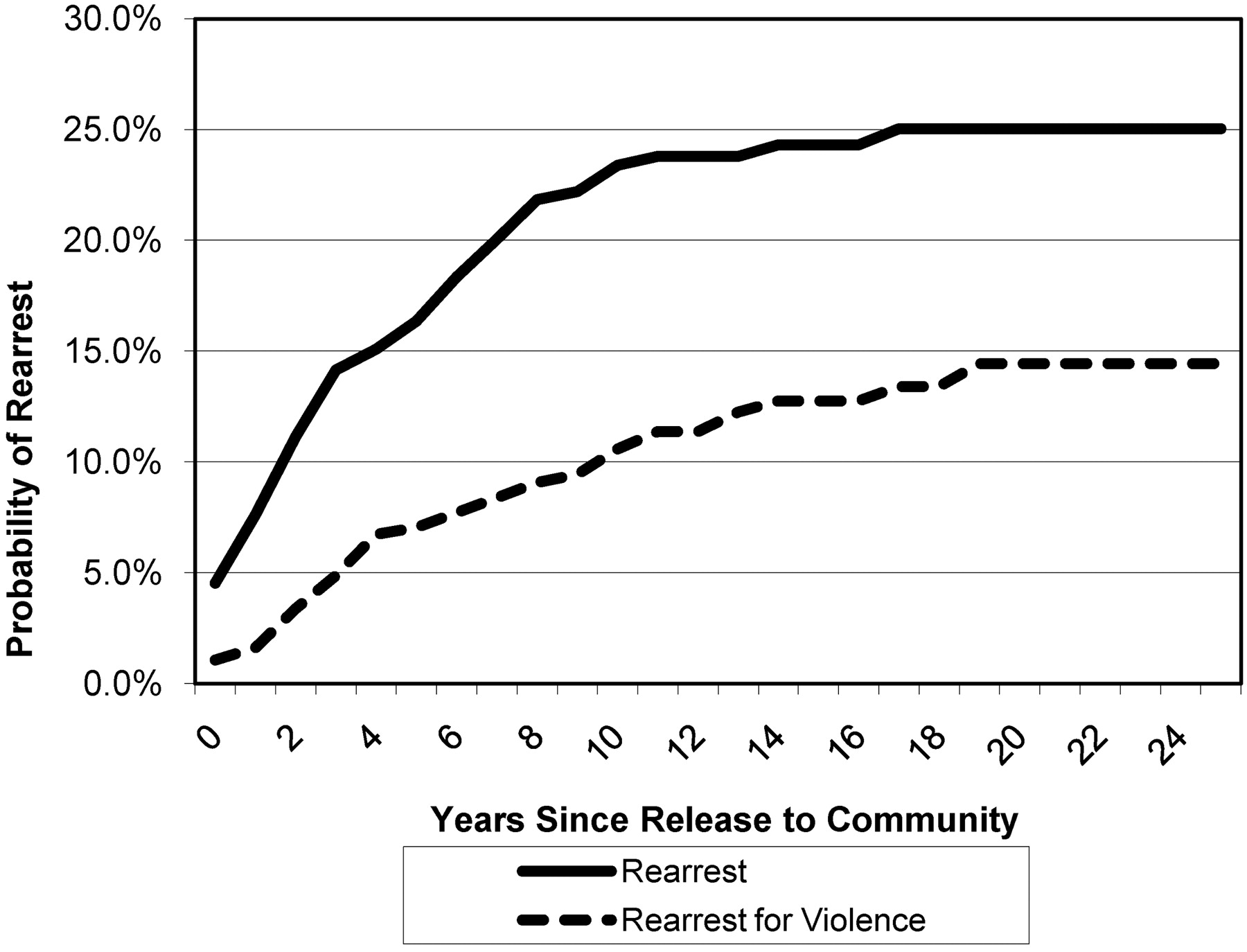
A survival curve of time to re-arrest revealed that 11 percent are re-arrested for any offense and 3 percent are re-arrested for a violent offense within three years of release. By the five-year mark, re-arrests had increased to 16 percent for any re-arrest and 7 percent for arrests for violence. Figure 1 shows the probability of any re-arrest and of re-arrest for violence over time (one minus survival function).
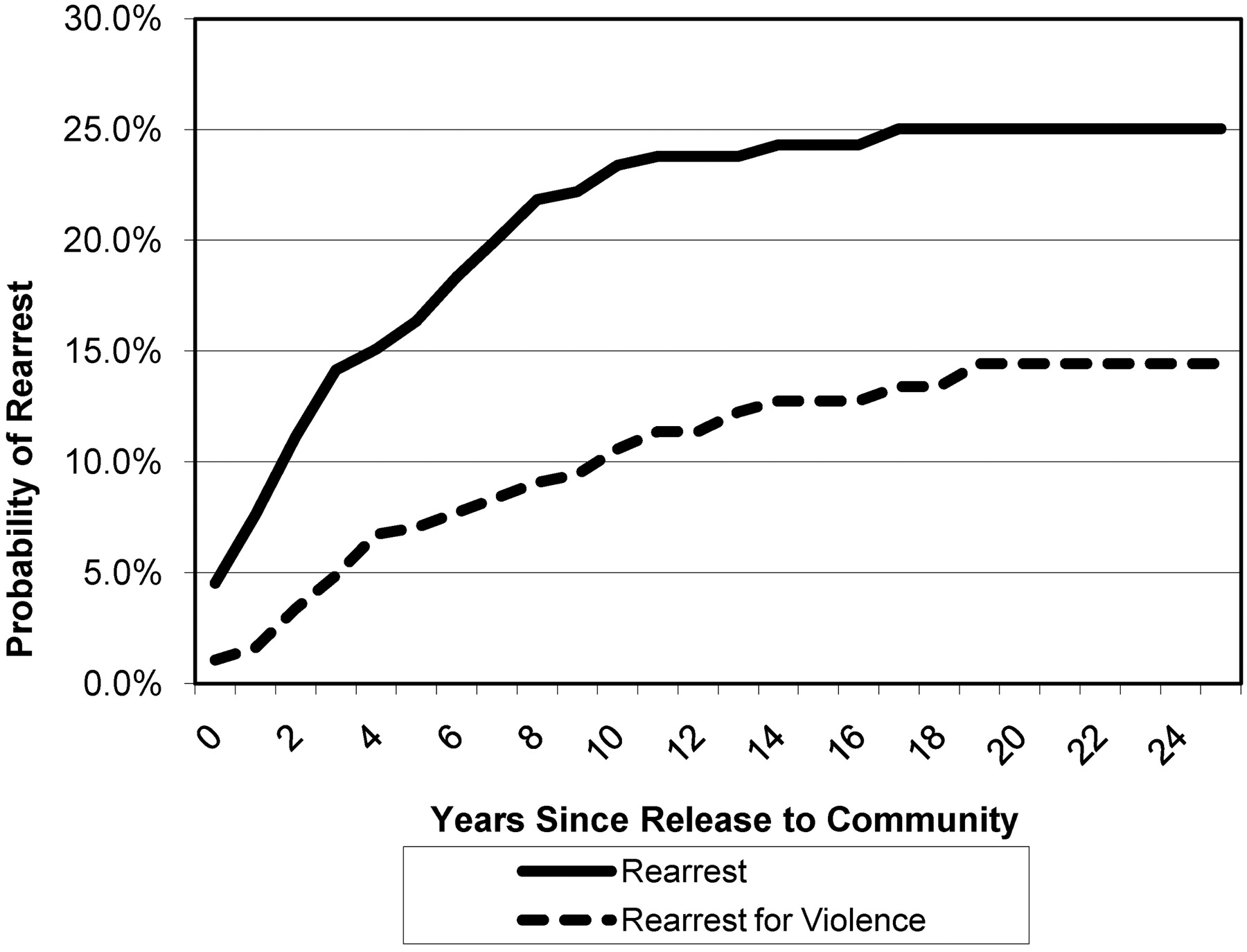
Survival estimates of rates of re-arrest and re-arrest for violence among NGRI releases.
Multivariate Analysis
A Cox proportional hazards regression model was used to assess the unique effects of length of hospitalization on recidivism, after controlling for the various measures of criminal and psychiatric history. The model development occurred in two stages. All predictor variables other than length of hospitalization were entered into the equation in stage one, followed by entry of the predictor variable of length of hospitalization.
Cox regression is a form of survival analysis. It is used to measure the effect of independent variables on a dependent variable that represents the amount of time a specific event takes to occur. Survival analysis is used when subjects have been at risk of the occurrence of an event for various amounts of time. Rather than exclude subjects that were not at risk for a given time, survival analysis creates survival estimates based on outcome information from all subjects, taking into account their time at risk. Cox regression does similarly, but allows for independent variables to be added to the analysis. It does presume that the effects of independent variables on a dependent variable are constant over time.
Model for Any Re-arrest
The initial regression model for the prediction of any re-arrest yielded a significant goodness-of-fit statistic for likelihood ratios (χ2 = 73.8, df = 9, p = .001, N = 385). Length of hospitalization was then added to the model and increased the chi-square by 7.6, a statistically significant increase at the .01 level. Thus, length of hospitalization did appear to predict re-arrest. The effect of length of hospitalization on re-arrest was confounded, however, by a relatively high positive correlation (r = .62) between length of hospitalization and date of release, a variable that also was predictive of re-arrest. When date of release was added to the prediction model, it was predictive of re-arrest, and length of hospitalization lost all significance. The relatively high correlation between date of release and length of hospitalization is due to combined effects of sample selection (the sample was limited to cases of admission after 1979, so that releases occurring in the 1980s were disproportionately short-term stays) and real increases in lengths of stay over time. The confounded effects of length of hospitalization and date of release on re-arrest are difficult to disentangle. Rather than maintaining date of release in the prediction model, we chose to exclude it, but we revisit the decision in the discussion section of this article.
The model was then trimmed of all nonsignificant covariates, resulting in a chi-square of 76.6 with 5 df. The assumption of proportional hazard was confirmed by plotting the partial residuals for each covariate against survival time. Four variables emerged as significant predictors of re-arrest, along with the variable of length of hospitalization. The significant covariates included gender, age at release, antisocial personality diagnosis, and re-arrest while hospitalized as an NGRI. The effect of length of hospitalization on re-arrest was somewhat curvilinear. More specifically, while those with relatively short stays in the hospital were re-arrested at higher rates than those with longer stays, the effect of additional years in treatment declined by the third year. That being said, a log transformation of the length of hospitalization measure did not significantly improve the predictive value of the model.
After survival curves for each year in treatment were reviewed, the treatment was grouped into four categories (rounded to the nearest whole number): zero to two years (n = 71), three to five years (n = 132), six to eight years (n = 93), and nine or more years (n = 90). These periods were selected because they best represented the periods exhibiting notable changes in re-arrest rates. The results appear in Table 2. The reference group on the categorical length of hospitalization measure comprised subjects who were in NGRI inpatient treatment for nine years or more. This group showed a statistically significant lower risk of re-arrest than persons who were treated for zero to two years, but showed no statistically significant improvement over those treated three to five or six to eight years. While the survival curves of the two intermediate length of hospitalization groups did fall between the lowest and highest groups, the differences were too modest to reach statistical significance, given the limited sample size. Moreover, the relatively little difference between the two intermediate length of treatment groups is notable. Nonetheless, if we had larger samples, the difference in rates of re-arrest over time between the long-term treatment group and the mid-range groups might reach statistical significance.
Result of Cox Regression Analysis of Correlates of Rearrest
The results show that after adjustment for all other covariates in the model, being male increased the hazard of re-arrest by 398 percent, having a diagnosis of antisocial personality increased the hazard of being re-arrested by 103 percent, being arrested while hospitalized increased the hazard by 88 percent, and each year of increased age at the time of release decreased the hazard by 5 percent. Finally, being in treatment for zero to two years increased the hazard of re-arrest by a 235 percent relative to those who were in treatment for nine years or more, while those in treatment for three to five years and six to eight years were not significantly different from persons in treatment nine years or more.
Figure 2 shows the probability of the arrest function of this model when other predictor variables are set at their means. As noted above, the difference between the top and bottom curves was the only one to reach statistical significance. When the analysis was limited to males only, the results were the same.

Estimate of re-arrest by time in treatment (at means of covariates).
Model for Re-arrest for Violence
Approximately half of the re-arrests of this sample involved violence, as previously defined. We employed a similar process to build a model for the prediction of re-arrest for violence, including an analysis of partial residuals to confirm the assumption of proportional hazard. Most of the same predictor variables were utilized, but the number of prior arrests for violence replaced the measure of all prior arrests, and females were excluded from the analysis, due to the absence of any re-arrest for violence among the 68 female NGRI discharges. Clearly, gender is the strongest predictor of re-arrest, regardless of the precise re-arrest measure.
Only two predictor variables, number of prior arrests for violence and age at release, emerged as significantly predictive of re-arrest for violence. The hazard of re-arrest for violence increased 32 percent for each prior arrest for violence and decreased approximately 8 percent for each year of increased age at the time of release (Table 3). Length of hospitalization added no predictive power to the equation, regardless of whether expressed as a continuous variable or a categorical variable, as described above. While those in treatment for zero to two years showed the highest rates of failure, the differences were not sufficient to reach statistical significance. The other three groups had very similar trajectories, and the differences were neither statistically significant nor in the expected direction (Fig. 3).
Result of Cox Regression Analysis of Correlates of Rearrest for Violence
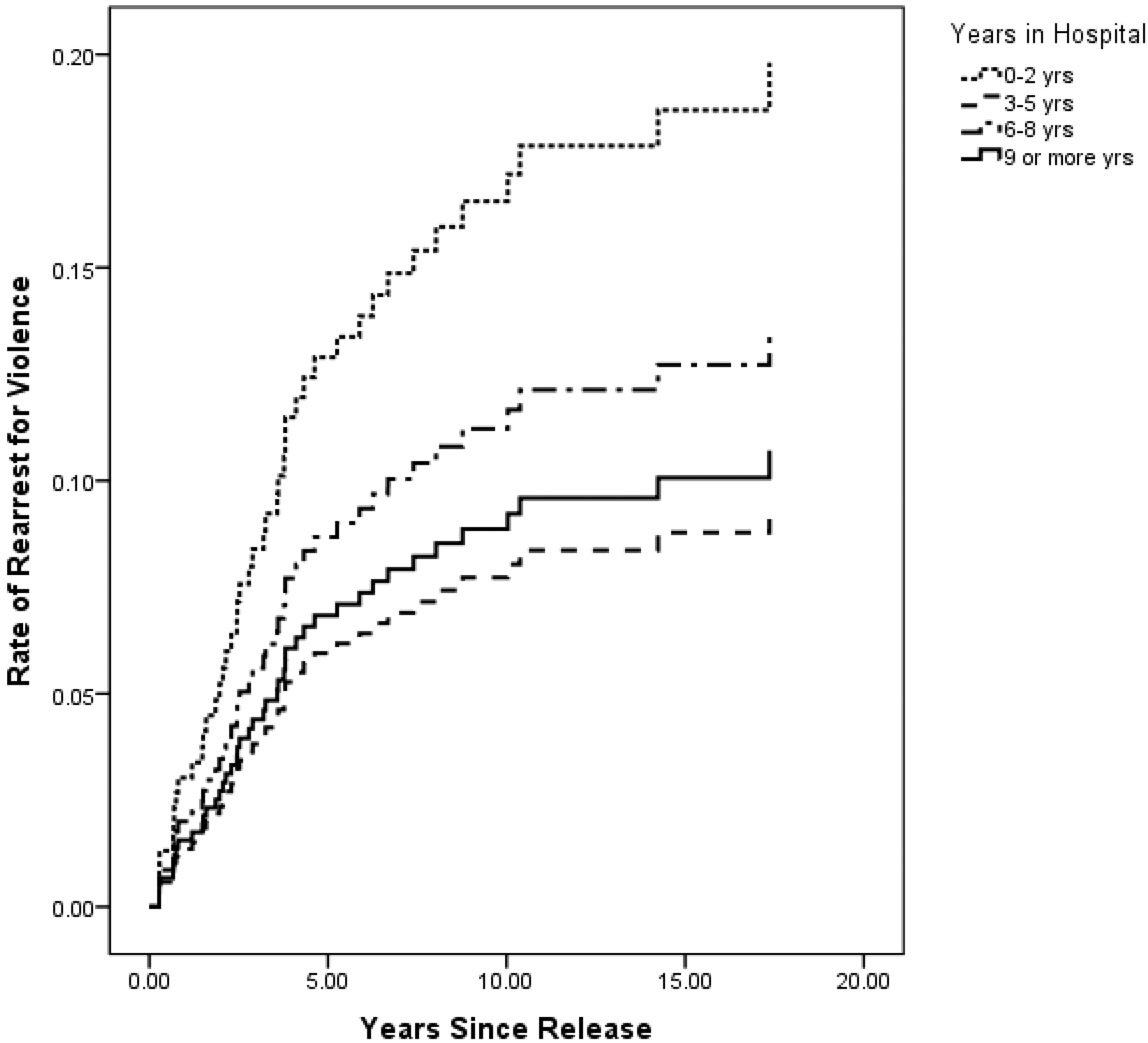
Estimate rate of re-arrest for violence by time in treatment (at means of covariates), males only.
Discussion
This analysis revealed a relatively modest risk of re-arrest among the NGRI discharges in New York State. Survival curves indicate that within two years of release, an estimated 2 percent of females and 14 percent of males are re-arrested. In contrast, a study of prison releases in 2002 in New York State revealed that 42 percent of females and 56 percent of males were re-arrested within two years of their release from prison.13 Moreover, the risk of re-arrest among NGRIs is largely limited to the first few years subsequent to release. Nearly one-half of the re-arrests are estimated to occur within the first two years of release and almost two-thirds occur by the fifth year. If NGRI releases have not been re-arrested by their 10th year in the community, their probability of re-arrest approaches zero.
While these low rates of re-arrest are notable, they do not address the question of whether hospital beds are utilized efficaciously or whether individuals could be released from the hospital earlier without increasing the risk to public safety. The regression analysis was designed to answer these questions by isolating the unique contribution of length of hospitalization to the outcome in terms of re-arrest. We found that length of hospitalization had a modest effect on re-arrest and no effect on re-arrest for violence. Moreover, the relationship between length of hospitalization and re-arrest lost significance when the date of release was added to the regression equation.
Characteristics that exerted the greatest influence on re-arrest among this mentally ill population were similar to those that predict re-arrest in the larger offender population (i.e., gender, age, antisocial diagnoses, and selective measures of prior arrests). These findings comport with prior research findings and speak to the importance of demographic and criminogenic factors in the prediction of arrest. Unfortunately, the factors are historical and static and, while predictive, provide little guidance for intervention. Although the positive relationship between the diagnosis of antisocial personality and re-arrest provides a more viable target for intervention, the interconnectedness of that diagnosis with historical criminal history measures and the absence of a physiological origin to the diagnosis has caused some to argue that it is largely a psychometric measure of criminal history. Still, the diagnosis provided more predictive power with regard to any re-arrest than did the criminal history measures.
Neither a history of psychosis nor one of substance abuse was predictive of re-arrest or re-arrest for violence within this population. The failure of a diagnosis of psychosis to predict re-arrest or re-arrest for violence was anticipated, particularly given that most subjects carried that diagnosis in their histories and that much of the prior research involving institutionalized populations has shown no relationship between psychosis and violence. Substance abuse, however, is widely recognized as a significant risk factor for violence among the mentally ill.5,14 The absence of a relationship between a diagnosis of substance abuse and recidivism in this population is noteworthy. Yet, substance abuse was nearly always a secondary diagnosis and, while the condition most likely aggravated the primary mental illness, its effect may have dissipated with treatment of the primary condition. Moreover, court orders of release routinely contain conditions that prohibit illicit drug and alcohol use and contain provisions for random monitoring to detect use. These conditions may contribute to the absence of a relationship between prior substance abuse and recidivism.
Overall, most predictor variables were more weakly correlated with re-arrest for violence than with general re-arrest. While the low base rate of re-arrest for violence limited the power of this research to discern these relationships, the rarity of violence across all lengths of hospitalization suggests that LOS is not critical to favorable outcomes as measured by re-arrest for violence.
The absence of re-arrest for violence among females is significant and, coupled with a low overall rate of arrest among females, suggests that this population may be particularly appropriate for shorter periods of hospitalization. Interestingly, females are often considered to be a more challenging patient population, despite their very positive outcomes in the community.
The limitations of this research caution against unbridled generalization to a broader population of patients. The period of discharge for this sample spans over 25 years, and treatment regimens changed significantly over that period. More recent releases were more likely exposed to cognitive-behavioral interventions and more effective medications. However, given that those released after the mid-1990s would have been more likely to have been exposed to these treatment advances and that they, as a group, also showed longer LOS, an effect associated with improved treatment probably resulted in an overestimate of the relationship of LOS and re-arrest, rather than the opposite. Indeed, that may partially account for the fact that LOS was unrelated to re-arrest once the date of release was added to the equation.
The period in which the discharge occurred also may have affected the rate of re-arrest through its relationship with level of community disorganization. Recidivism is the result of a complex interaction of individuals with their environments. Those released between the mid-1980s and -1990s were more likely to reenter relatively disorganized communities that were in the throes of a crack cocaine epidemic and record crime waves. Crime rates in New York City, for example, were twice as high in the late 1980s and early 1990s as in the late 1990s and beyond. Yet, to the extent that this figured into the results, it too would have increased, rather than reduced, the magnitude of the LOS effect. That is, the poorer outcomes among those who were hospitalized less than three years may have been partially due to their being disproportionately released during periods of significant community disorganization. This too would help explain why the addition of the release date variable to regression equation caused LOS to lose significance in the prediction equation.
The treatment of mental illness is an extraordinarily individualized endeavor. Had the length of hospitalization not been so heavily related to the date of release, one might hypothesize that it was associated with unmeasured factors that masked a greater treatment effect. For example, if longer periods of hospitalization were associated with treatment resistance or cognitive limitations and if those factors were, in turn, associated with recidivism, then controlling for such factors may have caused a stronger treatment effect to emerge. However, the LOS was highly related to the date of release and clearly influenced by exogenous legal considerations and administrative practices.
Despite the fact that the limitations of the research arguably should have resulted in an overestimation of the effect of LOS on recidivism rather than masking such an effect and that the addition of date of release to the regression equation did indeed reduce that relationship, additional research is needed before conclusions are drawn regarding optimal lengths of hospitalization. Ideally, research should include more temporally homogeneous samples and control for quality of treatment before and after release into the community. Thus, while this research raises questions concerning the value, in terms of criminal justice outcomes, of protracted hospitalization, it should not be interpreted as supportive of any general cap on the length of hospitalization. Instead, it should serve as a cautionary note that lengthy hospitalization does not necessarily equate to better outcomes. Similar findings have occurred in drug treatment research and may speak to the importance of affording patients the opportunity to utilize the skills developed through treatment or else risk their deterioration over time.15 Still, more research is needed to affirm the applicability of such findings to the forensic mental health system.
Footnotes
-
Disclosures of financial or other potential conflicts of interest: None.
- © 2011 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}
{kind=link}