


Abstract
There has been great debate concerning the existence and meaning of compensation neurosis. It is included in the International Classification of Diseases (ICD)-9 and -10 but not listed in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR). On the eve of publication of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), we re-examine the history and concept of compensation neurosis and conceptually update the condition to reflect current psychiatric thought. We consider its utility as a diagnostic entity for forensic evaluations and its components as they relate to exaggeration in injury claims. We also discuss how compensation neurosis differs from malingering and factitious disorder.
The use of the term compensation neurosis was more prevalent in the late 1800s to the mid-1900s than it is today, on the verge of the release of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).1,–,3 Highly revered historical medical figures such as Charcot have commented on aspects of the condition, claiming it was caused by “hysteria and neurasthenia”4,–,6 (Table 1). The more modern definition of the condition is seen in the 1946 quote from Foster Kennedy that “[C]ompensation neurosis is a state of mind, born out of fear, kept alive by avarice, stimulated by lawyers, and cured by a verdict” (Ref. 7, p 19). The concept was further defined in 1961 when Henry Miller, a neurologist, proposed a set of diagnostic criteria for accident neurosis that were initially accepted but were later challenged by the medical community1,2,8,–,12 (Table 2).
Various Names for the Concept of Compensation Neurosis That Have Been Used Over Time
The Miller criteria are frequently criticized as being unworkable by today's diagnostic standards, which are based more on operationally or functionally defined symptom criteria than on the interpretation of the patient's underlying conscious or unconscious mental motivations.13,14 Other criticisms are that the diagnosis does not have a predictive value, since many people who receive the diagnosis do not seem to improve or return to work after completion of litigation.14 These criticisms highlight the problems encountered when researching this condition, which include identifying the proper population for study; defining markers of improvement; evaluating for and controlling the vast number of confounding variables involved, such as the specific injury that occurred and the specific symptoms that developed; and subpopulations reporting different exacerbating factors.6,13,15 As noted by the anxiety researcher Mayou, “Few studies have been specifically designed to answer questions about the role of compensation, but there is consistent evidence that the processes of compensation and insurance benefits should be seen as among the many social influences on course and outcome” (Ref. 13, p 400).
The popularity of the diagnosis was also affected by new disease categories and diagnoses that have been introduced in the Diagnostic and Statistical Manual of Mental Disorders, Third Edition (DSM-III)16 and Fourth Edition (DSM-IV).17 Individuals who might have received a diagnosis of compensation neurosis in the past, in some cases now are erroneously subsumed into the categories of posttraumatic stress disorder (PTSD), postconcussive syndrome, adjustment disorders, pain disorder, and somatoform disorder. For example, Blanchard et al., looking for prognostic markers to identify individuals who would later receive a diagnosis of PTSD after a car accident, found the single greatest prognostic indicator to be whether a lawyer was contacted. As they noted, “[I]t is possible that those who have decided to seek litigation are subsequently inclined to portray themselves as more symptomatic…and thus more likely to meet the criteria for PTSD” (Ref. 18, p 8).
Thus, the field of psychiatry, particularly the field of forensic psychiatry, is left with the question of whether one of the historical explanations for the exaggeration of symptoms should be totally forgotten or should be maintained in some form as a valid diagnostic and real-world concept, even if unrecognized in the DSM-5. Should this diagnosis be reformulated and incorporated into a new diagnostic term that does not contain the ambiguity and stigma that plague the term compensation neurosis? As noted by Winckler, “Despite long-standing discussions, it still remains unclear whether ‘compensation neurosis' means a genuine psychiatric disorder or whether it merely stands for a person who claims unjustified demands after having suffered a traumatic situation” (Ref 19, p 219).
What Is Compensation Neurosis?
We propose that compensation neurosis is an exaggeration of symptoms that occur as a result of the unique stressor of seeking legally awarded compensation. It is brought about primarily by internal motivators coupled with a lesser degree of anticipation of secondary gain. Financial reward can clearly be a component in the condition and may influence the course, but the overall constellation of symptoms is due to more than just the pursuit of money.
Compensation neurosis is born out of many factors, such as unwarranted suggestions of illness and long-term injury (e.g., by lawyers, friends, family, and experts); the prolonged time and resultant stress incurred when seeking to have the claim heard; tendencies for stress to exacerbate somatization and underlying personality dynamics (dependent, avoidant, borderline, histrionic, and narcissistic disorders); rationalization; a need for justice, retaliation, or vindication; advantages of embracing the role of victim; or a sense of entitlement.1,4,6,9,–,12,15
Just as many psychiatric conditions can have various prognoses and rates of remission, so can compensation neurosis. Very rigid interpretation of the definition of compensation neurosis leads to the straw-man argument that the condition has no prognostic value because not everyone who receives the diagnosis improves after settlement.14 It is unlikely that just because a claim has been settled, all of the previously mentioned factors that influenced the development of the compensation neurosis would resolve (Table 3). As noted by Woodyard in his study of compensation neurosis:
It is, therefore, unfortunately not possible to estimate the total effect of settlement (since there are few unsettled controls), but clearly it does not guarantee loss of symptoms and return to work. However, review of general practitioner's records very often shows heavy [office] attendance that drops sharply soon after a final medicolegal report is given, presumably at the time of settlement, supporting the traditional belief that symptoms will improve once the legal case is out of the way [Ref. 15, p 193].
Improvement after settlement may occur for many reasons besides direct compensation. Once the case is over, the litigants have a sense of closure, stress and uncertainty are reduced, and they may now be in a position to move on with their lives. In addition, there is less stress in their lives regarding the uncertainty of the court case, the approaching deadlines, or the decision-making regarding the case. They are no longer directly involved in an adversarial system where their identity and reputation are under scrutiny and they have to prove that they are injured.
Reasons That Someone Correctly Diagnosed With Compensation Neurosis Would Not Return to a Comparable Level of Work or Appear to Improve After Injury
What Is Not Compensation Neurosis?
Compensation neurosis is not exaggeration, as described by the DSM-IV-TR's V code of malingering.17 Malingering is the overt and intentional gross misrepresentation of symptoms for secondary gain, defined as an external incentive, such as financial gain or avoidance of work.20,–,23 One of the unfortunate drawbacks to using the term compensation is that many automatically associate compensation with financial reward. Although there can be financial secondary gain as part of a compensation neurosis, the distinction is that the exaggeration occurs entirely, or at least primarily, for the external incentives in malingering and as a combination of external and internal incentives, with internal motivators being in equal or larger factor in compensation neurosis.
Compensation neurosis is not just the exaggeration commonly seen in individuals who engage in a form of reporting bias. Although reporting bias or misattribution can be part of compensation neurosis, the term bias, in general, does not indicate the potential motivational factors or stresses that lead to the exaggeration.24,–,26 The term merely describes how the exaggeration occurs, much as a cough explains a physical symptom but does not identify underlying pathology (e.g., virus versus lung cancer).
The ICD-9 categorizes compensation neurosis along with Ganser's syndrome as an example of a “factitious disorder with predominantly psychological signs and symptoms” (300.16).27 This categorization may not be accurate, according to the DSM-5. Although the newly proposed criteria for factitious disorder have components similar to those for compensation neurosis (e.g., the behavior is evident even in the absence of obvious external rewards), what separates the two is the notion of an identified deception. Although there is clear exaggeration with compensation neurosis, it is not necessarily the result of an intended deception.
ICD-10 includes compensation neurosis under Code F68.0: elaboration of physical symptoms for psychological reasons.9 It notes that motivation for the exaggeration of symptoms may involve financial reward, but includes other components (e.g., “dissatisfaction with the result of treatment or investigations or disappointment with the amount of personal attention received [from medical professionals]”; Ref. 9, p 222). However, the ICD-10 does assume the presence of a real illness: “Physical symptoms compatible with and originally due to a confirmed physical disorder, disease, or disability become exaggerated or prolonged due to the psychological state of the patient” (Ref. 9, p 222).
We contend that a compensation neurosis can occur in the context of psychosomatic symptoms brought on by the stress of seeking compensation and the societal expectations of illness, even if no real injury exists. Lees-Haley and Brown,28 in examining personal injury claimants with no history of brain injury, toxic exposure, or documented neuropsychological impairment, found that high rates of symptoms associated with these diagnoses were reported. The stress of litigation itself can lead to the onset of psychiatric and physical symptoms unrelated to any underlying physical cause.13,26,28,–,31
Who Contracts Compensation Neurosis?
Research on compensation neurosis has suggested patient types who are and are not prone to the condition. Individuals believed to be least likely to have the condition are generally young, well-motivated, and better-educated, with clearly identifiable illnesses or deficits (e.g., amputees) and without the tendency to engage in prolonged self pity.1,6,8,10,–,12,32 Individuals who were believed to be prone to the condition often have diagnoses of more ambiguous and subjective symptom-based injuries, such as soft tissue injury (e.g., back strain or whiplash), pain syndromes (e.g., causalgia, fibromyalgia, or reflex sympathetic dystrophy), and primary psychiatric injuries (PTSD, depression, or anxiety).6 In addition, those with only pain symptoms also frequently have a co-morbid psychiatric condition, with onset either before or after the injury, and frequently downplay or deny the existence of the preexisting psychiatric condition.6,10,11,15,32,33 People prone to the condition have characteristics of lower preinjury cognitive abilities, poor preinjury psychosocial functioning, low preexisting job satisfaction, hypochondriacal personality components, high suggestibility, tendency to assign blame for their difficulties to others, cluster B personality traits and defense mechanisms (e.g., entitlement, hysteria, or narcissism), and cluster C personality disorders (e.g., dependency).2,6,10,11,15,32,33
These characteristics at times are also found in populations of patients who malinger or have factitious disorder.
Why Does a Legal Setting Encourage Compensation Neurosis?
Unique to individuals seeking compensation is that they have to make and sustain a claim of injury and impairment in an adversarial system. Individuals in the compensation system, be it civil litigation or disability certification, may be interviewed and medically challenged many times, often over a period of years.8 They often experience, especially with disability claims, an initial rejection of their claim followed by a lengthy appeals process that leads to further anger, frustration, or need for validation and retribution and a sense of prolonged uncertainty and helplessness. In addition, even after being awarded disability, individuals may be concerned about losing their benefits because of future reviews, which becomes a sword of Damocles hanging over their heads. These factors result in conscious and unconscious pressure not to get better or progress in treatment, because improvement could diminish or eliminate compensation, create the impression that the claimant was not initially injured, raise questions about integrity, or disappoint people in the claimant's life, such as family members and lawyers, who are also highly invested in the disability claim.6,8,9,15
The prolonged adversarial process and frequent medical and legal evaluations also lead to the symptoms becoming magnified and recalcitrant in nature (a.k.a., symptom hardening) because the claimant must engage in multiple recountings of his medical story, with conscious or subconscious cues constantly being delivered by the people around him (lawyers, family, coworkers, and experts).8 In contrast, persons with clearly definable injuries, such as amputation, are less likely to have a secondary compensation neurosis because, no matter how much time passes or how many times they are asked about their injuries, their limb loss and physical limitations are evident. Thus, there is no pressure to hold firm to subjective complaints and exacerbate potential symptoms over time to be believed or recognized.
In addition, people with clearly defined illnesses are less likely to experience iatrogenic anxiety from exposure to medical experts. We have been involved in many cases of civil litigation in which most of the experts are in agreement, but one or two, usually those who use experimental techniques or procedures (e.g. functional magnetic resonance imaging (fMRI) or quantitative electroencephalogram (qEEG)) to diagnose and prognosticate regarding conditions such as mild traumatic brain injury, come to entirely different and dramatic conclusions (e.g., the injury is going to lead to an early death).34,–,37 We are not claiming that these techniques always lack validity or clinical utility, but in court cases, they can be applied in a misleading way that is not fully supported or accepted by the scientific community (e.g., generalizing smaller studies on selected research populations to a general population, using proprietary software to which only the expert has access, or using nonstandard ways of analyzing data, roughly analogous to over- or underexposing x-rays to obtain a desired result or an incidental or false-positive finding). For example, the American Academy of Neurology and the American Clinical Neurophysiology Society, in their report on digital EEG, qEEG, and EEG brain mapping, warned, “The use of these techniques to support one side or the other in court proceedings can readily result in confusion, abuse, and false impressions” (Ref. 35, p 284). This confusion and abuse creates legitimate concerns in litigants about their health and further increases their anxiety about whether they are being justly compensated. It also often makes them distrustful of other experts and clinicians who repudiate these findings, especially in the cases in which imaging or qEEG representations allegedly show pathology.
It may be hard for individuals seeking compensation to find high-quality or impartial clinical physicians. Many doctors intentionally do not treat individuals seeking compensation claims for a variety of reasons1 (Table 4). The result is that plaintiffs often end up being treated by doctors who actively seek to treat compensation clients or who are more sympathetic to individuals involved in the legal process.
Why Some Doctors Intentionally Avoid Getting Involved in Compensation Claims
In addition to being led by doctors of all types and training (e.g., MDs, DOs, chiropractors, psychologists, and doctors of nursing), claimants are also influenced by their lawyers. Lawyers often spend time talking with claimants about their symptoms and syndromes, defining exactly what the symptoms of a particular condition are, providing them with information about their condition and prognosis, and defining the important symptoms of their cases. Lawyers may refer claimants to clinicians and experts who they believe are likely to document the patient's symptoms in a positive and supportive way.38 Some of these clinicians and even experts have a potential stake in the outcome of the case because they have accepted a letter of protection (LOP) from the lawyer. The potential biasing effect of an LOP can be seen in this excerpt from a Florida Supreme Court opinion: “Respondent's office provided [the doctor] with a letter of protection, which contained a promise to pay him for [defendant's] treatment from [defendant's] recovery in the personal injury case…[and] was a common practice in respondent's law firm.”39 Although the American Academy of Psychiatry and the Law (AAPL) Ethics Guidelines clearly state that “[c]ontingency fees undermine honesty and efforts to attain objectivity and should not be accepted,” 40 not everyone involved in lawsuits belongs to the AAPL. Although LOPs are usually offered to clinicians, an additional ethics-related pitfall is encountered when the clinician's treating role becomes entwined with also serving as an expert witness. Although many forensic scholars such as Strasburg et al.41 and Reid42 have cautioned about serving as both expert witness and clinician, the practice becomes difficult to avoid, especially when the clinician initiates a treatment relationship, knowing that a lawsuit is occurring (e.g., records are likely to be subpoenaed and the clinician deposed, blurring the boundary between fact and expert witness) and that payment will be affected by the outcome.
Although not every lawyer or expert engages in practices that intentionally or unintentionally produce a compensation neurosis, such behavior occurs regularly and more often than is generally appreciated. For example, Essig et al.,43 in a survey of lawyers, found that it was common for them to spend at least one hour preparing clients for independent medical examinations by reviewing the symptoms of their illnesses, neuropsychiatric testing (e.g., likely tests to be administered, how tests work, and validity scales), and how malingering is detected in forensic evaluations.43 In a survey by Wetter and Corrigan,44 50 percent of lawyers believed it appropriate to provide clients with at least a moderate amount of information about the psychometric testing that they might undergo, and some thought it advisable to provide as much information as possible.
Even individuals such as Mayou, who question the validity of compensation neurosis as a diagnosis, recognize the unique iatrogenic potential for harm in the legal and disability arena. He commented:
In this context, it is important to emphasize that individual psychological reactions and other aspects of outcome are substantially determined by the reactions of other people, family, friends, employers and, not least, doctors. Iatrogenic factors can be of considerable significance…. There has also been a conspicuous increase in litigiousness and in the expectations of victims and of the wider public that those who are believed to have caused injury should both be punished and pay compensation…. It is possible, even probable, that changes in expectations have affected individual illness behavior as one of the many psychosocial determinants of the outcome of injury and illness [Ref. 13, pp 399–400].
Does Compensation Neurosis Fit in With Other Current Diagnostic Concepts?
The DSM-5 committee, at least in the field trial stage, has made the decision to “de-emphasize medically unexplained symptoms…and now focus on the extent to which such symptoms result in subjective distress, disturbance, diminished quality of life, and impaired role functioning.”45 Although this approach may work well for most clinical and research psychiatrists, it may be problematic for psychiatrists trying to provide objective forensic and disability evaluations, where the potential for malingering and symptom exaggeration is higher. Many researchers, especially those in the trauma-related field of anxiety, often champion the importance of unexplained subjective symptoms as being real and harmful to the patient if not recognized. They express the belief that malingering is a rare condition and that consideration of it distracts from the real suffering of individuals.13
Part of what hinders the discussion about symptom exaggeration and malingering is that there is no widely recognized base rate for known symptom exaggeration.28 The base rate can be influenced by many different factors, and studies therefore report the rate of exaggeration or malingering in compensation cases to be as low as 1 percent and as high as 70 percent.20,–,22,38,46 Mittenberg et al.47 attempted to determine the frequency of malingering and exaggeration by reviewing psychological test results from 33,531 cases submitted by members of the American Board of Clinical Neuropsychology. They reported that malingering or extreme symptom exaggeration was suspected in about 30 percent of personal injury cases (n = 6,371), 30 percent of disability claims (n = 6,388), 19 percent of criminal evaluations (n = 1,341), and 8 percent of clinical and medical cases (n = 22,131). These findings could indicate that both clinicians and forensic evaluators are rightly concerned that the frequency of malingering and extreme symptom exaggeration is or is not common in their respective fields. So, assuming a general base rate of about 30 percent for litigation evaluations, it makes sense to maintain the compensation neurosis construct as a possible explanation for symptom exaggeration in this context.20,–,22,46,47
The changing nomenclature in the DSM-5 shows a clear movement away from making “pejorative or stigmatizing” diagnoses, as noted by the renaming of the terms dementia (proposed change to major neurocognitive disorder) and conversion disorder (proposed change to functional neurological symptom disorder) and the possible removal of some personality disorders. (At the time that this article was submitted, DSM-5 was still being reformulated in the open-response stage).48,–,50 The removal and renaming of traditional terms could also lead to more bracket creep (a financial term used to describe how inflation causes individuals to enter a higher tax bracket without a real increase in buying power, but increasingly used in the medical community to describe more patients meeting criteria for a disorder because of overly inclusive changes in diagnostic criteria) or broadening of other diagnostic conditions, as some have warned is already occurring with PTSD.20,21,51,–,53
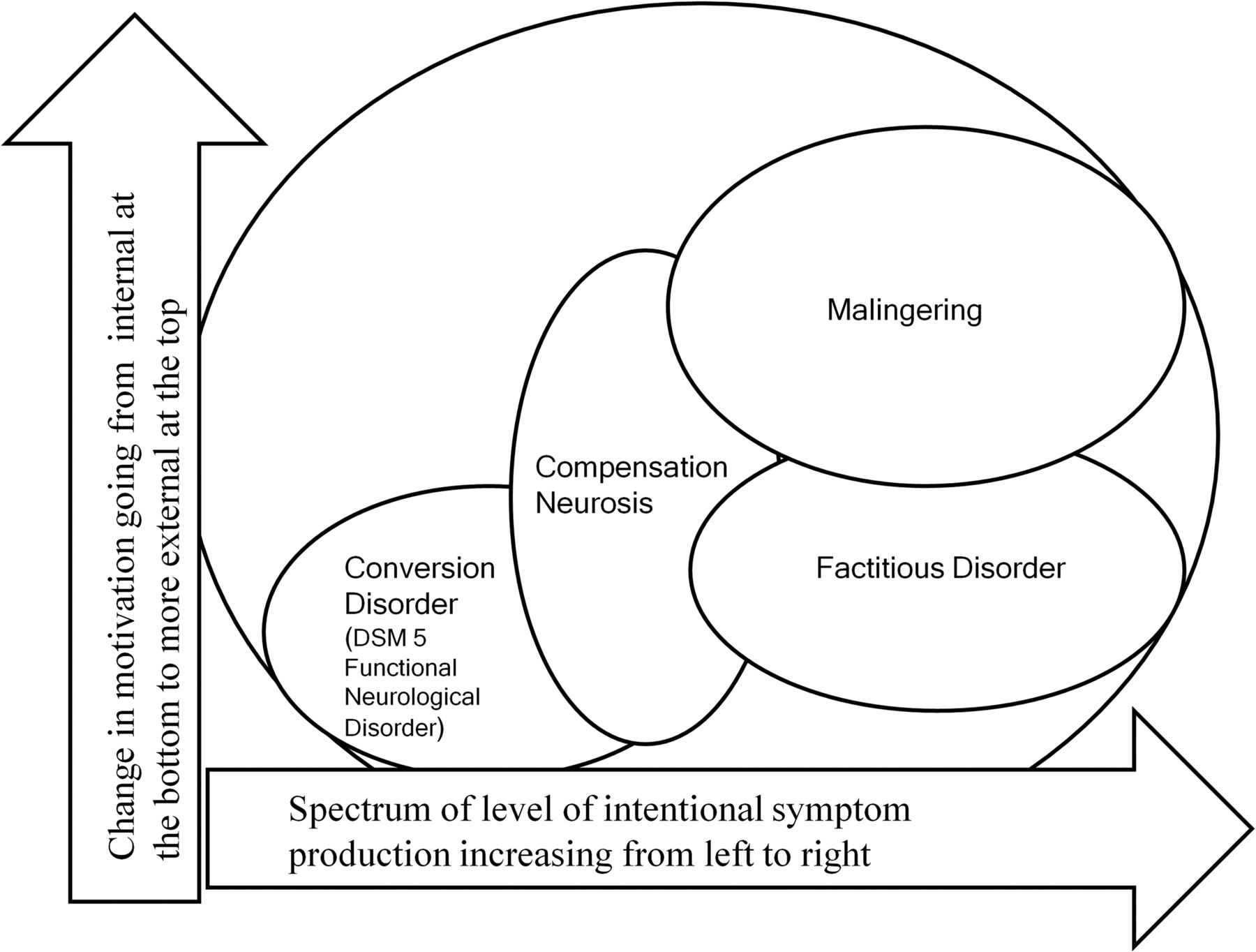
Just as many disease states are now being thought of as spectrum disorders (e.g., autism and Asperger's), conversion disorder, factitious disorder, compensation neurosis, and malingering could be thought of as occurring on a spectrum to explain exaggeration.8,11,15,30,54 (Fig. 1). Although the diagnosis of compensation neurosis would require the physician to determine the level of conscious and unconscious motivation, such a determination is currently frequently made in distinguishing conversion disorder from factitious disorder. The determination of conscious versus unconscious motivations in these cases is often made on the basis of the history obtained, commonly occurring presentations (e.g., la belle indifférence), inquiry into outside stressors, and a review of records. That physicians can have different opinions about whether a patient has a particular disease on a spectrum of disorders (e.g., conversion disorder versus factitious disorder) does not diminish the overall diagnostic construct of either condition. Often, variance in diagnostic opinion is due to the differences in information available, the differences in symptom presentation at the time of evaluation, the weight of significance applied to symptoms, and the degree of familiarity and experience that the evaluators have with the various conditions.

Conceptual understanding of how compensation neurosis fits into the spectrum of symptom exaggeration.
The perception that compensation neurosis is shaped by the expectations and beliefs of others without the presence of an underlying disease is similar to the DSM-IV-TR's diagnosis of shared psychotic disorder (297.3), also known as folie á deux, or the proposed DSM-5 condition of delusional disorder, shared type.55 In both cases, symptoms develop in individuals due to their consistently being exposed to a stressor. In folie á deux, this stressor is chronic delusions. In compensation neurosis, the stressor is the highlighting of impairments that reinforce the condition by frequent contact with lawyers, family, and experts. In both cases, the expectation is that once the stressor is removed, the symptoms will improve with time.
Diagnoses have been established for stress brought about by a particular event. The primary examples are bereavement, adjustment disorder, and PTSD. Just as it is true that not everyone who is exposed to a death or trauma will have these conditions, not everyone involved in a compensation claim will have compensation neurosis. That the condition is seen more frequently in people with preexisting psychiatric disorders or in those who have co-occurring personality features does not limit the usefulness of the diagnosis or the uniqueness of the condition. Similar predisposing features are noted in the other stress diagnoses, such as PTSD.20,21,31
Moreover, that the diagnosis may be used primarily by a specific subspecialty of psychiatry (e.g., forensic psychiatry) does not taint or limit it. There are many diagnoses that apply primarily to a single psychiatric specialty, such as child psychiatry, and that are based on only observable behavior thought to be due to internal, nonphysical causes, such as feeding disorder of early childhood (307.59), enuresis not due to a general medical condition (307.6), or separation anxiety disorder (309.21). In addition, forensic evaluators see a unique population under different conditions than do traditional clinicians, and so it is not unreasonable for there to be unique diagnostic categories for forensic examiners.
Conclusions
Whether there is a defined name for symptoms produced from the stress of an adversarial situation or not, such situations do occur, just as stress in other circumstances causes illness such as PTSD, bereavement, and adjustment disorder. Although there may be overlap and a varying spectrum of presentation between compensation neurosis, conversion disorder, factitious disorder, and malingering, it is important to recognize these conditions in their own right. The lack of flexibility in this area may lead to harm to patients, the legal system, and the credibility of forensic psychiatry, with individuals either receiving diagnoses of conditions that they do not have, such as adjustment disorder or PTSD, or being unfairly accused of blatant wrongdoing with a diagnosis of malingering. Although the DSM-5 appears to be moving away from looking at motivations for unusual symptoms, this change may result in a schism in psychiatry. The field of forensic psychiatry must address these concerns and needs diagnoses in the DSM-5 that will allow objective evaluations, even if it means using unflattering terms. Excluding appropriate diagnoses in the field of forensic psychiatry will only result in the decreased use of the current DSM in court and a potential explosion of idiosyncratic diagnoses (again, see Table 1) or references to the ICD system to fill the diagnostic void in the legal setting.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2012 American Academy of Psychiatry and the Law





{kind=link}