


Abstract
The veteran-forensic interface is an emerging area of relevance to forensic clinicians assessing or treating returning Iraq and Afghanistan war veterans facing criminal sanctions. Veterans' Treatment Court (VTC) represents a recent diversion mechanism for low-level offenses that is based on a collaborative justice model. Thirty-nine percent of veterans who served in Iraq or Afghanistan and receiving VA services reside in rural areas. Rural veterans facing criminal justice charges may be at a disadvantage due to limited access to forensic psychiatrists with relevant expertise in providing veterans services for diversion. Therefore, widening the pool of forensic clinicians who have such expertise, as well as knowledge of the signature wounds of the wars as related to aggression and reckless behavior is necessary. This article presents an overview of VTCs and discusses the role of forensic clinicians as stakeholders in this process.
In a recent article, Pinals1 highlighted the importance of forensic mental health professionals' knowledge of the veteran-forensic interface, indeed describing this as the next forensic frontier. Since October 2001, approximately 1.64 million U.S. service men and women have been deployed to engage in combat operations in support of Operation Enduring Freedom (OEF, Afghanistan) and Operation Iraqi Freedom (OIF, Iraq),2 frequently to war zones.1 Both the Afghanistan and Iraq wars have involved a large number of military reservists or National Guardsmen who have had multiple war zone deployments that have resulted in disruption to family and have caused financial hardship. Such stressors in addition to the trauma of combat for the returning veteran can be overwhelming and result in negative coping behaviors (such as alcoholism) and resultant difficulties with the law (e.g., domestic violence, driving under the influence, and reckless behavior). Clearly, a preferred strategy is to address returning combat veterans' psychological problems early, to circumvent negative outcomes. However, as the United States Department of Justice (DOJ)3 data suggest, there are many examples of veterans whose conditions were not checked who subsequently experienced substance abuse, unemployment, and involvement in the criminal justice system. These outcomes represent the high cost of military service for the men and women who serve in a theater of combat.4
In this emerging area a trend of relevance to forensic clinicians who are assessing or treating returning Iraq and Afghanistan war veterans facing criminal sanctions is the development of Veterans' Treatment Court (VTC). For specified low-level offenses, such courts allow diversion from incarceration to community probation and veteran-specific treatment interventions. Rural veterans facing criminal charges may be at a disadvantage because of limitations in access to Department of Veterans Affairs (VA) services. The Veterans Health Administration (VHA) provides health care services to approximately 7.8 million of the country's 23 million veterans. Forty-one percent (or 3.3 million) of the veterans enrolled in the VHA system reside in either rural or highly rural areas of the country. Within this group, 39 percent of those who served in Afghanistan and Iraq reside in rural areas.5 VHA's Office of Rural Health (ORH) was created in 2007 to improve access to and quality of care for the then 3.1 million veterans who constituted 38 percent (and in 2011, 41%) of veterans enrolled in the VA who resided in categories specifically defined as rural and highly rural areas of the country. The 2007 enrollment data identified 3,031,357 rural and 125,588 highly rural veteran enrollees.5
Rural veterans have been found to have poorer access to VA services and a higher intensity of mental health problems.6,–,8 In rural areas where clinical expertise and VA access may be more limited, the development of VTCs represents a unique opportunity for forensic psychiatrists and psychologists to assume a consultant role. This article highlights Veterans' Treatment Courts (VTCs) as a diversion option and a role for the forensic clinician that is likely to be of high value in rural settings.
Veterans' Treatment Court
The VTC represents a mechanism of diversion from incarceration to community-based treatment for veterans who become involved in the justice system. VTCs generally are a derivative of mental health and drug treatment courts.9 Moreover, they are a grassroots phenomenon emerging in jurisdictions that have an interested stakeholder, such as a judge, prosecutor, or public defender, who is often a veteran.4 There is wide variability across jurisdictions in several core characteristics of VTCs: some allow for violent felonies to be eligible, others do not; some require a nexus between military service and the crime; some are only for combat veterans; and others are for all veterans regardless of combat status, as the courts are treatment-based.9 All require the veteran to have a mental health problem, broadly defined to encompass substance abuse and other psychiatric conditions. VTCs utilize multiple community agencies as treatment resources, but with an emphasis upon Veterans Affairs (VA) to provide treatment, generally for the military service-related conditions connected to problematic behavior (e.g., PTSD, TBI, and drug and alcohol abuse).10 The VA health care system, a core and often mandated aspect of the treatment portion of veterans' courts, offers a wide range of services within the medical centers, such as residential care for dual or single conditions of substance abuse and PTSD, specialized care for TBI and broad medical and psychiatric outpatient services, in addition to programs designed to enhance work skills (such as compensated work therapy). Key advantages of VTCs are that the treatment services are paid for by the federal government (thereby freeing up local county resources for nonveteran defendants), and that a single provider (VA) covers the entire docket of veteran defendants.9 In addition, combat OIF/OEF veterans have priority status for care within the VA system, and Vet Centers offer free care for all combat veterans, regardless of their ability to pay for services.
Collaborative Justice Model
VTCs do not operate under a traditional adversarial model.9 Rather, they utilize a collaborative justice model in which all parties (prosecutor, defense counsel, probation, the veteran, veteran community mentors, and the VA) participate in a cooperative effort toward the veteran's rehabilitation.4 VTCs promote strong emphasis on veteran identity. These courts also utilize community veteran mentors as coaches to provide support for veterans to brainstorm, to achieve the mission of their rehabilitation and employment, and to establish or strengthen their ongoing familial and other interpersonal relationships.
As Figures 1 and 2 depict, with their emphasis on treatment rather than punitive solutions, VTCs stand to benefit both the veteran and society. The collaborative justice VTC model is in keeping with a movement away from using jails as institutions of mental health care. VTCs are similar to other mental health programs for diversion representing a burgeoning trend toward decriminalizing mental illness and provide a rich arena of expanded scope of practice for forensic clinicians, particularly in the underserved rural areas where many returning Afghanistan and Iraq veterans reside.
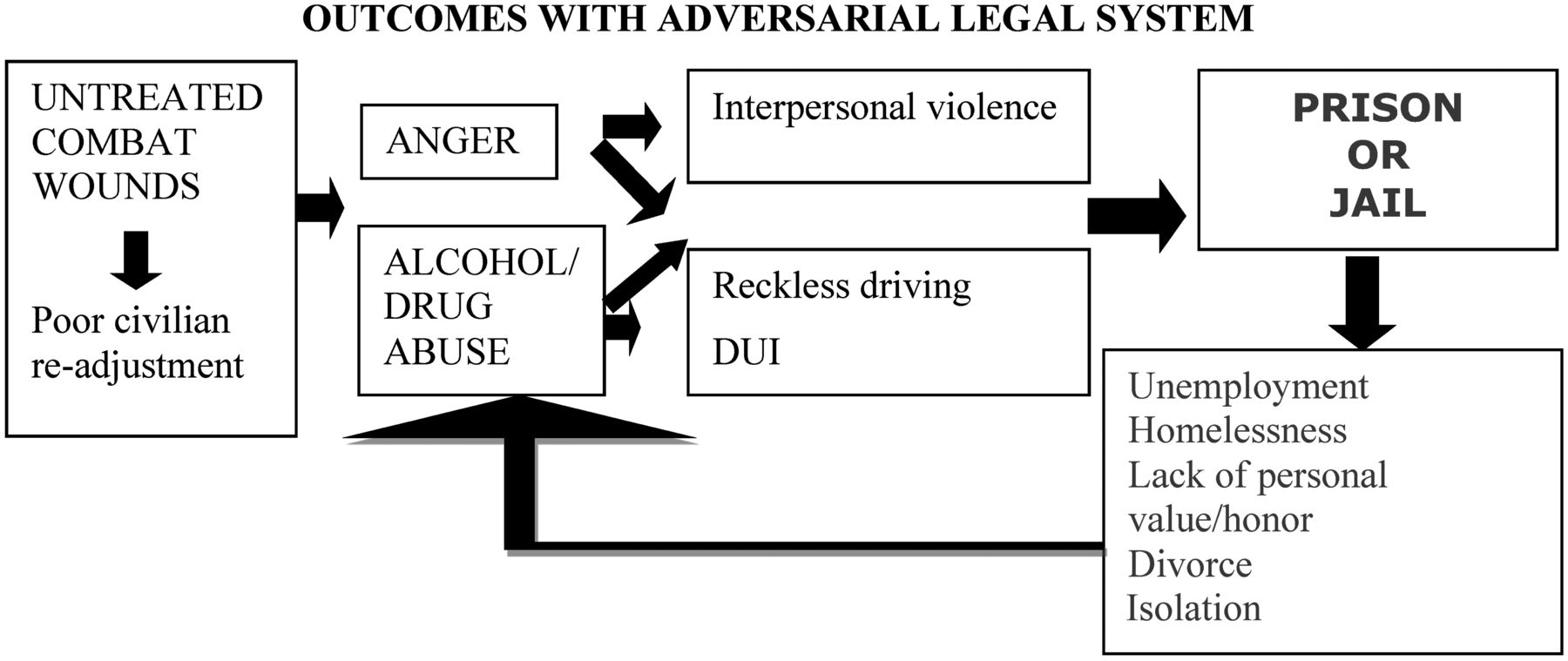
Outcomes with an adversarial legal system.
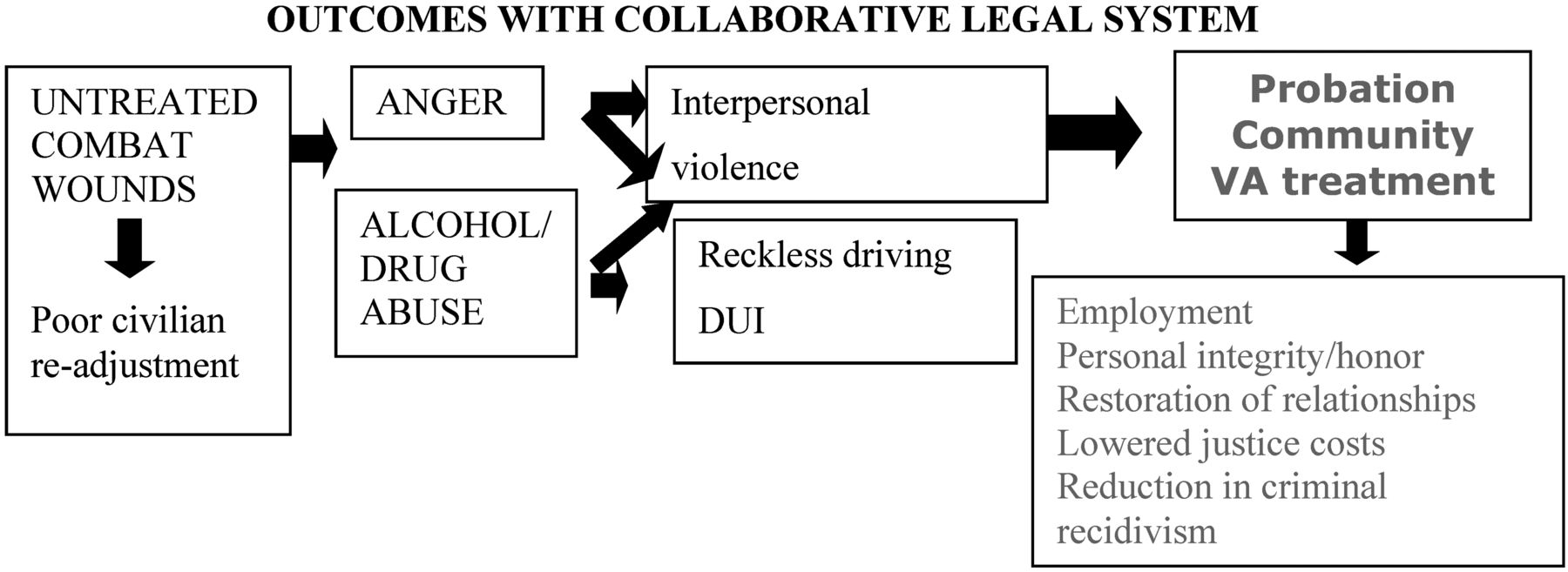
Outcomes with a collaborative legal system.
VTC Development
VTCs gained recognition and impetus with the establishment of the court in 2008 in Buffalo, New York.4 The VTC was in response to the increasing numbers of veterans appearing in court and the result of the effort of one interested judge.4 The National Association of Drug Court Professionals (NADCP)10 reports that there are (as of April 2012) 97 Veterans Courts and many more VTCs in various planning stages. The courts vary in legal status acceptance criteria. Some are preconviction diversion programs, while others accept only veterans who have pleaded guilty. Some hear only nonviolent cases, while others accept low-level violent offenses such as assaults without great bodily injury.4 With respect to veteran status criteria, some veteran courts confine participation to OIF/OEF (Operation Iraqi Freedom/Operation Enduring Freedom) veterans with combat-related PTSD, other mental illness, or brain injury.9,11
There are limited data on VTCs across the nation. A 2011 survey by Holbrook and Anderson12 of 53 existing veterans' courts in operation as of March 2011 reported data from just 14 courts that responded to a survey. They found that while the majority of courts heard misdemeanor and felony offenses, the felony offenses were less serious, excluding sexual assault and violent offenses involving serious bodily injury. Eligible offenses for veterans' court diversion included DUI, fleeing from the police, terroristic threats, and felony domestic assaults. As for qualifying for treatment, five courts mandated the presence of a treatable behavioral or substance abuse disorder for veteran court eligibility; others required a link between the mental condition and offense for veteran court involvement; and yet other courts accepted all veterans, excluding serious offenses, regardless of the nexus of the criminal behavior to a military- or nonmilitary-related mental health problem.
VTC and VJO
The primary method of the VTC's interaction with the VA is through the Veteran Justice Outreach (VJO) Program.9 By way of background, a complementary program that preceded the VJO is the HealthCare for Reentry Veterans (HCRV) program begun in 2006. It provides veterans in more than 1,000 state and federal prisons linkage to the VA and has to date reached more than 37,000 incarcerated veterans.9 Typically, VTCs work with VJO specialists who engage in important placement decisions.
Forensic psychiatrists and psychologists tend not to be involved in the VTC process. There are 172 VJO Specialists, the majority (95%) of whom are master's-level licensed social workers and a small number (5%) of whom are licensed psychologists. There are no VJO specialists who are psychiatrists. The role of the VJO specialist is that of a VA systems expert involved in determining the veteran's eligibility for VA services as well as facilitating admission into a court-approved VA treatment program. VTCs have as their focus criminal justice charges stemming from psychological or substance abuse problems viewed as linked to military service. Forensic psychiatrists and psychologists could provide an important role in acting as consultants to the VTC and as a liaison between the VA's VJO staff member, the court, and the veteran. A critical concern is the identification of clinical syndromes that the OEF/OIF veteran has, such as PTSD and traumatic brain injury (TBI), the nexus to criminal behavior, and how to provide adequate treatment so as to reduce criminal recidivism. These tasks fall squarely within the purview of forensic psychiatrists and psychologists. We suggest that the absence of forensic psychiatrists and psychologists represents a vacuum for needed diagnostic expertise and treatment recommendations to the court. Consulting psychiatrists and psychologists could provide forensic evaluations for the VTC that specifically delineate the treatment necessary for the OEF/OIF veteran and detailed guidelines for the veteran to follow. Such expertise provided to VTCs would serve to augment the veteran's successful transition to productive citizenship.
Rural Veterans
Knowledge of rural veterans' characteristics and needs is steadily expanding, with the following general findings reported in the Office of Rural Health (ORH) Strategic Plan for Fiscal Years 2012 through 2014:
We know that these Veterans are increasingly made up of soldiers returning from Operation Enduring Freedom and Operation Iraqi Freedom and that 15 percent of them have at least one service connected disability…. Prior studies indicate that Veterans who live in rural settings have greater health care needs than their urban counterparts. Specifically, rural Veterans have lower health-related quality-of-life scores and experience a higher prevalence of physical illness compared with urban Veterans. While prevalence of most mental health disorders is lower for rural compared with urban Veterans, rural Veterans with mental health disorders are sicker as measured by lower health-related quality-of-life compared with urban Veterans. These differences in health-related quality-of-life scores which equate to lower self-rated health status, among rural dwelling Veterans are substantial, clinically meaningful and associated with increased demand for health care services. Despite greater health care needs, rural Veterans are less likely to access health services for both physical and mental illness, either through VA or the private sector. In particular, rural Veterans have lower access to care for chronic conditions such as hypertension and posttraumatic stress disorder [Ref. 5, p 1].
Although it is not known what proportion of rural veterans have contact with or are involved in the justice system, the U.S. Department of Justice Bureau of Justice Statistics (BJS) has estimated that 9 percent of jail inmates, parolees, probationers, and Federal Bureau of Prisons inmates report that they are veterans and that 10 percent of state prison inmates also report having served in the U.S. military.3 Though not reflective of Afghanistan and Iraq war veterans, the BJS reports on veterans in prisons and jails, inclusive of data through 2002, may be instructive to trends that may emerge among the recent group of returning war veterans. BJS data indicate that justice-involved veterans have high rates of psychiatric illnesses (including mental disorders and substance abuse) and social problems (such as homelessness). While not conclusive, the intersection of a substantial number of rural veterans5 and the substantial illness and social burden faced by justice-involved veterans suggests a significant role for health care assessment and treatment for the rural justice-involved veteran population, without which research has found that community readjustment is frequently unsuccessful and reentry into the justice system a likely conclusion.
Rural Access Limitations
As most VA Medical Centers and clinics are located in urban or suburban areas, a lack of resource availability greatly inhibits the implementation of VTCs in rural counties.5 Veterans returning to rural counties who incur legal charges may not have the benefit of the VTC model and, because appropriate diversion options are not available, consequently experience sanctions, such as jail and prison, that have long-lasting negative implications for civilian readjustment.
A recent roundtable session representing eight VHA Veterans Justice Specialists identified several characteristics of rural justice outreach work, including, most prominently, distance barriers and access to VA services for the veterans seen in these courts (McGuire JM, Garrick T, Sreenivasan S, Rural Veterans Court: National VA Conference Call, May 2, 2012). The specialists concurred with each other on the following general themes:
In rural parts of states such as Alabama, Oregon, Michigan, Georgia, and Arkansas, distances ranging from 100 to 500 miles between court locations and VA Medical Centers are common.
Judges who want to assure that veterans get the services they need are faced with the complications of crossing state lines and jurisdictions.
Veteran populations in the courts are sometimes quite small, making identification of veterans a significant challenge. While many courts have a roughly equal population of current-era (e.g., OEF/OIF) versus prior-era veterans (Vietnam and post-Vietnam), there is no set pattern of age or war era representation.
Substance abuse services are the primary need, and navigating with courts to meet this need necessarily involves assistance from a range of VA clinical programs to get veterans to outpatient or residential treatment, including staff of Homeless Program Outreach, Housing and Urban Development (HUD) VA Section 8 Housing (VASH) programs, local VA community based clinics, and Veteran Service Organizations.
Secondary to services is the need for transportation to the service points, which can variably be arranged through subsidies for service-connected and low-income veterans (known as beneficiary travel in the VA), shuttles between outlying VA clinics and central medical center facilities, and VA-funded residential programs providing the transportation.
One recent innovative method of addressing rural access has been the implementation of the Web-Cam Court, as in Indianapolis and rural Oregon (Skinner P, personal communication, November 17, 2011). In the latter jurisdiction, the Klamath County Veteran's Treatment Court is located 85 miles from the VA Southern Oregon Rehabilitation Center where veterans receive residential care. Veterans are able to comply with court sessions through web-cam appearances. The veteran appears for court at the VA clinician's office where a web-cam on an office desktop (complying with VA TeleHealth and VA Firewall) connects to a VA staff person in court with a VA laptop. The veteran is able to inform the court about treatment status, goals, and plans. The VJO Oregon reported that there were 28 veterans in the Klamath County VTC, with 10 undergoing residential treatment at the remote site. The Web-Cam Court has afforded these veterans the ability to comply with court mandates and appearances without having to miss treatment. The VJO specialists' identification of the needs of justice-involved rural veterans underscores limited clinical resources available to this group. A tele-forensic model similar to the Web-Cam Court may be another method of addressing limited rural court access to forensic experts.
OIF and OEF Veterans in the Justice System
Noonan and Mumola3 reported Bureau of Justice (BJS) survey results for 2004, including that fewer than five percent of veterans in State (3.7%) or Federal Prisons (4.2%) reported service during the Afghanistan and Iraq War (2002–2004). Vietnam and post-Vietnam veterans represented most of the incarcerated veterans. The trends noted may be of value to understanding the potential questions that may arise among the next generation of war veterans from Iraq and Afghanistan. Noonan and Mumola3 found that, despite their generational differences, Vietnam-era and post-Cold War-era incarcerated veterans had similar rates of violent offense (61% and 57%, respectively), prior use of drugs (72% for both eras), and alcohol use (70% and 60%, respectively), although rates of mental health problems were slightly higher for post-Cold War veterans (56.7%) when compared with Vietnam veterans (47.9%), not a statistically significant difference. Estimates as to the numbers of OIF/OEF veterans currently in the justice system remain limited given that the last BJS data were collected either before the attacks of 9/11 (jail and prison survey) or three years after (prison survey). Recent preliminary data from the VJO indicates that in the period from April 2011 to April 2012, approximately 14,000 veterans were seen across the nation in prisons, jails, or courts by VJO specialists. Among these, approximately 3 to 4 percent of veterans in prison had served in Afghanistan and Iraq; approximately 15 percent seen in jails and courts had served in Afghanistan and Iraq.
Recidivism Rates From Current Veterans Courts
Veteran Treatment Courts are new, and therefore data are limited regarding rates of criminal recidivism. Early record examination of the Buffalo, New York Veterans' Court found a 0 percent rate of criminal recidivism one year into the program.4 Holbrook and Anderson12 found, across the 14 courts reviewed, that the total number of veteran participants in the programs was 465, with 59 graduates (8 had withdrawn, 21 were early terminations) with a one-year recidivism rate of under two percent (one case). Though follow-up is still at the preliminary stage (that is, only one year after graduation in a limited number of graduates), the low recidivism rates are promising.
Conclusions
For the returning combat veteran who has had exposure to events that take place only in war, transitioning back to a civilian life is not simple. Veterans returning home from a combat zone experience an array of postdeployment adjustments, and for returning Afghanistan and Iraq veterans that includes the derailing physical and mental impact of combat stress and traumatic brain injury. As a result, returning service members are at increased risk of engaging in unsafe behavior (such as reckless driving, heavy drinking and other risk taking) and to have a sense of invincibility.9 These tendencies if ignored can lead to negative consequences for the veteran both in the home and work setting; and, although these veterans are generally law abiding, their postdeployment behavior leads some to run afoul of the law and straight into the judicial system. Veterans' courts represent a mechanism for combat veterans who become involved in the justice system to engage with a system that is not punitive or adversarial but collaborative and that seeks to work toward a more effective resolution of problems. Moreover, these courts recognize the role of combat stress and related disorders in returning war veterans as a source of behavior that leads them to be in conflict with the law.
Forensic psychiatrists and psychologists to date have not had a prominent role in VTCs, but their specialized clinical expertise offers the potential to ensure the returning Afghanistan and Iraq war veterans' successful completion of diversion programs. Rural forensic clinicians with veteran-specific forensic expertise can bridge the gap in services to veterans (both treatment and assessment) through VA or court contracts with non-VA providers and potentially through broader use of web-cam technology. Therefore, it is necessary to widen the pool of forensic clinicians who have expertise related to veterans' justice diversion services and knowledge of the signature wounds of war as related to aggression and reckless behavior. This new frontier1 for forensic clinicians merits investigation, given the clear long-term benefits for the justice-involved veteran to be adjudicated through collaborative diversion as opposed to incarceration. Finally, engaging forensic psychiatrists and psychologists as stakeholders increases the likelihood of expanded rural VTCs for justice-involved Afghanistan and Iraq war veterans.
Acknowledgments
The authors acknowledge the dedication of VA staff who work with justice-involved veterans and thank the following for their input on serving justice-involved veterans in rural areas: Patricia Bradford, Gary Helle, Michael Matwyuk, Sonny Hatfield, Miranda Watkins, David Kagabitang, Brad Allison, and Paul Skinner.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2013 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}