


Abstract
This descriptive analysis is an examination of the extent to which a veteran's mental health diagnosis or the initial criminal charge committed before program enrollment relate to a greater propensity for sanctions, harsher sanctions, higher rates of relapse on substances, or overall program compliance. This is a retrospective descriptive analysis that focuses on those participants in the Harris County (Texas) Veterans' Court Program from June 2010 through April 2012 for whom the court had issued sanctions. The most clinically relevant association (p = .014) was found between veterans with substance use relapse and subsequent discharge from the program. Furthermore, the following four infractions were associated with a subsequent jail sanction: unexcused absence (p = .014), failure to complete a task (p = .010), substance use relapse (p = .001), and missing a hearing (p = .012). Given these findings, veterans with relapses in substance use during the course of the program are at greatest risk of noncompletion of the program and may represent a subpopulation of veterans who require greater or different types of assistance.
“In war, there are no unwounded soldiers,” wrote the poet José Narosky, whose aphorism could be no more apropos than when describing veterans with mental illness, such as those served by our nation's veterans' courts. Such courts offer the possibility of pretrial or postadjudication diversion for select veterans whose crimes and psychiatric histories fit within certain criteria. By so doing, these courts demonstrate an appreciation of the fact that soldiers traumatized by the horrors of war often face significant hurdles upon reacclimation to U.S. civilian life.1,–,3
Since the first veterans' court was established in Anchorage, Alaska, in 2004, and was first modeled for widespread dissemination in Buffalo, New York, in 2008, similar programs have spread to other jurisdictions, with over 300 courts in more than 35 states as of January 1, 2014. In 2009, Harris County, Texas, created the state's first veterans' court to serve the Houston metropolitan area.4 Like many of the veterans' courts that preceded it, this court provides an integrated treatment program, encompassing mental health care, substance abuse treatment, vocational rehabilitation, and veterans' benefits. It stands in contrast to specialty courts, which have historically hewn to a more limited ambit of drugs or mental health.
Veterans' courts were born of a need to improve service to veterans whose criminal activity was related to some form of mental illness. They share common elements with both mental health courts and drug courts. To date, they have been embraced by the National Association of Drug Court Professionals as a means of more appropriately addressing the needs of this challenging population.
For a veteran who has committed a criminal offense to be eligible for the diversion offered by a county veterans' court, the crime, as well as the veteran's mental health diagnosis, must fit within specified criteria. For example, veterans' courts commonly allow veterans with mental illness, substance use disorders, or traumatic brain injuries to participate. At the Harris County Veterans' Court Program (HCVCP), veterans must appear in court as frequently as twice a month, and substance users are regularly tested for drug abstinence. Compliance is often rewarded with gift cards, while those with either substance relapses or further encounters with law enforcement receive a variety of sanctions (e.g., verbal warnings, community service, increased frequency of court appearances, monitoring devices, or brief incarcerations). In addition, creative, therapeutic-based interventions, such as developing an action plan to avoid recurrent problematic behavior, are applied whenever possible. At the HCVCP, the treatment was almost exclusively VA based, with some community contracts for services not provided at the VA.
To date, no comprehensive assessment of veterans' court sanctions has been published. Furthermore, a search of the literature reveals a paucity of studies addressing veterans' courts. However, with regard to the mental health court (MHC) literature, sanctions have been deemed an “essential element” of MHCs,5 and participants charged with drug offenses have been shown to receive more frequent sanctions than those charged with other offenses.6 In addition, research on juvenile drug courts has demonstrated that court sanctions are associated with failure to graduate from the court program.7 Therefore, our research team hypothesized that, as a consequence, participants who are charged with substance use offenses would be more likely to incur court sanctions and less likely to complete the HCVCP. Thus, given both the dearth of formal, systematically constructed reviews of veterans' court sanctions and the substantial policy implications of this topic, we set out to determine whether there are associations between veterans' court sanctions and various other criteria, to challenge that hypothesis. In this descriptive analysis, we examine systematically the data obtained from the HCVCP with regard to the aforementioned associations. In so doing, we hope to gain a better understanding of which veterans are more likely to complete the court program.
Methods
This was a retrospective descriptive analysis that included those 53 participants in the HCVCP between June 2010 and April 2012 for whom the judge issued sanctions. Fifteen veterans enrolled in the HCVCP were excluded from our descriptive analysis because they were never sanctioned by the court.
Baylor Institutional Review Board approval to proceed was received on March 13, 2012. The court subsequently provided the deidentified HCVCP data, which included the following: age, sex, ethnicity, initial mental health diagnosis (if any), substance abuse diagnosis (if any), initial criminal charge resulting in referral to the HCVCP, date of sanction, type of sanction, date of infraction, type of infraction, and HCVCP treatment phase during which each sanction or infraction occurred. No names or initials, birth dates, social security numbers, addresses, or phone numbers were provided; thus, the descriptive analysis team had no way to identify, locate, or contact any of the participants in this retrospective review. Groupings of initial criminal charges, infractions, and sanctions were made based on their similarities, as our sample size was too small to permit a formal factor analysis.
Twenty-five initial criminal charges were merged into the following four groups: (1) assault (assault or bodily injury of a public servant, assault or bodily injury of a family member, aggravated assault with a deadly weapon, assault on a family member impeding breath, assault on a family member twice or more within 12 months, assault on a family member, aggravated assault on a family member, and deadly conduct); (2) burglary, forgery, or theft (attempted burglary of a habitation, burglary of a habitation, unauthorized use of a vehicle, evading arrest or detention with a vehicle, criminal mischief amounting to $1,500 to $20,000, theft of $1,500 to $20,000, burglary of a building, and forgery); (3) driving while intoxicated (DWI) (DWI 2nd; DWI 2nd, offender blood alcohol content (BAC) ≥0.08; DWI 3rd, offender BAC ≥0.08, and intoxicated assault with a vehicle resulting in serious bodily injury); (4) drug possession (possession of penalty group 1 controlled substances: <1 g, 1 to 4 g, and 4 to 200 g; possession of 1 to 4 g of a penalty group 2 controlled substance and possession of 5 to 50 pounds of marijuana).
Twenty-four infractions were merged into the following seven groups: (1) unexcused absence (unexcused absence from a court hearing); (2) failure to complete a task (failure to complete assigned homework, failure to provide required documentation, and failure to obtain approval before starting a new medication); (3) failure to complete treatment (late arrival to required treatment, failure to complete a halfway house or inpatient treatment program, failure to complete community service, failure to comply with a judge's order, having a treatment facility rules violation, and failure to enroll in required education); (4) substance use relapse (positive drug test, admission of drug use before failing a drug test, and admission of alcohol use before failing an alcohol test); (5) missed hearing (missed probation office visit, missed scheduled drug test, missed 12-step or support meeting, missed treatment without an excuse, absence from treatment facility with a warrant issued, and absence from the HCVCP but with voluntary return); (6) arrested (arrest for a new drug charge, arrest for a nonviolent misdemeanor or lesser offense); and (7) other (infractions classified as “other”).
Eighteen sanctions were merged into the following 11 groups: (1) verbal reprimand; (2) behavioral contract; (3) increased testing (imposition of testing, increase in testing frequency, electronic monitoring); (4) placement in a holding cell for duration of the docket; (5) written reports; (6) imposition of a 12-step program (imposition of or increase in 12-step or support meetings, with or without journaling); (7) loss of privileges; (8) community service (up to 8 hours or greater than 24 hours); (9) phase adjustments (starting the current phase over, adding weeks to the current phase, adding months to the current phase, returning to the previous phase); (10) jail (up to 10 days); and (11) discharge from the program.
In addition to analyzing the HCVCP veteran demographics, we evaluated for differences between the number of sanctions, infractions, and both mental health and substance use diagnoses grouped by ethnicity and initial criminal charge, by using analyses of variance (ANOVAs) for continuous variables and Kruskal-Wallis tests for categorical variables. The ANOVAs included the use of the Games-Howell multiple comparison procedure to account for differences between group sample sizes and within sample variance. Finally, we used the Pearson correlation between the sanctions, infractions, initial charges, ethnicity, and diagnoses to evaluate for associations between sanctions, between infractions, and between sanctions and infractions to examine for any potential common groupings between items.
Given the preliminary nature of these descriptive analyses, we chose not to use the conservative Bonferroni correction, but instead retained the α at 5 percent. SPSS version 15 for Windows was used for these analyses.
Results
Initial Criminal Charge
Significant associations were noted between participants with an initial criminal charge of burglary, forgery, or theft and those with psychotic disorders (p = .039) or a diagnosis of opiate, PCP, or benzodiazepine use (p = .039). Furthermore, during Phase 1 of the HCVCP, veterans with an initial criminal charge of drug possession committed a significantly greater number of infractions than those charged with either assault or burglary (p = .008).
Sanctions
The following four statistically significant associations were found in the 11 sanctions groups: (1) loss of privileges and subsequent discharge from the program (r = 0.353; p = .009); (2) written reports and verbal reprimand (r = 0.284; p = .039), written reports and increase in testing (r = 0.404; p = .003), written reports and placement in holding (r = 0.331; p = .016), written reports and jail (r = 0.289; p = .036); (3) verbal reprimand and community service (r = 0.516; p < .001), verbal reprimand and placement in holding (r = 0.284; p = .039); and (4) increased testing (drug or alcohol) and the imposition of a 12-step program (r = 0.645; p < .001), increased testing and phase adjustments (r = 0.436; p = .001), and imposition of a 12-step program and phase adjustments (r = 0.335, p = .014).
Diagnoses
The diagnosis of attention deficit hyperactivity disorder (ADHD) was associated with the imposition of a 12-step program (r = 0.353; p = .009), as was polysubstance use (indicating two or more nontobacco substance use disorders) (r = 0.353; p = .009). In addition, veterans who had a psychotic disorder were more likely to incur placement in a holding cell for the duration of docket (p < .001). Finally, an association was found (p = .009) between veterans with anxiety disorders and subsequently being required to consent to a behavioral contract.
Infractions and Sanctions
With regard to associations between infractions and sanctions, a significant association (p = .014) was found between veterans who committed the infraction of substance use relapse and a subsequent sanction of discharge from program. Furthermore, associations were noted between the following four infractions and a subsequent jail sanction: unexcused absence (p = .014), failure to complete a task (p = .010), substance use relapse (p = .001), and a missed hearing (p = .012).
Partial Correlations Between Infractions and Sanctions
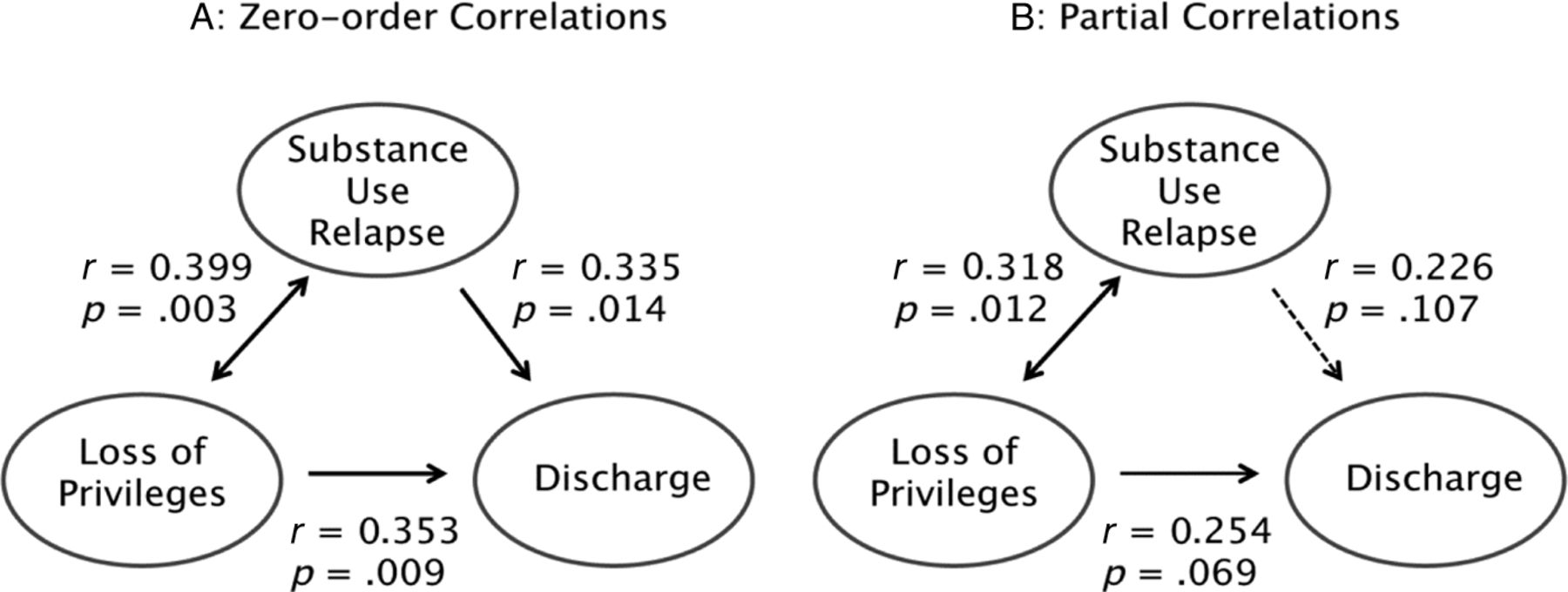
Given the close association between the infraction of a substance use relapse and the subsequent sanctions of loss of privileges and discharge from the program, as well as the consequences to both the veteran and society, we evaluated partial correlations between these three conditions to shed further light on their relationship. Figure 1 presents both the zero-order correlation and the partial correlation between each pair of variables while controlling for the third variable. The results indicate that a substance use relapse is significantly associated with the loss of privileges, which is itself associated with discharge from the program.
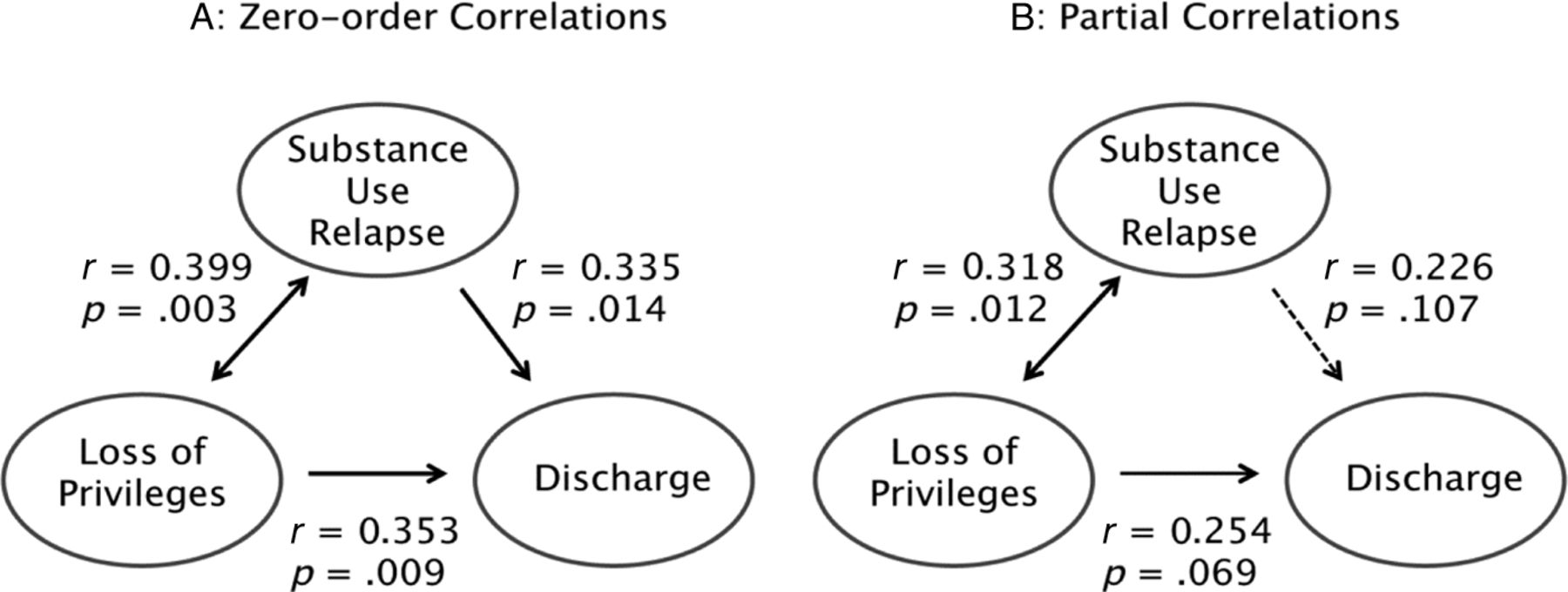
(A) Zero-order and (B) partial correlations between having a substance use relapse infraction, the loss-of-privilege sanction, and the discharge-from-program sanction.
Discussion
Perhaps the most notable result, even after evaluation for partial correlations, is the strong association between veterans who experienced a substance use relapse and subsequently incurred a loss of privileges, which ultimately resulted in a discharge from the program. Such an association suggests that it may be beneficial for various veterans' court programs to provide more support to veterans who have substance use relapses, to avoid an unfortunate and potentially avoidable discharge. Alternatively, these individuals may be better served by different treatment modalities or an entirely different venue. Examples of such enhanced support could include increased intensity of treatment and increased frequency of drug testing, as well as the use of other monitors of alcohol use. Given that unscheduled discharges may result in the accrual of additional administrative costs to the program due to extra clerical processing charges or court time, such outcomes may be worth avoiding. Alternatively, program administrators could judiciously choose to allocate limited resources to veterans with the greatest likelihood of completion.
As many substance-using veterans' court participants may be ineligible for traditional drug courts, owing to either their criminal history or comorbid mental health disorders, consideration should be given to the appropriateness of the available substance use treatment programs within the VA for severe and polysubstance use disorders. Alternatively, it may be possible to apply community resources to obtain the appropriate level of care for this challenging population. Future investigations should seek to improve understanding of which substance use diagnoses are most associated with program discharge.
An additional finding of significance was the association between veterans being jailed after an unexcused absence, failure to complete a task, substance use relapse, or a missed hearing. Given the considerable burdens on most county jail systems and the costs associated therewith, a reduction in both the frequency and duration of jail stays would be highly desirable from a taxpayer perspective. Furthermore, there are societal benefits to reducing individuals' exposure to jail when feasible from a public safety perspective. Earlier interventions by the program to avoid any of these four infractions would then cause savings to accrue to the program.
There was a notable association between the sanction of placement in a holding cell for the duration of the docket and a diagnosis of psychotic disorder. Brief incarceration is used as a sanction in both drug courts and mental health courts, though less frequently in the latter.6,8 The reduced use of jail sanctions in mental health courts may be due to differential public safety concerns between court type, based on the respective initial criminal charges accepted by each or the recognition that jail sanctions may be more effective in behavioral modification for drug use behavior than for psychosis-driven behavior. For mental health providers, the placement of a psychotic patient in a jail cell, albeit briefly, may raise ethics-related challenges and contradictory tensions between the desire to treat with the least restrictive means and the immediate need to maintain order in the courtroom. Considering the small number of defendants with a diagnosed psychotic disorder in our sample (four) and the lack of information regarding the specific behavior for which the sanction was applied at the time, it is not possible to speculate on the apparent association between this diagnosis and this particular sanction in the HCVCP. Future studies that include larger samples of program participants may help to clarify and validate this association. In addition, this population of psychotic patients may have unique vulnerabilities, such that future studies are warranted to help us improve our understanding of the effectiveness of brief jail holds as an intervention for persons with behavioral health relapses.
The most notable limitation of our descriptive analysis is the limited sample size of 53 veterans. Such is unavoidably the case for any veterans' court program that has been started within the past few years, as most have been. Thus, the door is open for future research once veterans have had a chance to pass through the veterans' court system in greater numbers. A further limitation of our research is that it does not provide outcome data regarding rates of recidivism, homelessness, or employment after graduation from the HCVCP. In addition, outcome data relating to mental health or substance use over time or to access to services for treatment are not available. Also, there are no data regarding long-term outcomes related to participation in a veterans' court or regarding whether other interventions beyond the court's involvement, such as exposure to VA services, were responsible for the success of the participants. Finally, with the use of a single court there is a limitation caused by the idiosyncrasies of a particular judge and how he may choose to impose sanctions within a specific court docket. With a new court program, there are modifications made in response to lessons learned. The experience of these initial participants, their successes and failures, may have led to alterations in how sanctions were meted out over time.
The HCVCP, similar to other such programs that are rapidly gaining popularity across the country, presents a unique opportunity to reach and serve the mental health and substance use needs of our returning veterans whose illnesses may or may not have contributed to their criminal justice involvement. However, there has been limited research on the process and outcomes of these courts. This article has presented the results of an initial investigation into the process of one such court and has identified a significant association between a substance use relapse, the subsequent loss of privileges, and ultimate discharge from the program. This finding shows that veterans in one particular veterans' court were less successful at remaining in the program and that the factors associated with success across veterans' courts should be better understood. Although no specific conclusions can be made on the basis of this association, it indicates that aggressive early treatment for drug-related infractions may be helpful in mitigating the risk of irregular discharge from the program.
Acknowledgments
We thank John M. Oldham, MD, for advice regarding the manuscript.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2015 American Academy of Psychiatry and the Law





{kind=link}