


Abstract
Patients' treatment records often contain information critical to risk assessment. We sought to determine whether psychiatrists treating outpatients agree about the standard of care (SOC) for requesting records from a patient's past clinicians. This web-based survey invited psychiatrists to review a hypothetical outpatient clinical vignette and to indicate whether they would request a release of information (ROI) from the patient for treatment records from past clinicians. Respondents also described the community SOC for similar scenarios and what they would do if a patient refused the ROI. Data were collected from June 15 through June 19, 2012. Most psychiatrists would try to obtain treatment records from any therapist, psychiatrist, or primary care physician seen by the patient within the past year. Some would require the patient's consent to ROI as a prerequisite to treatment. Few respondents felt that obtaining records from several years ago would be necessary in a typical, moderate-risk outpatient case. In an average outpatient scenario, the SOC would be to request treatment records from the past year. Psychiatrists rely heavily on clinical judgment when determining whether to obtain medical records from other providers.
A patient's records of prior mental health treatment often contain information of vital importance to the psychiatrist. Reviewing medical records is an important part of systematic risk assessment1 and can help to minimize the risk of errors arising from poor recall or inaccurate reporting by the patient.2 Treatment records may reveal a history of suicide attempts, substance abuse, civil commitment, hospitalizations, or violent behavior that the patient may not readily disclose to new clinicians. Charts from hospitalizations can also provide critical background regarding the patient's response to different treatment options, history of adverse events (such as medication allergies), and relevant medical and psychological histories.
Failing to consult a high-risk patient's records may increase the likelihood of an adverse outcome and subsequent lawsuit. As Tsao and Layde explained, “[f]ailure to obtain … important data precludes a psychiatrist's making a sound judgment based on those data” (Ref. 3, p 310). Common causes of lawsuits in psychiatry include failure to prevent patient suicide and failure to protect or warn third parties if a patient is at high risk for violent behavior.4 Risks may be identified, and adverse outcomes may be averted, if the psychiatrist thoroughly reviews records of prior treatment.
In Jablonski v. United States,5 the Ninth Circuit Court of Appeals upheld a wrongful death lawsuit against physicians whose patient murdered the plaintiff's mother. The doctors failed to review the patient's treatment records, which would have revealed a history of homicidal ideation and risk for future violent behavior. An expert witness for the plaintiff testified “that the failure to obtain Jablonski's records was negligent in light of accepted community standards” (Ref. 5, at 398), and the Ninth Circuit upheld a lower court's finding that the murder could have been prevented had the doctors obtained the medical records (Ref. 5, at 399).
Hindsight bias is a common problem in cases that result in an adverse outcome.6,–,8 In retrospect, it may seem that the psychiatrist should have requested the medical records, whereas in reality the decision not to obtain the records may have been consistent with the clinical judgment of other competent psychiatrists. Some patients (particularly those with a history of high-risk behaviors) may have extensive treatment records that few, if any, psychiatrists would have time to review in their entirety.
In medical malpractice litigation, plaintiffs' attorneys typically argue that the physician failed to conform to the accepted standard of care (SOC) for the profession and that this departure from the SOC constituted negligence resulting in harm to the patient or third parties.9 The SOC has been described as “the core of any malpractice case” (Ref. 10, p 664), and the use of the SOC concept in medical malpractice cases in the United States dates back to the mid-19th century11 and has analogs in English law.12 Although medical and behavioral health professionals often use the term standard of care in a clinical context, in the context of litigation the SOC is a legal term whose definition and interpretation is subject to change and revision over time. For general purposes, the SOC in medicine can be defined as “the caution that a reasonable person in similar circumstances would exercise in providing care to a patient” (Ref. 12, p e192). Reid notes that the SOC “is usually highly correlated with … what real doctors do across the country” (Ref. 13, p 172).
In some jurisdictions, courts apply what is called “the locality rule”: the SOC is defined through determining what is customary among professional peers in the local community. However, because of several factors, including the increasing standardization of medical practice across the country, most courts have opted to apply a national standard,14 and this trend appears to be increasing.10,15,16 Furthermore, the national SOC is more often applied than a local SOC for specialties14,17 such as psychiatry. Another trend in recent years has been for courts to explore what is reasonable practice, rather than to defer blindly to custom.18,–,20 Some states have passed laws in an attempt to define the SOC,19 but these definitions are typically vague and provide little guidance to the forensic expert who is asked to consult or testify in a malpractice case. In recent years, legal scholars have defined the SOC as “[t]hat which a minimally competent physician in the same field would do under similar circumstances” (Ref. 19, p 111).
When seeking to determine the SOC, courts often look to clinical practice guidelines (CPGs) promulgated by professional organizations,21 such as the American Psychiatric Association (APA). The APA's Practice Guidelines for the Psychiatric Evaluation of Adults indicate that it may be helpful to consult a patient's treatment records,2 but they do not provide specific, detailed guidance regarding which circumstances warrant such records requests or how many records should be obtained (or how far into the past) and from which treatment providers. This vagueness may leave psychiatrists and courts unsure of the SOC for records requests. Furthermore, clinical practice guidelines are often based on quality improvement initiatives and represent a clinical formulation, not the legal SOC, which represents a lower threshold of “minimal competence” (Ref. 10, p 665). The SOC plays an important role in cases that are settled without trial22 and in those that are resolved in a courtroom. In malpractice cases that go to trial, courts often require expert testimony regarding the SOC.15,23 Lewis and colleagues highlighted an important potential problem with expert testimony on the SOC:
In theory, the customary standard is based on empirical evidence, but expert witnesses are unlikely to know how other physicians practice. Instead, these expert witnesses are likely to base their testimony on what they would have done under the circumstances [Ref. 15, p 2633].
In a typical “battle of the experts,” “[h]and-picked testifying physician-experts give diametrically opposed views on what physicians usually do … based on nothing more than their accumulated professional experience” (Ref. 10, pp 663–4). This type of testimony is vulnerable to bias17 and may be especially vulnerable to Daubert24 challenges. Even in cases that do not proceed to trial, expert physicians (“outside reviewers”) are often asked by malpractice carriers to opine as to whether a physician charged with negligence conformed to the SOC.22 Thus, it is important for forensic experts to have a working knowledge of the SOC in their chosen specialty.
Very few published cases address the question of how one determines the appropriate SOC. Several scholars have called attention to evidence that most physicians simply do not know what is customary practice among their peers.10,14,15 There is little published research regarding the SOC in psychiatry25 and a dearth of published research or empirical data to inform determinations of SOC, even in other medical fields.10,14,26,27 Absent from this dialogue is the contribution of empirical data investigating what is, in fact, the standard practice among psychiatrists. There is some evidence supporting the use of physician surveys to help determine the SOC in certain types of cases.17,28 Therefore, we decided to survey psychiatrists about their opinions regarding the SOC for requesting records of prior treatment in a common outpatient treatment scenario.
Methods
A survey invitation was sent to psychiatrists in Rhode Island, then throughout the United States, through the Community Psychiatrists Listserv. The invitation contained a description of the survey and process for obtaining participants' informed consent; a hyperlink to a detailed disclosure of risks, privacy, and security practices for the study; the principal investigator's contact information; and a link to the survey, which was hosted at the website Survey Monkey. At the website, a welcome screen again described the survey and risks and protection of respondents. After having been advised of survey procedures, participants gave informed consent. This study was approved by the Institutional Review Board of Butler Hospital in Providence, Rhode Island.
Respondents provided basic demographic data: educational background, decade of residency completion, gender, state(s) of licensure, practice setting, certification or specialization, and nature and content of practice. We requested these data to help place participants' responses in context (i.e., was our sample skewed heavily toward a particular factor, such as having only hospital-based psychiatrists?) and to determine whether data were generalizable to a broader swath of psychiatrists in the United States, not to perform statistical analyses of differences in response patterns based on demographic variables. We did not collect information about age or ethnicity. After providing demographic data, respondents were asked to review the following hypothetical clinical vignette:
Mary is a 35-year-old manager who lives with her husband and two children. She is referred to you for an evaluation of depressed mood, and you develop a working diagnosis of major depressive disorder, moderate, recurrent. You decide to prescribe an SSRI.
This vignette was designed to represent an uncomplicated case without any red flags that indicate high or imminent risk.
Respondents were asked how likely they would be to request a release of information (ROI) for records of proper treatment from each of eight possible sources (Question 1; sources listed in Table 1). Participants were also asked what they believed would be the community SOC for requesting records in a similar scenario (Question 2). Responses were presented in a five-point Likert scale format: Never request, unlikely/rarely request, neutral/occasionally request, likely/usually request, or definitely/always request. Question 3 (“What do you think you would be likely to do if the patient refuses to authorize the ROI?”) and Question 4 (“How do you know the standard of care?”) were open ended; participants were invited to respond in their own words. Respondents could skip any items that they preferred not to answer.
Respondents Who Would Request Prior Treatment Records, and Perceived SOC
Data were collected from June 15 through 19, 2012. We performed only basic data analysis, using Microsoft Excel. We analyzed responses by determining the percentage of participants who responded each way. In reviewing participants' responses, we were interested in seeing whether psychiatrists agreed about the SOC for requesting treatment records for an outpatient with moderate depression. We also hoped responses might clarify how outpatient psychiatrists determine the SOC.
Results
Sample Characteristics
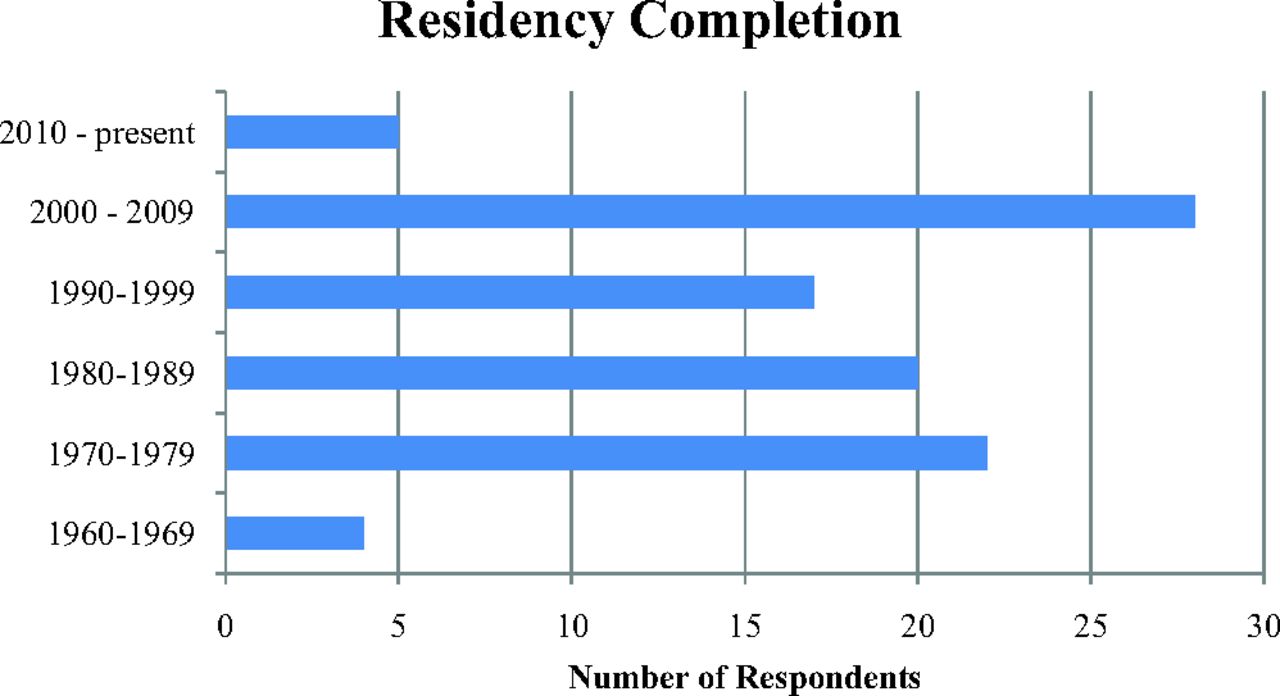
Ninety-eight psychiatrists (96 MDs and 2 DOs) responded to the survey. Figure 1 shows the distribution of respondents by decade of residency completion; 47 respondents were female. Physicians were licensed to practice in the following states: Rhode Island (53); Massachusetts (16); New York (11); California (5); Maryland (5); Connecticut (4); Washington (4); Ohio (3); Texas (3); 2 each from Illinois, Kansas, North Carolina, New Jersey, and Oregon; and 1 each from Alaska, Florida, Hawaii, Iowa, Kentucky, Louisiana, Maine, Missouri, New Hampshire, Pennsylvania, Vermont, and Wisconsin. Several respondents held licensure in more than one jurisdiction.

Distribution of respondents by training completion date.
Participants reported working in a wide variety of practice settings: hospital-based practice (43), community mental health centers (24), solo private practice (14), small group practices (8), academia (6), federally qualified health centers (2), private nonprofit organizations (2), assertive community treatment (1), and prison (1). Some respondents worked in several different practice settings. Participants held certification or specialized in the following additional fields: children and adolescents (10), geriatrics (9), addictions (6), forensic psychiatry (5), and psychosomatic medicine (2).
Seventy-five respondents practiced at least some outpatient medication management; 63 worked in teaching, education, or research; 52 provided outpatient psychotherapy; 39 did some hospital/inpatient work; 23 did consulting (e.g., for insurance companies); and 38 reported that their work involved additional “other” activities, such as management or committees. The sample was dominated by psychiatrists who see patients in outpatient practice.
Likelihood of Requesting Records and Perceived SOC
Table 1 illustrates respondents' likelihood of requesting records from different sources and their perception of the community SOC for such requests. Eight respondents identified other sources they would consult, such as the patient's family members, academic records, a statewide electronic healthrecord, psychometric testing results, other medical specialists, and records from a nonpsychiatric hospitalization.
Course of Action for ROI Refusal
Eighty-four psychiatrists described what they might do if a patient refused to authorize the ROI. Fourteen would refuse to continue treatment or refer the patient to a different provider, whereas the remaining 70 would in some way proceed with treatment. Responses offered by those who would proceed with treatment fell into one or more of the following categories: explore the refusal; attempt to persuade or explain; proceed if uncomplicated or proceed with caution; revisit the question later in treatment; document the refusal; or act according to unique case factors. Several responses were contingent (e.g., “Keep bringing it up. Might be unwilling to prescribe. Eventually might refer elsewhere.”).
Some respondents specified factors that would influence their likelihood of insisting on an ROI as a condition of continued treatment. Variables identified as important to this determination included duty to warn, patient's compliance with treatment expectations, history or likelihood of substance abuse, treatment setting (e.g., private practice versus public clinic), patient's diagnosis, severity or acuity of illness, patient's capacity or competency, care provision by another clinician, presence of suspicious factors in the patient's presentation, and psychosocial variables, such as involvement of family or significant others.
How Psychiatrists Learn the SOC
Seventy-eight participants responded when asked, “How do you know the SOC?” Each answer corresponded to at least one of the following categories: from colleagues or other providers (44.9%; n = 35), through experience or practice (35.9%; n = 28), “I don't know” or guessing (26.9%; n = 21), through training and education (14.1%; n = 11), from the literature or professional organizations (10.3%; n = 8), or through institutional policies (9.0%; n = 7). Answers categorized as “from colleagues or other providers” included discussion, observation, and experience in receiving record requests from other providers.
Discussion
The results of this survey suggest that outpatient psychiatrists rely heavily on clinical judgment when determining whether it would be appropriate to request medical records from prior treatment providers. As the data in Figure 1 and Table 1 demonstrate, respondents agreed that, for an uncomplicated case, the current practice is to try to obtain records from patient's therapist and psychiatrist seen within the past year, current primary care physician (PCP), and possibly the referring emergency room. Psychiatric hospitalization records from several years ago were deemed important but not essential. Few respondents felt that the standard would be to request records from a psychiatrist who had treated the patient more than 10 years ago. Thus, it seems that the current practice for the average outpatient would be to request records from any treatment providers seen within the past year, but not necessarily records from several years ago.
These findings support one respondent's observation: “I do not know if it is a standard or not … higher acuity care and more immediate is more relevant than older lower level of care.” Another respondent stated, “I practice in a teaching institution, and this is what I was taught and what colleagues and I teach. I believe wider community providers may not pursue records with the same frequency, and I believe care without requesting at least recent records is less than excellent care.” Many respondents noted that individual clinical factors influence their likelihood of requesting records from a prior treatment provider or requiring the patient's ROI as a condition of treatment. Such comments, coupled with the data obtained in our survey, provide at least some clarity, albeit not definitive, as to the likely SOC for requesting prior mental health treatment records in outpatient psychiatry.
Question 4 (“How do you know the SOC?”) raised some important concerns. It is noteworthy that 26.9 percent of those who responded to this question stated frankly that they do not know the SOC, are not sure how they know the SOC, or are just guessing. One participant stated, “I know no standard, just what I do.” Only 11 respondents mentioned training or education when asked how they know the SOC. Because a large proportion of our sample was within 10 years of residency completion (as shown in Table 1), this finding is surprising and suggests an important target for improvement in both residency and continuing medical education.
One respondent mentioned that ROI refusals occur “quite often” in his experience, as some patients in his practice (a crisis center) are angry with their previous clinicians. Such a situation presents the psychiatrist with a difficult ethics-related dilemma. Should one continue to treat the patient, hoping that over time a strong therapeutic alliance will persuade the patient to reconsider? Many respondents endorsed the use of informed consent to mitigate risk in such cases. The psychiatrist can describe the risks associated with lack of access to earlier records, such as an increased possibility of misdiagnosis and unintended adverse outcomes (such as allergic reactions to a medication), a potentially longer period for trial and error of different treatments, and even ignorance of warning signs of worsening symptoms noted by prior clinicians. The disclosure of risks and the patient's informed refusal to authorize the ROI can be documented in the chart. Simply refusing to provide treatment to a patient who refuses to authorize an ROI may be ethically problematic.
There are several weaknesses and limitations to the present study. First, the sample distribution was not uniform; Rhode Island, being the first author's home state, was overrepresented, and the results may not apply to all jurisdictions. In addition, the Community Psychiatrists Listserv provides a sample of convenience, and responses may not be representative of U.S. psychiatrists as a whole. Second, surveying physicians about practices they feel are reasonable is only one method of obtaining empirical evidence to help inform SOC determinations. This method is vulnerable to what Cramm and colleagues14 have described as idealization bias (i.e., physicians who responded to our survey may have overestimated the quality of care that they normally provide or that their colleagues provide). In reality, outpatient psychiatrists may not actually request or review as many treatment records as respondents to this survey believe. In some ways, observation and collection of data concerning actual practice patterns may yield superior evidence.10 Such studies have been conducted using standardized patients (i.e., actors),29 but there is evidence suggesting that the expense of such methodologies may outweigh their utility.30 As electronic medical records and clinical information sharing gain greater acceptance, the cost and difficulty of conducting practice-based empirical research is likely to decline, and future research studies will further clarify practice patterns to help inform SOC determinations.
To minimize the time and inconvenience to participants and thereby increase the response rate, we used a very short clinical vignette, and participants were able to skip questions they preferred not to answer. However, few respondents skipped any questions. Because of the brevity and hypothetical nature of the vignette, the participants' responses are not necessarily representative of the actual SOC in actual clinical practice. Outpatient psychiatrists typically have more information about the patient than the limited data provided in our vignette, and many respondents indicated that the SOC for requesting records varies on a case-by-case basis, depending on the patient's circumstances. One anonymous reviewer of our manuscript raised the question of whether prescribing a somatic intervention (in this case, an SSRI) predisposes to requesting records of past treatment; this leads to the question of how responses or practices might change if risk-related factors in the case were different. We suspect, but do not know for certain, that more extensive treatment records would be requested in a case with a high-risk presentation, such as past violent behavior.
We do not know whether people who are actually interested in identifying an SOC would be more or less likely to answer this survey request, so there may be a response bias of which we are not aware. Furthermore, by explicitly mentioning the term standard of care in some of the survey items, the survey may have primed respondents to consider the legal context and implications of their comments, possibly biasing their responses. However, given the candor among respondents who stated that they did not know the SOC, we believe that this survey has important implications for health care professionals and patients alike.
A final word of caution is warranted for the interpretation of our results. The SOC changes over time. As electronic medical records proliferate, it may become easier to obtain more extensive past treatment records for a patient. Furthermore, the process for reviewing records may change accordingly. For example, in electronic records, psychiatrists may conduct searches for specific words or phrases that indicate potential higher risks, and these searches may even be preprogrammed or automated at some point. It may become even easier than using the “CTRL+F” or “Find” functions built into common text-reviewing software. Searching for the phrase “suicide attempt” visually, when it is buried in a hand-written record (even a small one), can be a burdensome and time-consuming process when compared with using an electronic search tool for the phrase, even in voluminous records. These advances are likely to result in changes to the common practice among psychiatrists in requesting and reviewing prior treatment records. Readers should keep this in mind when interpreting our findings and realize that the corresponding SOC may change significantly in the coming years.
Conclusions
Surveys of physician peers can help to inform expert testimony about the SOC in medical malpractice cases, strengthening the evidence through empirical data,17 and can also inform clinical practice by providing clinicians with more information about what their colleagues believe is reasonable action. To our knowledge, this study is the first of its kind to survey outpatient psychiatrists about the SOC for requesting a patient's mental health treatment records. Our results suggest that, given respondents' understanding of the SOC, the current appropriate practice in outpatient psychiatry is to request an ROI for recent treatment providers, but not necessarily to condition treatment upon obtaining the ROI. Psychiatrists in our sample generally agreed that records ought to be requested from any psychiatrist, therapist, or PCP seen within the past year. The importance and relevance of past records decreased with the passage of time, such that records from a patient's distant past (i.e., 10 years ago) would not be essential in an average case. That several respondents specifically noted that their actions would depend on the specific factors in the case supports Simon's observation: “There is no stock answer to the question of what constitutes the standard of care. The courts apply reasonable standards to fact-specific cases” (Ref. 6, p 9).
We hope that our research findings will encourage dialogue and future research regarding the SOC in outpatient psychiatry. The study results should provide some clarification for outpatient clinicians as to what their colleagues would do in an average case.
Acknowledgments
The authors thank Miranda P. Icart for assistance in the collection of data for the study.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2015 American Academy of Psychiatry and the Law





{kind=link}