


Abstract
A rational algorithm for effective pharmacotherapy for impulsive aggression takes into account five factors: sufficiently defined and characterized aggressive behavior; availability of agents studied by trials of sufficient quality; risks, side effects, and contraindications; severity of aggressive outbursts; and co-occurring mental and medical conditions. Clinicians in forensic and correctional treatment centers, indeed in any treatment setting, should be able to optimize their effectiveness in treating impulsive aggression by using methods that consider these five factors.
Research supports the efficacious use of several drugs in pharmacotherapy for impulsive aggression,1 but no drug has been approved by the U.S. Federal Drug Administration (FDA) for this purpose. Despite numerous research reports and critical comparisons of the quality of anti-impulsive aggressive agent (AIAA) drug trials,2,3 the clinician is left with little guidance in how to go about selecting a drug for a particular patient with impulsive aggression. In a word, impulsive aggression is behavior that is angry or rageful, eruptive, unplanned, and lacking in self control, contrasted with premeditated aggression, which is planned, controlled, and unemotional.
There are earlier algorithms in the literature on pharmacotherapy for clinical aggression (e.g., Donovan and Aybar, 20034; Glancy and Knott, 20025,–,7; Mattes, 20128; and Moeller and Swann, 20079). Mattes8 supported the use of oxcarbazepine in particular. The system used by Donovan and Aybar4 was based on categorizing affective aggression as cognitively impulsive or paranoid and mood as mixed irritable or outer-directed irritable. The algorithms developed by Glancy and Knott6,7 and by Moeller and Swann9 were attempts to address more comprehensively the aggression caused by a wide variety of mental disorders. The focus of the present algorithm is limited to impulsive aggression, a common clinical concern. The proposed algorithm is based on a recent review of quality drug trials of anti-impulsive aggressive agents (AIAAs), to address efficacy of specific agents in the treatment of impulsive aggression in particular.2 It also takes into account recent changes in the diagnostic criteria of intermittent explosive disorder in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).10
Now that this edition of the DSM has expanded the criteria for intermittent explosive disorder (IED) to include a broader definition of impulsive aggression than did the criteria in the Fourth Edition-Text Revision,11 the volume of officially recognized patients with impulsive aggression amenable to pharmacotherapy is apt to increase. As explained below, this phenomenon has come about because the criteria for IED are now expanded to include aggressive outbursts that are of high frequency but low intensity (i.e., verbal, not necessarily physical, aggression). No doubt a mainstream consensus group will eventually develop an algorithm for selecting AIAAs in the treatment of impulsive aggression. Meanwhile, the algorithm that we present is offered as an approach that would ensure consideration of critical factors in selecting AIAAs for individual patients.
Five critical factors are involved in selecting an AIAA treatment of impulsive aggression in individual patients:
clearly defined and characterized aggressive behavior;
identification of drugs with efficacy demonstrated through drug trials of sufficient quality;
risks, side effects, and contraindications;
severity of the patient's aggressive outbursts; and
identification of any co-occurring mental or medical conditions.
For focus and brevity, this algorithm is limited to pharmacotherapy for impulsive aggression that is not secondary to a comorbid mental or medical disorder. For pharmacotherapy for secondary impulsive aggression, the reader is referred to a recent review by one of the authors.1
Much aggressive behavior can be reduced with nonpharmacological measures. Except for aggression due to severe mental illness or impulse, the structured environment of a correctional setting can be useful in maintaining order and reducing aggressive behavior.1 In inpatient or residential treatment settings, social learning and behavioral techniques can be useful, including the classic token therapeutic economy.12 Psychotherapy, including relaxation, cognitive therapies, and development of social and communication skills, can be applied to the treatment of clinical aggression, including impulsive aggression.13 Dialectic behavior therapy (DBT) can be of benefit, especially when self-directed or other impulsive aggression occurs in the context of borderline personality disorder.14 In cases where aggressive conduct is supported or provoked by the patient's social environment, adjustments of his surroundings can be useful.15 Where aggression is predominantly premeditated and not secondary to a major mental disorder, pharmacotherapy is not effective; thus, the best approaches would be nonpharmacological. Aggressive behavior, including impulsive aggression,16 has a psychological component for which psychotherapy can be useful regardless of whether pharmacotherapy is initiated. When aggression is severe and impulsive, pharmacotherapy is recommended. In the interest of space and focus, the present algorithm is limited to the pharmacotherapeutic approach.
A true algorithm is a decisional tree in which each decisional branch follows another, typically in a pattern of successive, dichotomous ramifications. For selection of an AIAA, two factors must be considered initially: definition and characterization of the aggressive behavior and identification of evidence-supported AIAAs. The remaining factors need not be considered in any particular order, but, although there has been some attempt to find the proper order for considering each factor, the decisional methodology offered here is not a rigid algorithm in the narrow sense.
Defining and Characterizing Aggressive Behavior
“Aggression is not aggression is not aggression,” the late Ernest Barratt would say when lecturing on impulsive aggression. He classified clinical aggression as premeditated, impulsive, or medically related,17 the latter being secondary to a psychiatric or neurological disorder. Felthous18 suggested a classification based on the degree of thought and emotion involved: 1) impulsive, 2) spontaneous, 3) compulsive, and 4) premeditated. In this article, the focus of concern is impulsive aggression with much emotion (rage) and little thought, which is increasingly recognized as a condition that can be improved by pharmacotherapy.17,19,–,21
A troublesome but common flaw in otherwise well-designed studies on drug efficacy in the treatment of aggressive behavior is the failure to define and characterize the type of aggression (impulsive or premeditated) that is being treated.22 Long a plague of such research, this error continues to be repeated in studies and study reviews.2
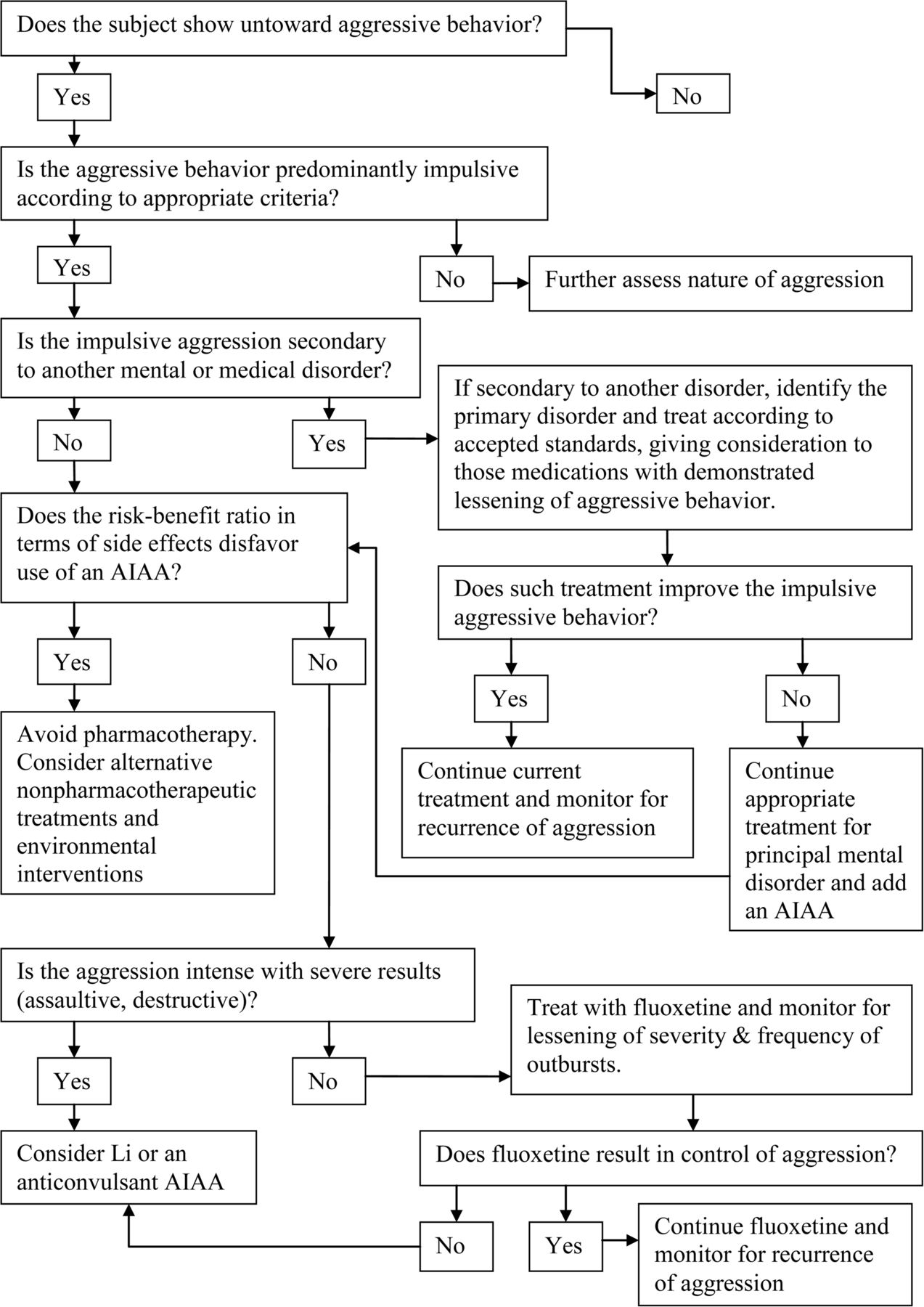
The first task in an algorithm for pharmacotherapy for impulsive aggression is to define and characterize the behavior (Fig. 1). Impulsive aggression is eruptive, unplanned, and shows a lack of self-control. Driven more by explosive emotion than by acquisitive or self-promoting goals, the impulsive outbursts of rage can be triggered by minor stimuli15 and can last a few minutes to several hours.23 Agitation crescendos until it is expressed in a violent act. During the state of extreme agitation, mental processing of information is deficient and meaningful communication is compromised.15

Algorithm for the pharmacotherapy of impulsive aggression. Beyond the factors embodied in the questions of the decisional algorithm, the clinician must consider the patient's medication history and the availability and affordability of the AIAA under consideration.
A more complete discussion of the nature of impulsive aggression, in many ways the mirror opposite of premeditated aggression, can be found elsewhere.15 A structured interview approach to the characterization of acts of impulsive aggression was developed by Stanford and Barratt24 and later modified to allow assessment on the basis of written records when the subject is unable to provide an accurate and reliable account of his violent episodes.25 The concept of impulsive aggression overlaps but is not identical with that of intermittent explosive disorder (IED).10,11 Trials of potential AIAAs have also used a modification of the DSM criteria for IED. The algorithm that we offer requires one of the following: initially and minimally defined impulsive aggression using criteria according to Barratt et al.,19–20 Felthous et al.,25 and Stanford and Barratt24 for characterizing impulsive aggressive acts; or the criteria for IED found in the third and later editions of the DSM10,11,26,27 or a reasonable modification of the IED criteria of the DSM, such as that applied by Coccaro.28,–,30
The DSM IV-TR11 criteria for IED excluded aggression that is better explained by the existence of another disorder, such as antisocial and borderline personality disorders. This now relative exclusion was carried over into DSM-5,10 even though it was dropped from Coccaro's31 research criteria for IED, which informed the changes in DSM-5.
Regardless of whether impulsive aggression is comorbid or secondary to a personality disorder, it is not treated in this algorithm as secondary aggression. If studies were discounted simply because of a co-occurring personality disorder, most of the high-quality drug trials demonstrating drug efficacy in the control of impulsive aggression would not inform development of this algorithm.
Nonetheless, this algorithm accepts impulsive aggression as defined and characterized by Barratt, as well as the IED or modified IED criteria used by Coccaro and colleagues: critical is that the aggression be impulsive, suitably defined. As will be discussed, the dichotomization of IED in DSM-5 into aggression that is of high frequency but low intensity versus low frequency but high intensity can also inform decisions on AIAA selection.
For pharmacotherapeutic decisions, the clinician must clearly distinguish whether the aggressive outbursts are mild or severe, frequent or infrequent. Also important is characterizing the impulsive nature of the aggression. Aggression against animals, for example, is not uncommon in the histories of forensic subjects who are antisocial,32 prison subjects who are aggressive toward people,33 or those who display disordered conduct that may be premeditated rather than impulsive.32,34 An aggressive act can be premeditated, compulsive, spontaneous,18 or even mixed, and is not invariably impulsive.
Once impulsive aggression has been identified, the clinician must determine whether the aggression is secondary to another mental or medical disorder, as the other disorder will dictate the first line of treatment. Regardless of whether the disorder is secondary, a further useful recognition is the presence of a co-occurring mental or medical disorder for which an FDA-approved AIAA is indicated.
Efficacy of Anti-impulsive Aggressive Agents as Evidenced by Drug Trials of Sufficient Quality
Several psychotropic agents have been used or recommended for the control of clinical aggression, but with variable, little, or no attempt to define the type of aggression being treated. We limited our interest to the treatment of impulsive aggression, adequately defined and characterized as discussed above. Next, we turned to those agents that have been studied and shown to be efficacious in reducing impulsive aggression.
A recent review examined the quality of 55 peer-reviewed studies on pharmacotherapy for aggression, regardless of study outcome2 and regardless of type of drug tested. Of those studies, only 23 met the quality criteria for inclusion in this analysis. The higher quality studies (n = 10; 45%) clearly defined impulsive aggression and satisfied most of the other quality measures, including measures of aggression, recruitment of subjects, study design, and outcome measures. Quality measures were weighted according to how strongly each was present, with the possible total scores ranging from 0 to 57. Among the 23 studies that were compared, the median and mode scores were 42. Higher quality studies were deemed to be those with a total quality score equal to or above this threshold.
The specific drugs evaluated in these higher quality studies included the anticonvulsants phenytoin, carbamazepine, valproate/divalproex, levetiracetam, and oxcarbazepine; the mood stabilizer lithium; the antipsychotic haloperidol; the antidepressant fluoxetine; and the amphetamines d-amphetamine and pindolol.2 Of these drugs, only levetiracetam had negative results and therefore lacks evidence of efficacy for impulsive aggression.35 Drugs with efficacy in treating impulsive aggression that was confirmed by more than one higher quality study included phenytoin,19,35,36 carbamazepine/oxcarbazepine,37,–,39 valproate/divalproate,37,40,41 lithium,42,–,44 and fluoxetine.28,30,45 Some evidence supports positive effects of sertraline46,47 and other selective serotonin reuptake inhibitors (SSRIs)48,49 in diminishing impulsive aggression, but most of the adequately controlled drug trials on SSRIs have evaluated fluoxetine.2 Thus, despite fluoxetine's increased risk of medication interactions via p450, only those AIAAs, including only those SSRIs adequately supported by research of sufficient quality (specifically among the SSRIs, fluoxetine) are included in this evidence-based algorithm.
If there is concern about drug-drug interaction via p450 and the patient is averse to the blood testing necessary for lithium and anticonvulsant AIAAs, sertraline could be a reasonable selection, but with the realization that the medical evidence of its efficacy is less robust than that for fluoxetine. Two of the three studies that supported lithium42,43 and one of the three studies that supported carbamazepine/oxcarbazepine38 involved children as subjects. All other replication studies enrolled adults. Although some high-quality studies included both male and female subjects and others only male subjects, none involved only female subjects. Thus, the possibility of a differential response based on gender has not been adequately studied.
Jones and colleagues3 conducted a meta-analysis to assess evidence of the efficacy of mood stabilizers in reducing repetitive or impulsive aggression. Their review, which included quality measures, supported efficacy of carbamazepine/oxcarbazepine, phenytoin, and lithium, but not levetiracetam and valproate. Comai and colleagues50 recently published a translational approach to pharmacology for aggressive behavior that provides a summary of possible neuroendocrine mechanisms of action for AIAAs. Goedhard and colleagues51 presented a review of the quality of drug trials in the treatment of clinical aggression, but without distinguishing types of aggression (e.g., impulsive) or the psychopathological context.
Based on these reviews of quality and efficacy, this algorithm for the treatment of impulsive aggression is limited to phenytoin, carbamazepine/oxcarbazepine, valproate/divalproex, lithium, and fluoxetine.
Risks, Side Effects, and Contraindications of AIAAs
Important in a comprehensive algorithm on pharmacotherapy for impulsive aggression would be reasons not to select particular agents or classes of AIAAs. Consideration of risks, side effects, and contraindications is especially critical when prescribing AIAAs, because none of these agents is FDA approved for the treatment of impulsive aggression or IED. These are topics for which information is available, however, and with which clinical psychiatrists should already be familiar.
To summarize, some primary considerations for avoiding AIAAs or using them only with extra circumspection:
pregnancy, as all AIAAs present some risk to fetal development, especially in the first trimester52,–,60;
other conditions and population groups with elevated risks with specific AIAAs (e.g., for carbamazepine the risk of epidermal necrosis and Stevens-Johnson syndrome in patients of Asian ancestry);61
use of lithium in patients with cardiac pathology,62,–,64 renal disease,62,65 diabetes insipidus,66 or thyroid disease67,68 and in elderly patients;69 and
use of divalproex in patients with impaired liver function.70,71
Other risks of divalproex include pancreatitis and polycystic ovaries.72 As in prescribing any medication for any condition, the clinician must weigh the risks and benefits.
Of the AIAAs, fluoxetine has the most favorable side-effect profile, but one must bear in mind the risk of drug–drug interactions via the p450 system for fluoxetine in particular. Aside from fluoxetine, valproate/divalproex has a more favorable side-effect profile than lithium, other anticonvulsant AIAAs, and antipsychotics.70,73 One must always consider the risk of drug–drug interactions. For example, carbamazepine and phenytoin can decrease the efficacy of oral contraception,74 and therefore fluoxetine or valproate should be favored for women taking contraceptive medications, or they should be advised to consider alternative means of contraception.
Severity of Aggressive Outbursts
DSM-5 retained intermittent explosive disorder as a diagnosis.10 Although today's research evidence for the efficacy of AIAAs is not based on the DSM-5 criteria, just published in 2013, clinicians in the future will use the current DSM to diagnose IED and therefore impulsive aggression. One difference in the DSM-5 criteria for IED from those in previous editions, which may prove useful in this algorithm for selecting AIAA agents, is its dichotomization of IED into mild and severe types. Applying the polythetic diagnostic approach that began with the Third Edition of DSM,75 the clinician can now diagnose IED if the aggressive acts are frequent but not necessarily severe or intense or if they are severe and intense, but not necessarily frequent. The new inclusion of impulsive aggression, wherein aggressive outbursts are of high frequency but low intensity in terms of destructive results, is supported by research and argument of Coccaro31 in particular and will cast the diagnostic and therapeutic net for IED more broadly. Although Coccaro argues that there are common features in both forms of aggression and that they represent different manifestations of the same disorder, there may be therapeutic value in considering high-frequency/low-intensity and low-frequency/high-intensity outbursts to represent subsets of IED or impulsive aggression.
The mild form of IED in DSM-510 would be manifested first by verbal aggression (e.g., temper tantrums, tirades, or arguments) or physical aggression toward property, animals, or other individuals, occurring twice a week on average, for a period of three months. The physical aggression does not result in damage or destruction of property and does not result in physical injury to animals or other individuals (Ref. 10, p 466).
This less severe expression of aggression corresponds to the aggressive conduct investigated by Coccaro's group,28,30 which showed a favorable response to fluoxetine. Thus, fluoxetine can be considered a first-line AIAA for this milder form of impulsive aggression, which can be verbal or physical. If fluoxetine is ineffective or the aggressive acts are sufficiently severe as to require a more aggressive approach, trial of an anticonvulsant AIAA or lithium may be warranted.
Unless the aggression requires management because of the seriousness of its result, such as assaultive and physically destructive behavior, the first-line AAIA would be fluoxetine28,30 because of its favorable side-effect profile and convenience of administration. Unlike the anticonvulsant AIAAs and lithium, use of fluoxetine does not necessitate regular blood tests.1,28 As with the prescription of any AIAA, a baseline chronology of impulsive behavior should be documented before initiating fluoxetine, and the frequency and severity of outbursts should continue to be monitored to titrate to an effective dose and to ensure medication responsiveness.
In the second type of aggressive behavior, which can also qualify as IED, the poor control over impulses is manifested by three behavioral outbursts involving damage or destruction of property and physical injury of animals or humans occurring within a 12-month period (Ref. 10, p 466).
This type of aggression, more severe in its harmful results, corresponds with that studied by Barratt and colleagues,19,20 which improved with phenytoin. For such serious and dangerous aggression, the clinician may turn directly to a specific anticonvulsant AIAA or lithium, rather than to an initial trial of fluoxetine.
Co-occurring Conditions
Mental Disorders
Treatment of the principal disorder can reduce aggressive behavior that is secondary to the condition. Sometimes the very medicine used to treat the principal disorder happens to be an effective AIAA: a mood stabilizer for bipolar disorder, for example. In that case, the AIAA is FDA approved for the principal disorder and control of impulsive aggression is a secondary, but useful, benefit. Even with insufficient symptoms to diagnose another disorder, a few symptoms of another disorder can help to inform the selection of an AIAA. Signs of depression would favor selection of fluoxetine. Increased affective drive or lability of mood and affect would favor a mood stabilizer, specifically a mood-stabilizing AIAA.
Seizure Disorder
Seizure disorders commonly co-occur with mental disorders and impulsive aggression. If the patient exhibits impulsive aggression as well as a seizure disorder, thought should be given to an anticonvulsive AIAA that could effectively control both disorders. This principle of parsimony in pharmacotherapy would disfavor the use of lithium, because lithium is not an anticonvulsant. It would also disfavor the use of levetiracetam for seizure control, because levetiracetam has not been demonstrated to control impulsive aggression.35 The parsimony principle limits the choice of AIAAs to those that are also effective anticonvulsants: phenytoin, carbamazepine/oxcarbazepine, and valproate/divalproex. Of course, some seizures are only controlled with the use of other non-AIAAs, but if both conditions can be controlled with a single drug, then the question becomes which of these AIAAs warrants selection over the others. Phenytoin may be favored if the aggression is serious and the need for control is urgent (see below), whereas carbamazepine/oxcarbazepine and valproate/divalproex may be the better choice for symptoms of emotional dysregulation. Once the selection of AIAA is narrowed to carbamazepine/oxcarbazepine versus valproate/divalproex, the ultimate selection will rest on the pharmacotherapeutic history of improvement, side effects, and any risks of side effects that are peculiar to the patient.
Unless known pharmacotherapeutic history or risk of certain side effects dictates otherwise, two considerations are the presence of a mood disorder for which a mood stabilizer is indicated and urgency of the need for a therapeutic response. If impulsive aggression co-occurs with a disorder on the bipolar spectrum, ranging from bipolar I disorder where the mood disorder is most severe and the medication for a mood stabilizer is most compelling, to the emotional instability of borderline personality disorder, for which the value of pharmacotherapy is not as strongly supported by research, consideration can be given to an anticonvulsant AIAA that is also an efficacious mood stabilizer: carbamazepine/oxcarbazepine or valproate/divalproex, but not phenytoin. This consideration lies more clearly in the algorithmic branch that deals with impulsive aggression secondary to another disorder; but the causal connection with a bipolar-type mood disorder is not always clear, and impulsive aggression can co-exist independent of any other mental disorder.
Because mood stabilizing medications are familiar and commonly used in clinical psychiatry, phenytoin, the AIAA with the most high-quality studies supporting its efficacy,19,–,21,36,37 which has been confirmed by drug trials of high quality,2,3 is neglected. The risk of side effects from phenytoin, most of which are dose related should be less when it is used as an AIAA, requiring lower dosage and blood level than for seizure control.20 Nonetheless, when it is used to treat both seizure disorder and impulsive aggression, the higher dose for seizure control is necessary, but it increases the risk of side effects that occur in the pharmacotherapy of seizure disorder, in any event. Still, by using only one drug instead of two for the two conditions, the risk of side effects is limited.
In the United States, seizure disorders are typically treated by neurologists with whom the psychiatrist can work in collaboration. Of the anticonvulsant AIAAs, phenytoin, carbamazepine, and valproic acid are used to treat tonic-clonic and focal-onset seizures. Valproic acid is also efficacious for absence, atypical absence, and myoclonic and atonic seizures.74 With the dual-purpose use of an anticonvulsant AIAA, both neurologist and psychiatrist can monitor for neurologic and systemic side effects, some of which develop after extended use, such as the gum hyperplasia associated with phenytoin, the aplastic anemia caused by carbamazepine, and the hepatotoxicity related to valproic acid.
If a woman with epilepsy who has impulsive aggression becomes pregnant, she should be continued on the anticonvulsant, because the risk of teratogenic effects of anticonvulsant medication is less than the potential harm to mother and fetus that could be caused by uncontrollable convulsive seizures.74 In this case, it can be especially prudent to take advantage of the two-for-one effects of an anticonvulsant AIAA. Precautions to reduce the risk to the fetus include:
mono-anticonvulsant therapy, with, if possible, the lowest effective dose in the first trimester;
prescription of a folate to reduce risk of neural tube defect and of oral vitamin K in the last two weeks of pregnancy as prophylaxis against transient deficiency in vitamin K-dependent clotting factors; and
intramuscular administration of vitamin K to the infant at birth.74
If the type and frequency of seizures allow the woman to be withdrawn from anticonvulsant medication before conception, then the co-occurrence justification does not exist.
Psychopharmacotherapy History
Obtaining the patient's psychopharmacotherapy history is an important step in psychiatry generally. For impulsive aggression secondary to another disorder (not the topic of this algorithm), the importance is obvious. If a bipolar patient's impulsive aggression secondary to mania was effectively controlled in the past with lithium, for example, this history can usefully inform the current pharmacotherapy treatment plan. Before prescribing fluoxetine, lithium, or an anticonvulsant AIAA, an inquiry should be made about the patient's experience with AIAAs, and the adequacy of trials and the drugs' effects, including impacts on aggressive behavior, both favorable and adverse should be determined.
Affordability and Availability
Not often mentioned in scientific articles is the reality that a medicine must be available and affordable to the patient. Medicine has no effect if it is not taken. If the prescribed medicine is unavailable or unaffordable, it cannot be prescribed. The AIAA may be on the hospital formulary and easily administered while the patient is in the hospital, but if it is not affordable, the patient will not be able to obtain it after discharge. Likewise, if the patient is returned to a jail from a security hospital, it is more likely that the AIAA will be continued if it is on the jail formulary. Consideration of its affordability and availability can be critical therefore when deciding which AIAA to prescribe for treatment of impulsive aggression.
Discussion
The treatment of and pharmacotherapy for IED are addressed in one of psychiatry's major text books.76 The present, more expansive algorithm for the selection of AIAAs in clinical practice places two considerations at the forefront: identification of efficacious AIAAs based on drug trials of sufficient quality and proper characterization of the aggressive behavior of individual patients. It is less important that the other steps be addressed in any particular order, so long as all steps are methodically addressed.
Before the improved characterization of impulsive aggression and higher quality drug trials of AIAAs, the received wisdom was to select a drug that would be used to treat the mental disorder that comes closest to the patient's condition. For example, if the aggressive behavior occurred within the context of hypomanic traits, a mood stabilizer would be selected; if in the context of schizotypal traits, an antipsychotic would be chosen. This rule of thumb has merit if prudently applied. Impulsive aggression can be the principal clinical concern, as discussed herein, but it can also be secondary to another disorder with known pharmacological treatment. It then makes sense to select a medication specifically to treat the principal disorder. Such a treatment has been discussed before for aggression secondary to schizophrenia and psychotic disorders, delusional disorder, bipolar disorder, depression, and traumatic brain injury.1 Other decisional trees for pharmacotherapy for clinical aggression include aggression secondary to a principal mental disorder.5,–,7,9 These algorithms are for the treatment of clinical aggression in general and are not limited to impulsive aggression. Indeed, aggression secondary to another mental or medical disorder is often controlled with efficacious treatment of the principal disorder, and the question as to whether such secondary aggression is also impulsive may seem inconsequential.
Where the aggression that occurs together with another mental disorder does not subside with appropriate treatment alone, clinicians often add a mood stabilizer, particularly if the aggression has an affective component. A better practice would be to characterize the aggressive behavior initially, even if it occurs in the context of a co-occurring mental disorder.25 Proper identification should result in more efficient and effective treatment. Aggression that occurs together with another disorder may or may not be secondary to that disorder. Moreover, the causal distinction is not always easily and clearly made. Much of the aggressive behavior that has been reported in association with schizophrenia, for example, is not the result of delusions, command hallucinations, or disorganized thinking, but is impulsive,18 perhaps a function of destabilization that does not amount to psychosis or a result of impaired executive function in the frontal lobes.
A recent review of pharmacotherapy for clinical aggression in general,77 together with its earlier companion article on a translational approach,50 usefully summarizes potential molecular antiaggressive mechanisms of various drugs, though it is not specific to impulsive aggression. The authors advocate using a combination of antipsychotic and antiepileptic medications without regard to specific psychopathological disorders. This approach may be more appropriate for aggression in schizophrenia spectrum disorders than for primary impulsive aggression. In any event, we recommend the more conservative approach described herein, with the objective being the evidence-based reduction of impulsive aggression with a single agent.
Our focus is on pharmacotherapy for impulsive aggression that is not secondary to another disorder. The question arises, however, as to whether aggression that occurs together with the character pathology of Cluster B personality disorders10,11 can be primary impulsive aggression or whether it should be parsimoniously attributed to the personality disorder for which impulsive aggression can be symptomatic and diagnostic. If, in using DSM diagnostic criteria, the aggressive behavior is attributed to the personality disorder, it can lead to a decision not to treat with an AIAA. Yet, drug trials have demonstrated efficacy in the treatment of subjects with an AIAA who have a personality disorder: borderline personality disorder in fluoxetine trials28 and antisocial personality in phenytoin trials,19,20 for example. Thus, our decisional method for pharmacotherapy for impulsive aggression does not exclude patients with borderline or antisocial personality disorder.
If a personality disorder should not bias clinicians against treating co-occurring impulsive aggression, should the particular personality disorder help guide the selection of an AIAA? There has been a tendency for mood stabilizers to be used more in drug trials in individuals with antisocial personality disorder and SSRIs in those with borderline personality disorder. One might consider the agent that has been shown to be efficacious with a given impulsively aggressive personality disorder. Of the mood stabilizers, valproate/divalproex appears to be most effective in impulsively aggressive individuals with borderline personality disorder.78,–,81 Thus, valproate/divalproex pari passu would be a reasonable first choice among mood/stabilizing AIAAs for impulsively aggressive patients with borderline personality disorder. If the aggression is high frequency/low intensity and is associated with a personality disorder (a borderline personality disorder, particularly), a risk–benefit analysis suggests a trial with fluoxetine, and if that is ineffective, treatment with divalproex.79
In several drug trial studies, only individuals with personality disorders were included. The 2011 study by Coccaro31 that led to the changes in diagnostic criteria for IED in DSM-5 included only those individuals. In that study, which was not a drug trial, but was intended specifically to contribute to IED criteria, more personality disorders fell into Cluster B, but Clusters A and C were also well represented. Only personality-disordered subjects were included because Coccaro recruited subjects from another study that had required the presence of personality disorder for inclusion. Paradoxically, recent editions of the DSM, including the current one, consistently tended to exclude personality disorders in diagnosing IED. Even though the exclusion was dropped from the original research criteria for IED developed by Coccaro and colleagues,29 efficacy studies best support use of AIAAs in impulsively aggressive individuals with personality disorders. It may therefore be concluded that the efficaciousness of AIAAs has not been strongly enough demonstrated to be used in individuals without a personality disorder and should therefore be prescribed only in individuals who have one. Certainly more AIAA drug trials are needed in subjects without personality disorders.
Meanwhile, it is advised that patients with impulsive aggression not be denied pharmacotherapy because they lack a personality disorder. Note that the personality disorders in Coccaro's 2011study31 were not limited to a specific personality disorder or even to one of the three clusters. Although impulsive aggression was well represented among subjects with bipolar disorder (11.9%) and antisocial personality disorder (14.4%), according to the research criteria, these disorders were present in only a fraction of the total number of subjects with IED. Impulsive aggression is best conceptualized as both a disorder and a dimension that is not specific to any other disorder.15 Hollander et al.82 found divalproex to be preferentially effective in reducing aggression among individuals with Cluster B personality disorders and borderline personality disorder, leading to the conclusion that divalproex is effective primarily for the treatment of aggression in individuals with personality disorders.82 Personality disorder should neither bar nor exclusively indicate pharmacotherapy with an AIAA.
Elsewhere, psychostimulants have been recommended as the first choice in treating impulsive aggression. Donovan and Aybar83 defined impulsivity as acting without thinking and limited impulsive aggression to that associated with ADHD. They cited evidence that methylphenidate improves disruptive behavior in children with ADHD.84 Indeed, a drug trial with d-amphetamine85 made the second tier in the quality comparison by Felthous and colleagues.2 The Amery study86 included boys, not adults. The concern here is primary impulsive aggression, not aggression known to be secondary to another condition. Atomoxetine (Strattera; Eli Lily & Co., New York, NY) has been approved for treatment of ADHD in adults, including prisoners, but proper diagnosis of ADHD is critical and, apart from atomoxetine, psychostimulants are tightly controlled in correctional settings because of the risk of abuse. Although stimulants may improve aggressive behavior in children with ADHD, it is not clear that they have the same result for severely aggressive behavior in conduct-disordered children87 or in adults with impulsive aggression. Research is needed that compares AIAA and psychostimulants in controlling impulsive aggression in adults with and without ADHD.
Fortunately, none of the well-tested AIAAs is known as a drug of abuse. This cannot be said for psychostimulants whose use is strongly discouraged in jails and prisons because of their potential for abuse.88 Benzodiazepines and other strongly sedative drugs should be avoided for long-term treatment of impulsive aggression for the same reason. Antipsychotics, such as risperidone, are first-line agents in the treatment of psychotic disorders and associated aggressive behavior,1,9 but should not be considered as first-line agents for impulsive aggression that is not associated with another mental disorder. The quetiapine experience is instructive, in that this drug was used, perhaps effectively, for a wide range of off-label indications, including irritability and aggression. Quetiapine abuse became problematic in jails and prisons89 and in the community. It has come under better control in prisons and jails,89,90 and hospitals and clinics are becoming aware of its risk for abuse. Antipsychotics, particularly quetiapine, should be avoided in the treatment of impulsive aggression. Moeller and Swann9 recommended risperidone, but only after more appropriate agents have been tried and have failed.
Conclusions
Research supports the use of certain AIAAs in the treatment of impulsive aggression that has been adequately defined and diagnosed, even if no AIAA is FDA approved for this indication. Research reports alone, however, do not inform the clinician as to which AIAA would be the best selection for a particular patient with primary impulsive aggression. The present review is intended to initiate discussion of a pharmacotherapeutic algorithm for impulsive aggression, if not provide useful clinical guidance. Five factors in particular are recommended for consideration when selecting an AIAA. A more definitive algorithm must await further research that compares efficacy and risks of different AIAAs on different subsets of IA patients and in different patient populations.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2015 American Academy of Psychiatry and the Law
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵





{kind=link}