


Abstract
Use of a conducted-energy device (CED), or Taser, by law enforcement officers (LEOs) is recommended over more lethal forms of force. LEOs interact with a wide variety of people including individuals with mental illness and those with substance use disorders. The literature is devoid of data regarding the effect of CEDs on this special population. We used data collected by LEOs from 2008 to 2009. There were 233 cases over the two-year period. Of the 233 individuals on whom the Taser was used, 38 had a mental illness and 91 were under the influence of substances (not mutually exclusive). The average number of shocks necessary to achieve compliance was 1.92 for persons with a mental illness (t(231) = 2.565; p = .011, versus nonintoxicated control subjects without mental illness and 2.55 for persons under the influence of stimulants (t(143) = 3.027; p = .003, versus nonintoxicated control subjects without mental illness). The results of this study serve to inform LEOs and administrators of the patterns of use of CEDs in communities.
The conducted-energy device (CED), or Taser (Thomas A. Swift's Electric Rifle, and also a brand name) is a new tool for law enforcement officers (LEOs) to gain control in potentially dangerous situations with less than lethal force. As the name suggests, these devices send an electrical current through the recipient's body. There are two main modes of applying a CED: the drive-stun mode and the probe mode. Drive-stun requires the handler to drive the electrodes on the device into the recipient's body before delivering a shock, coming into direct contact with the recipient. Probe mode is a method by which the handler can deploy the electrodes, which shoot out as darts, from a distance of up to 25 to 35 feet, depending on the type of CED, to deliver shocks to the recipient.1 The “electrical charge overrides the central nervous system, resulting in the loss of neuromuscular control,” involuntary muscle contractions, and fatigue, which give the administrator a brief window of time to gain control over the subject (Ref. 2, p 173). For this reason, more police departments now routinely use CEDs, and they have become part of the average law enforcement officer's weaponry.3
Although CEDs have helped minimize the use of other forms of escalated force, such as guns, controversy remains over the use and abuse of CEDs in certain populations, such as people with mental illnesses.5 The primary objective of this study was to examine the differences in use of CEDs between populations with and without mental illnesses.
Methods
The data used in this study are a subset of results from a U.S. nationwide prospective study of injury among individuals who had less-than-lethal weapons used against them for purposes of compliance with the police. (Unfortunately, it has never been published.) The original study used a standardized case report form documenting nonlethal weapon use. The date, type of incident, if the individual had a mental illness (according to Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) criteria4, which are similar to Fifth Edition (DSM-5)5 criteria), age, sex, intoxication status (confirmed by a toxicology report), if the individual was admitted to the hospital or died, weapon type, additional force used, medical evaluation provided, impact and injury sites, and additional comments were collected. Alcohol and drug levels were obtained with a toxicology screen. The LEO responding to the scene of the incident completed the form. In cases of missing or unclear information, the same LEO was contacted for further information or clarification. This project had Institutional Review Board (IRB) approval from the University of Louisville Hospital Research Integrity Office.
For the current study, two years' (2008 and 2009) worth of data were made available from one of the sites, Louisville, for secondary data analysis. Only Taser data were used, eliminating those data collected on the use of other less lethal weapons, such as pepper-ball guns and beanbag shotguns (used only 3 times over the 2 years of observation). Variables of interest were the presence of a mental illness, drug possession or use, additional force used, number of shocks administered, and compliance after application of the CED. A database was created using Statistical Package for the Social Sciences version 21 (SPSS). Data were recorded for 17 variables, and the computer program was used to generate independent samples t-tests, a two-way ANOVA, and descriptive statistics, when appropriate.
Results
The sample size was 238 individuals. Of those, 16.3 percent (n = 38) had a mental illness and 83.7 percent (n = 195) did not; information was missing for 2.1 percent (n = 5) of the sample. Thus, the final sample consisted of 233 individuals. The age of individuals ranged from 15 to 63 years (average, 32.8). The median age was 31.0 years, and the mode was 27.0 years. The majority, 93.6 percent, were male (n = 218) and 6.0 percent (n = 14) were female; 0.4 percent of data were missing for this variable (n = 1).
Drugs were confirmed present in 82 cases (35.2%), absent in 134 cases (57.5%), and suspected in 11 cases (4.7%). Data for this variable were missing in 6 cases (2.6%). Of those cases with drugs present, 11 (4.6%) were under the influence of a stimulant, 62 (26.1%) were under the influence of alcohol, 9 (3.8%) were under the influence of other drugs, and 9 (3.8%) were under the influence of multiple drugs.
Additional force was used to gain compliance in 118 cases (50.6%), with data missing for 2 cases (0.9%). Physical restraint, such as empty-hand control, was the most common use of additional force (n = 106), impact weapons were used in 2 cases, and multiple means were used in 10 cases. Six of the cases were suicide attempts. One death was caused by Taser use. No additional adverse effects were documented that were associated with the use of a CED.
Of the 233 individuals, 6.0 percent (n = 14) were not compliant, 13.7 percent (n = 32) were partially compliant, and 79.4 percent (n = 185) were compliant after receiving shocks; the level of compliance was missing in 0.9 percent (n = 2) of the reports. The average number of shocks administered was 1.6, and the minimum, median, and modal number of shocks administered was 1; the maximum number of shocks delivered was 6. One shock was administered in 146 of the cases, two shocks in 59, three shocks in 17, four in 5, five in 5, and six in 1. The data are summarized in Table 1.
Summary of Sample Size and Mean Number of Shocks for Each Variable
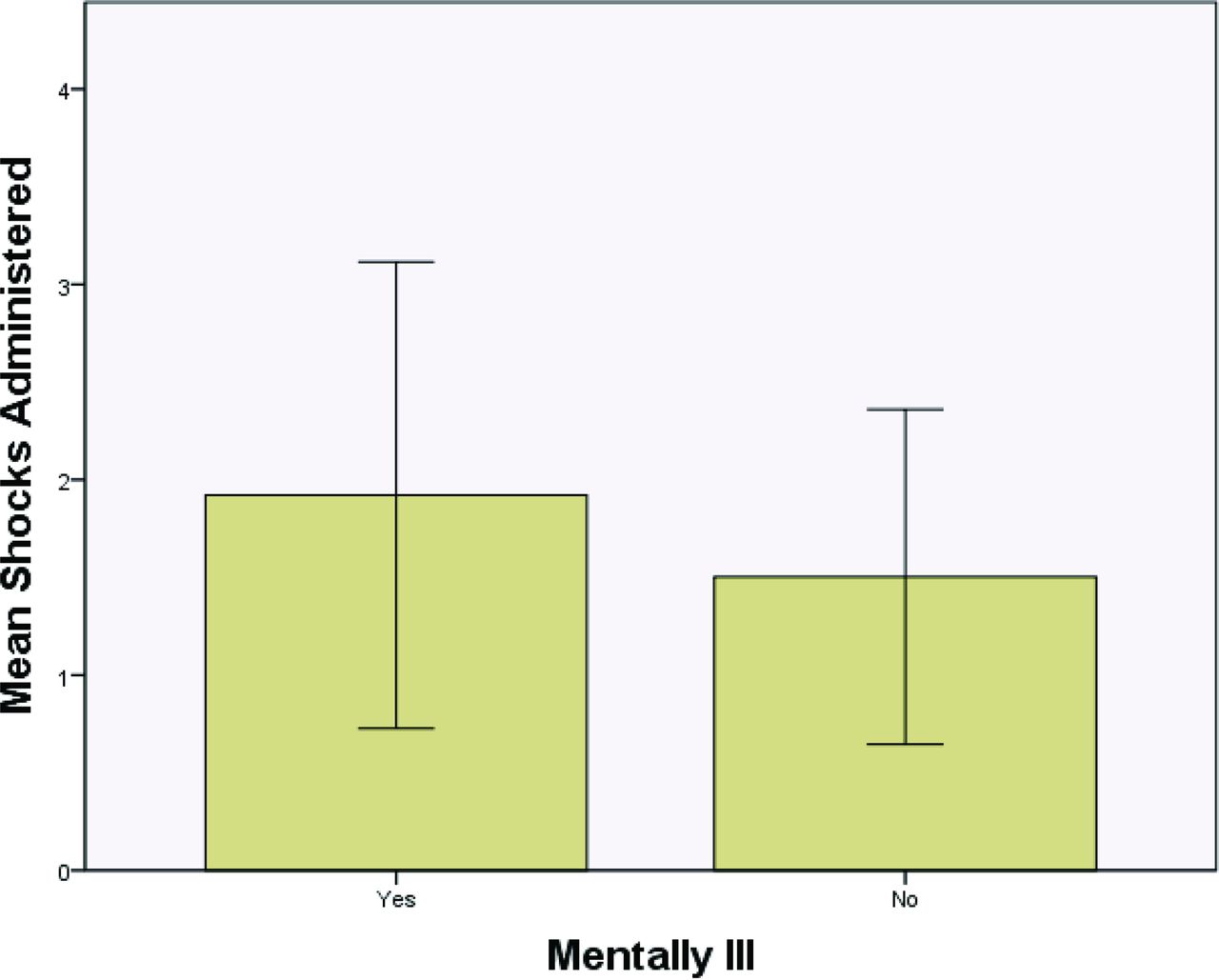
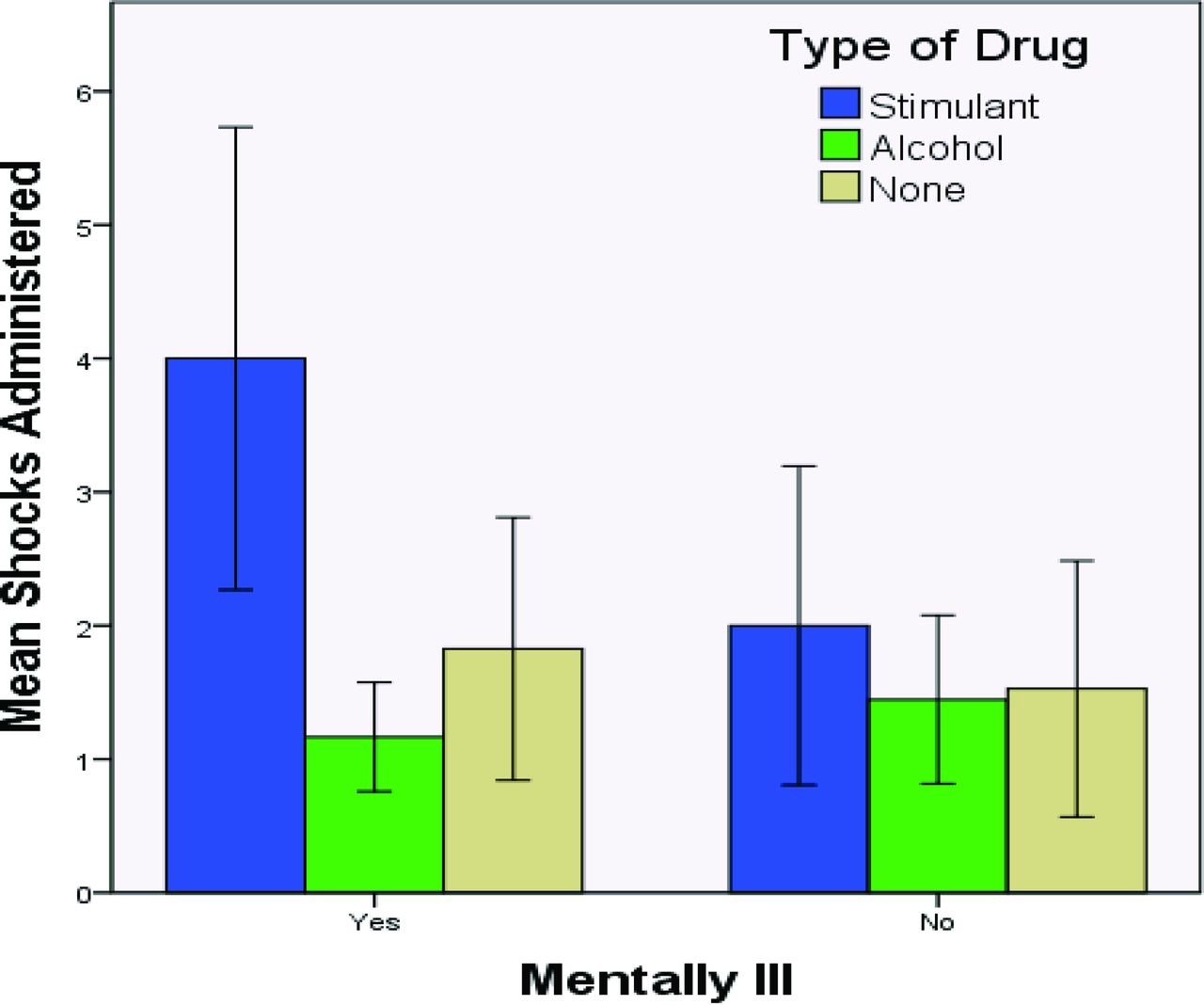
Individuals with mental illness received shocks significantly more times than those without mental illness (t(231) = 2.565; p = .011) (Fig. 1). Overall, there was no difference in the number of times individuals were shocked, based on whether they were under the influence of substances as an aggregate category (t(224) = .036; p = .971). The mean number of shocks administered on individuals under the influence of a substance was 1.58 ± 0.908 (SD) versus 1.58 ± .966 for individuals who were not under the influence of a substance. However, there was a significant interaction between the presence of substances and mental status on number of shocks delivered by LEOs (ANOVA, F(3,48.601) = 5.593; p = .002). Individuals who had mental illness and were affected by the use of stimulants required significantly more shocks than those using stimulants without a mental illness (Fig. 2). For individuals who were under the influence of alcohol, the number of shocks administered was only slightly greater for those individuals who also had mental illness compared with those who did not (Fig. 2).
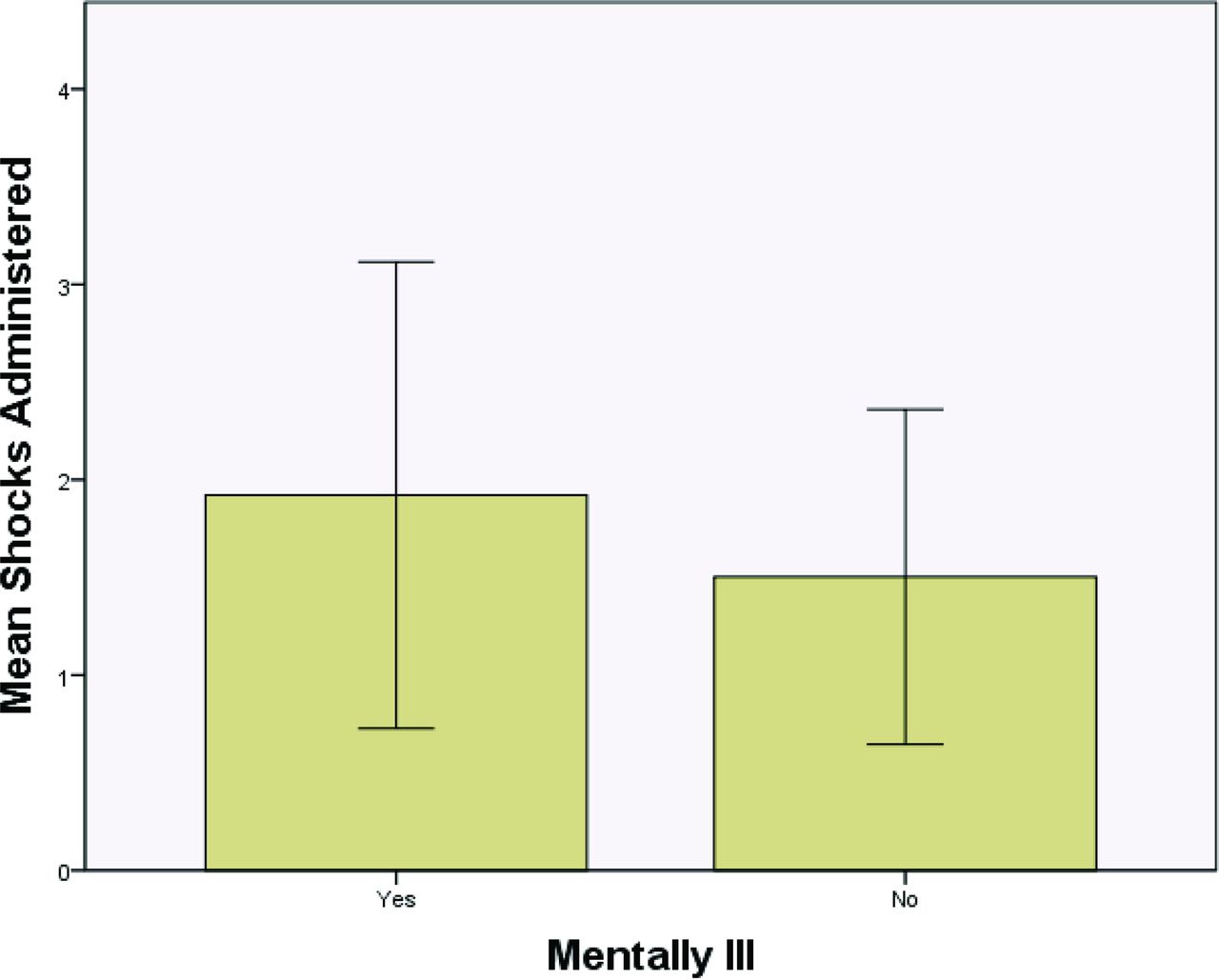
The mean number of shocks delivered to individuals, with or without mental illness. Those with mental illness were shocked significantly more times than those without (mean 1.92 ± 1.194 (SD) versus 1.50 ± .858; t(231) = 2.565; p = .011).
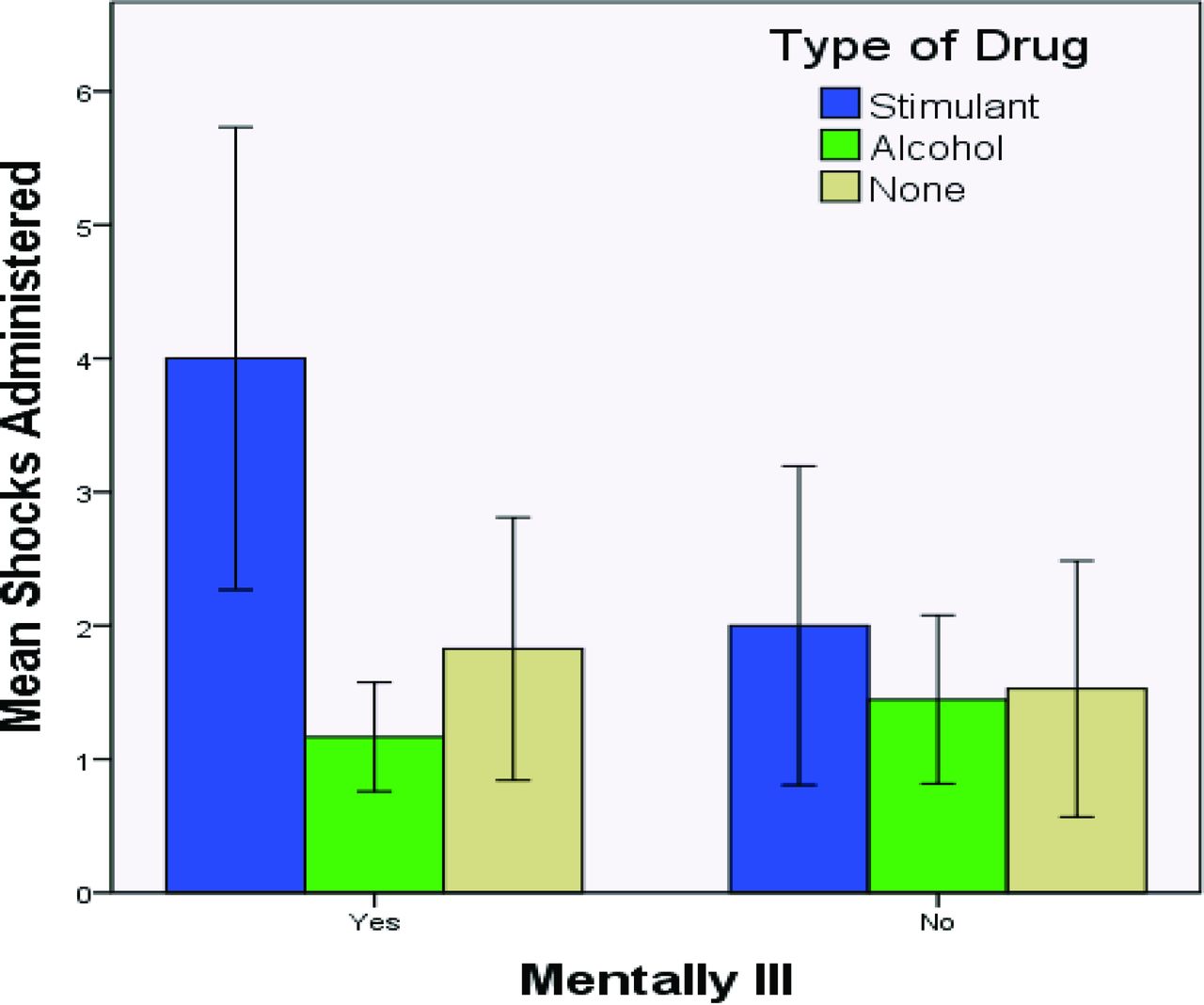
The number of shocks delivered to subjects with or without mental illness, in the absence or presence of alcohol or stimulant abuse. Bars are means and standard deviations. Individuals with mental illness under the influence of a stimulant were shocked significantly more times than those under the influence of alcohol (t(7)= 4.056; p = .005). Similarly, those with mental illness and under the influence of a stimulant were shocked significantly more times than those who were not under the influence of any substance (t(24)= 3.320; p = .003). Individuals without mental illness under the influence of a stimulant are shocked significantly more times than those under the influence of alcohol (t(62)=2.044; p = .045).
Stimulant use was associated with a significantly higher number of shocks, independent of the presence of a mental illness (t(143) = 3.027; p = .003) (Fig. 3). The mean number of shocks administered to individuals under the influence of a stimulant was 2.55 (SD = 1.572) and to individuals under the influence of alcohol was 1.42 (SD = 0.615).

The mean number of CED shocks delivered as a function of the substance used. Bars are means and standard deviations. Individuals under the influence of stimulants were shocked significantly more times than individuals under the influence of alcohol (t(71) = 4.194; p = .000) or individuals who were not under the influence of any substance (t(143)= 3.027; p = .003).
Discussion
We undertook an examination of the use of CEDs by LEOs to determine whether there was a difference in outcome if the subject had mental illness, substance abuse, or neither. We could not document a difference in adverse events secondary to CED use. However, persons with a mental illness (Fig. 1), or with stimulant use (Fig. 3), or both (Fig. 2) receive significantly more CED shocks than individuals without these characteristics.
There is very little research available on the influence of mental illness on CED use. CED use by the police began in the mid 1970s.1 Studies by the U.S Bureau of Justice Statistics (1999) (Ref. 6, p72) indicate that police use force in only “about 1 percent of all police-citizen encounters,” and CED use accounts for only a fraction of the uses. The low frequency of CED use makes research more difficult.
The limited research has shown that CEDs have been effective in reducing escalation to deadly force by LEOs in situations where they or the subjects were in danger.7,–,9 This has prompted national organizations such as the American Medical Association10 and the National Alliance on Mental Illness11 to support the appropriate use of CEDs. The current study supports this position. Nonetheless, the safety of the use of CEDs has repeatedly been a point of concern, partially due to some documented deaths (including one case among the individuals that we studied).3,6,12,13 The exposure of some vulnerable populations has also been a concern. In this examination of the effect of an underlying mental disturbance, we found that the type of mental disturbance may influence the number of shocks used by LEOs to gain compliance. Specifically, the Taser is used on individuals with mental illness, on average, 28 percent more frequently than on those without a mental illness. Likewise, it is used on individuals who are under the influence of stimulants 61 percent more frequently than on those who are not. Conversely, alcohol does not appear to play a significant role, despite the lower number of CED uses (11%) on those consuming alcohol than on those who were not using any substances.
One study grouped drugs and alcohol into a single category: intoxication.6 Whether for convenience or because of sample size, it is clear, based on our findings and because of the differing effects on the brain and body of the various types of drugs, that the categories of drugs should be analyzed separately. The same study lists intoxication as a risk factor for resistance by the suspect. The ratio of people on drugs to the number of intoxicated people was 7.1:12.8, meaning that 55.5 percent of people in that study were under the influence of drugs alone, and 44.5 percent were under the influence of alcohol alone. Of these individuals, 56.8 percent continued to resist after receiving a shock, but the study did not classify them according to drug consumed.
It is known that a subject's demeanor, hostility, and impairment are the strongest influences on police discretion in the use of force.14,–,16 The data also suggest that subjects with mental illness or under the influence of substances present themselves in a manner (i.e., more violent, hostile, resisting, and nonsensical) that correlates highly with a greater risk of use of stronger force.12,17,18 For this reason, individuals with mental disturbances may be at an increased risk of having an LEO use a CED as a means of gaining compliance. Furthermore, substance abuse and mental illnesses commonly coexist,16 and as we have shown; there is a significant interaction between mental illness and substance use on number of shocks used to gain compliance, with the mental illness intensifying the effect of the drug alone (Fig. 2). Collectively, these data suggest that individuals with mental disturbances have an increased likelihood of being subdued by Taser and being shocked more times during their interaction with a police officer. Although special LEO groups, commonly referred to as crisis intervention teams (CITs), who are specifically trained to identify individuals with mental illness, have helped reduce the use of force against such persons9,16,19 and have decreased the injury rate of police officers by sevenfold,19,20 such programs are not widespread enough to be effective.
In 2004, Amnesty International called for a moratorium on the use of CEDs by LEOs because of 74 deaths that had occurred after their use from 2001–2004.6 Multiple studies list illegal drug use, in conjunction with the effects of CED, as the most common risk factor that influences chances of death after being shocked; other factors include mental illnesses and pre-existing medical conditions, such as heart disease.1,2,6,7,13 White and Ready6 suggested that medications used by individuals with mental illness may increase the risk of death caused by the use of a CED. Researchers who studied 16 deaths associated with CEDs found that eight of the individuals were under the influence of phencyclidine (also known as PCP), seven were under the influence of a stimulant, and one had a pre-existing heart condition.1 In our study, of the 11 individuals who were under the influence of a stimulant, 1 died en route to the hospital after two shocks. Studies on the effect of consensual CED use on the heart generally show only tachycardia as a consequence,21,22 but law enforcement does not recruit vulnerable individuals.13 It is prudent to follow the American Medical Association recommendation and evaluate persons who have been shocked with a Taser in an emergency department.
One of the main limitations of the current study is the small sample size of individuals in certain categories. For example, only 11 individuals were under the influence of stimulants, and 38 had a mental illness. Nonetheless, even with this small number, the effect size of CED use was sufficient to reveal a significant consequence. Certainly, future research would benefit from augmenting the number of individuals in each category to make the findings more generalizable. Another limitation is that we reviewed only the effect of mental illnesses as an aggregate group on number of shocks received. Furthermore, there was no confirmation of the mental illness with a mental status examination. Finally, we examined only the effect of stimulants and alcohol on CED use. We did not separate cocaine and amphetamines. Since the various drugs have different effects on the brain and body, future research would benefit from examining the effect of all the different classifications of drugs.
Despite these limitations, this study shows that mental illness and substance intoxication can reduce the effectiveness of CED on an individual. Both a history of mental illness and use of stimulants on a person with mental illness can result in a greater CED dose than that applied to individuals without mental illness. These same populations have been reported as being more vulnerable to complications from CEDs.8,23,24 This study raises the possibility that the increase in adverse consequences of CEDs is related to dose, rather than, or in addition to, a pre-existing physiologic vulnerability. The current results direct research to examine the effects of multiple shocks at the interval at which they are administered in the field. As more is known about mental illnesses, preclinical studies may be able to model different physiologic changes in experimental animals, to determine which aspects actually increase risk of complications. In the intervening time, this knowledge allows reasonable policies to be put forward by both law enforcement and mental health organizations.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2016 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}
{kind=link}