


Abstract
There are an estimated 60,000 evaluations annually for competence to stand trial for felony indictments and likely more for misdemeanor indictments. Thus, there is an increasing interest in determining factors associated with a defendant's likelihood of being restored to competence to stand trial. Although previous studies have found that a misdemeanor charge predicts significantly less likelihood of restoration of competence when compared with felony charges, states typically allow treatment facilities less time to restore misdemeanor defendants than felony defendants. As there are no studies examining factors associated with restoration of competence to stand trial for misdemeanor defendants, separately from felony defendants, we conducted a retrospective study to examine demographic, clinical, and forensic characteristics associated with restoration of competence to stand trial of misdemeanor defendants. Almost 70 percent of defendants regained competence to stand trial during the study period. When restorable, defendants regained competence in less than three weeks, on average, which addresses a current question in the field regarding time limits for restoration of competence to stand trial. Single marital status and length of stay in the treatment facility during restoration of competence to stand trial were significantly associated with restorability. States may consider such factors when developing and reviewing time limit policies in consideration of the Jackson v. Indiana ruling and when designing interventions aimed at restoring competence to stand trial to misdemeanor defendants in a cost-efficient manner.
In the 1960 landmark case Dusky v. United States, the United States Supreme Court affirmed a defendant's right to an evaluation of his competence to stand trial.1 The Court outlined that the defendant must have “sufficient present ability to consult with his lawyer with a reasonable degree of rational understanding” and “a rational as well as factual understanding of the proceedings against him” to undergo criminal proceedings (Ref. 1, p 402). Since the Dusky decision, each United States jurisdiction has developed statutes regarding competence to stand trial and procedures for evaluation and determination of a defendant's competence. Most of these criteria are similar to those of the Dusky standard. Today, competence evaluations are the most commonly performed forensic examinations in the United States. There are an estimated 60,000 evaluations per year for felony indictments and a likely greater number for misdemeanor indictments.2
Competence evaluators find about 20 percent of individuals evaluated for competence to stand trial are incompetent; courts refer these individuals for treatment or education known as competence restoration, to enable them to become competent to stand trial.2,–,5 Based on the ruling of the 1972 landmark case Jackson v. Indiana,6 state statutes place a limit on how long an inmate can be held for restoration of competence to stand trial. The Court held that an incompetent defendant “cannot be held more than a reasonable period of time necessary to determine if there is a substantial probability that he will attain competency in the foreseeable future” (Ref. 6, p 739). The Court was unwilling to define a “reasonable period of time” because of differences in state policies and resources. This deference to the states resulted in various time limits for restoration of competence to stand trial. Though most states revised their statutes in response to the Jackson ruling, states continue to differ in how closely they follow the spirit of Jackson.7
The Jackson decision resulted in some challenges related to the restoration of competence of misdemeanor defendants. Many states provided noticeably shorter times to restore those charged with misdemeanors than those charged with felonies. This occurred in the absence of any evidence that misdemeanor defendants require less time for competence restoration than their felony counterparts. In fact, the guidelines were developed without consideration of the clinical characteristics of this population.8 In a recent study, Mossman9 found that a misdemeanor charge predicts significantly less likelihood of restoration of competence when compared with felony charges, in agreement with an older study.10 Misdemeanor defendants may be restored to competence less often, because the time allowed for assessment and treatment expires.9 Alternatively, incompetent misdemeanor defendants may experience more severe psychiatric symptoms that preclude their ability to assist their counsel or to understand the legal proceedings. Although allowing an excessive amount of time for assessment and treatment may postpone a defendant's right to due process and result in excessive costs to the system (as in Jackson), providing inadequate time may restrict a defendant's constitutional right to stand trial in a competent mental state.
There is increasing interest in determining factors that predict a defendant's likelihood of restoration of competence to stand trial. Several studies identify key factors, including a diagnosis of schizophrenia or schizoaffective disorder, severe psychiatric symptoms, cognitive impairment, and a deficit in psycholegal abilities, as predictive of a finding of incompetence to stand trial, preceding and during treatment.11,12 In addition, nonrestorable defendants tend to have prior episodes of incompetence and are prescribed more medications when undergoing restoration.13 In the 2003 case of Sell v. United States,14 the United States Supreme Court outlined several criteria, one of which is whether important government interests are at stake, to consider before administration of court-ordered involuntary medications for competence restoration. Few studies have been completed since the Sell ruling, and of those studies, none examined specifically whether a forced-medication order improves a defendant's likelihood of restoration. However, one case series noted that involuntary medication seems to restore some defendants with delusional disorder to competence.15
There are no available data on the demographic, forensic, and clinical characteristics of misdemeanor defendants referred for treatment for restoration of competence to stand trial. Many studies examine the violent nature of a defendant's charge,3,9,11,–,13,16,17 but do not separately evaluate the characteristics of misdemeanor defendants, despite the more stringent time requirements imposed on those restoring misdemeanor defendants. We hypothesized that the misdemeanor defendants who are restored to competence to stand trial have demographic, clinical, and forensic characteristics that differ from those of misdemeanor defendants who are deemed unrestorable. Identifying such factors may inform treatment interventions and state policy aimed at compliance with the Jackson ruling.
Methods
Setting
We conducted the following study in Sacramento County, California. In California, mental health facilities have one year to restore a misdemeanor defendant to competence to stand trial or to determine the defendant to be nonrestorable. The Sacramento County Superior Court refers incompetent misdemeanor defendants to the Sacramento County Mental Health Treatment Center for treatment to restore competence and refers felony defendants to a separate hospital system. We were able to collect data specific to misdemeanor defendants based on the separate assessment and treatment of defendants based on the seriousness of their charges.
We examined data obtained during admissions that occurred from 2004 through 2012 at the Sacramento County Mental Health Treatment Center, a public-sector inpatient psychiatric facility in Sacramento, California. During the study period, the Sacramento County Superior Court referred all misdemeanor defendants in Sacramento County who had been found incompetent to stand trial to this facility for treatment to restore competence. The court suspended the legal process pending treatment.
Upon defendants' admission to the treatment facility, a team consisting of a psychiatrist, a resident psychiatrist, a nurse, a social worker, and a psychologist assessed and treated them. The treatment team provided psychoeducation about each defendant's psychiatric disorders and education about the legal process; administered psychotropic medications; and provided group psychotherapy, which included mental health education, substance abuse education, recreational therapy, and relaxation techniques. The treatment team conducted regular clinical assessments to decide whether a defendant had regained competence to stand trial or whether a defendant was not likely to be restored within the allowable time frame. The treatment team assessed competence by evaluating the defendant's ability to articulate his knowledge about the legal process consistently, including the specifics of his case, and by observing his level of participation in treatment. During the latter portion of the study period, the team routinely used competency testing instruments, such as the Georgia Court Competency Test (GCCT)18 or the Competency Assessment Instrument-Revised (CAI-R),19 as part of the ongoing clinical assessment of competence. Upon restoration of competence to stand trial, the team referred the defendant to the court to resume the legal process. The court determined the disposition of defendants deemed unlikely to be restored to competence.
Statutory Schemes
Beginning in 2003 with Sell v. United States, courts could refer defendants for treatment with an order to administer psychotropic medications on an involuntary basis if the defendant refused treatment. In 2008, Sacramento County Superior Court judges began to issue forced-medication orders. If the court referred a defendant without a forced-medication order, treatment proceeded without the use of medication. In these instances, if the defendant was not regaining competence to stand trial by a certain point in treatment and refused the use of medication in his treatment, the team suspended treatment pending transfer of the defendant to jail to await a ruling regarding involuntary administration of psychotropic medications.
Procedures
Before data collection, the Institutional Review Board at the University of California, Davis, and the Sacramento County Department of Health and Human Services Research Review Committee approved the study protocol. Upon approval by both governing boards, we obtained demographic, clinical, and forensic data from electronic and paper charts for the 221 admissions of the misdemeanor defendants whom the court referred and who completed treatment for restoration of competence to stand trial from 2004 through 2012. Please refer to Figure 1 for the selection of admissions included in the data analysis.
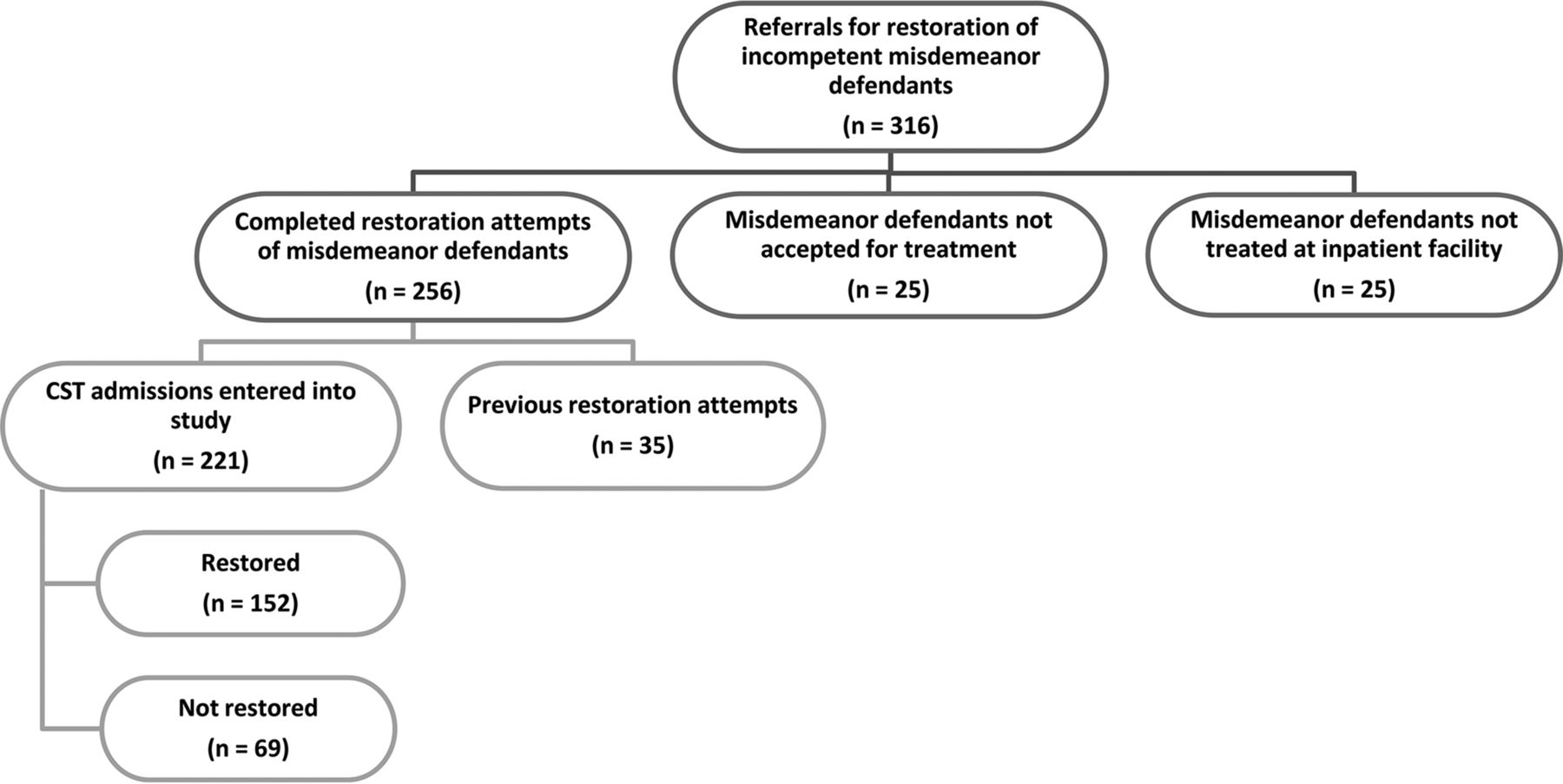
Selection of misdemeanants treated for competency restoration for inclusion in the data analysis.
The Sacramento County Superior Court referred a total of 316 misdemeanor defendants to the inpatient psychiatric facility during the study period for treatment to restore competence to stand trial. We excluded data for misdemeanor defendants who were referred for restoration of competence to stand trial but who did not complete treatment at the inpatient psychiatric facility. The facility did not accept 25 defendants, primarily because of the presence of a cognitive disorder, such as dementia. The facility accepted 25 other defendants, but did not treat those individuals for reasons not specified in the defendant's legal file. The treatment team completed a total of 256 restoration attempts during the study period. The court referred some defendants for restoration more than once. In those instances, we included data for the most recent attempt at restoration to examine whether a history of previous restoration attempts or a history of previous nonrestorability predicts future restorability. We did not include multiple admissions for those defendants, to preserve the assumption of independence in statistical testing.
We queried a computerized database for demographic characteristics of the misdemeanor defendants. We collected data on age at admission, gender, ethnicity, primary language, educational level, marital status, and employment status. We did not have access to data on housing status or income level.
We also queried the computerized database for several clinical characteristics, including year of admission, year of discharge, the number of contacts the defendant had made with the county for inpatient or outpatient treatment before and including the current admission (i.e., episodes), the number of previous inpatient hospitalizations, length of stay, cumulative length of stay, length of time the defendant remained out of the hospital before the reference hospitalization, and Axis I and II psychiatric diagnoses and global assessment of functioning rating on Axis V, based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision.20 We also collected information on insurance status and linkage with an outpatient clinic before admission.
We reviewed each defendant's paper chart to collect data on treatment with psychotropic medications during the admission, such as specific medications and medication classes in addition to administration of involuntary medications, including during instances of seclusion. We also recorded data on the defendant's performance on intelligence and competency testing, when assessed. However, because the treatment team did not refer many defendants for psychological testing and did not use formal competency testing consistently throughout the study period, we did not include those variables in the analyses.
The treatment facility maintains each defendant's legal file separately from the medical record. We queried each defendant's legal file for forensic characteristics, including the referring judge, the competence evaluators, the number and nature of misdemeanor charges, the date of commitment, and the presence of a forced-medication order on the commitment order. After 2008, if a defendant for whom the judge had not issued a forced-medication order before admission refused treatment with psychotropic medications, he was returned to jail pending a ruling regarding involuntary administration of medications and then readmitted to the inpatient psychiatric facility to resume treatment. In these cases, we treated the entire admission as a single episode and collected data accordingly.
We classified misdemeanor charges into three exclusive categories: violent, nonviolent, and sexual. We classified a charge as violent if it included intent to injure another person or being and was not sexual in nature. We classified a charge as nonviolent if it did not include intent to injure another person or being and was not sexual in nature. We classified threats to injure another person or being as nonviolent, because the threat itself did not represent an intent, or attempt, to actually injure the other person or being. We classified a charge as sexual if it was sexual in nature, regardless of whether we could also classify it as violent or nonviolent. We reached group consensus on the classification of each charge. If information regarding a defendant's charges was not listed in the defendant's legal file, we queried the public court website to include the missing data.
Finally, we recorded each defendant's outcome of the restoration attempt, restored or nonrestored, as the outcome variable. If the treatment team determined that a defendant was not likely to be restored, then we noted the basis of that determination (i.e., whether the defendant remained unable to understand the legal proceedings or to assist legal counsel) when available. We also recorded any history of restoration attempts for misdemeanor charges and the outcome of these attempts.
Rationale for Variable Selection
Similar to previous studies, we sought to determine associations between pre- or early admission variables, which are useful in predicting restorability before any restoration attempt.3,4,9,11,12,17 We also sought to understand associations between restorability and those variables for which treatment teams determine the data during the course of a restoration attempt.13 Certain variables, such as the length of stay or treatment with certain classes of medications may be useful in characterizing restorability to inform future predictions of response to treatment.
Outcome Criterion
We used the defendant's outcome after the restoration attempt (restored or not restored) as the outcome variable, consistent with previous studies examining variables associated with restorability.3,4,9,11,–,13,17 In accordance with the rationale used in those studies, the court typically accepts the treatment team's final determination of competence without further assessment. Also, this determination is the most consistent assessment across admissions.
Statistical Procedures
Because of the large number of variables and the small sample size, we used a model selection procedure, as described in detail below, to identify the variables most strongly associated with restorability. In the first stage of model selection, we conducted univariate tests to assess the strength of the evidence of a relationship between each dependent variable and the outcome variable. We used chi-square tests for categorical variables and t tests for continuous variables.
In the second stage, we included all variables that showed statistically significant evidence of a relationship with the outcome variable (at p < .05) and performed multiple logistic regressions. We assessed the intercorrelation of the explanatory variables to remove any variables that could create multicollinearity. When any two variables were significantly correlated with r2 > 0.6, we included only the variable with the lowest p value in the univariate test. We did not include explanatory variables for which there were many subjects with missing values, regardless of the significance of the p value. We used backward selection to reduce the model to those explanatory variables for which there was the strongest evidence of a relationship.21,22 We considered p ≤ .05 significant. We did not correct for multiple testing, because our aim was to build a multivariate model that identified possible associations while controlling for any confounding variables. Controlling the global type I error can lower the power to identify associations in a multivariate model drastically, and power was of more concern in this study than type I error.23 We used SAS software (SAS Institute, Cary, NC) to perform all statistical analyses.
Results
Of the 221 misdemeanor defendants referred for treatment to restore competence to stand trial, 152 (68.8%) were restored and 69 (31.2%) were not.
Demographic Characteristics
Table 1 lists the demographic characteristics of the misdemeanor defendants. No associations were found between demographic characteristics and restoration status with the exception of marital history. Being single (i.e., never married), was significantly associated with a nonrestored outcome.
Demographic Characterics
Clinical Characteristics
Table 2 describes the clinical characteristics of the study population. The two groups differed in the mean length of stay for the reference hospitalization. The restored defendants were hospitalized for 20.29 ± 12.52 days and the nonrestored defendants for 32.14 ± 20.17 days (t = 5.334; p < .001). The restored group had a higher mean global assessment of functioning score, based on assessment by their discharging psychiatrists.
Clinical Characteristics
The two groups did not differ in the mean number of treatment episodes, the number of previous inpatient psychiatric admissions, the cumulative length of stay (for all inpatient psychiatric admissions), and whether they were linked with an outpatient psychiatric clinic before treatment. We did not have access to the insurance status for many of the defendants.
Ninety percent of the nonrestored defendants had a diagnosis of a psychotic disorder, which was significantly higher than the proportion of restored defendants with that diagnosis (68%; χ2 = 12.588; p < .001). The group of restored defendants had a higher proportion with mood disorders than the group of nonrestored defendants (25% versus 6%, χ2 = 12.588; p < .001). The difference in proportion of each group with a diagnosis of an anxiety disorder was nearly significant (5% restored versus 0% nonrestored; χ2 = 3.414; p = .065). We did not find a statistically significant difference between the two groups in the proportion of defendants diagnosed with a substance use or cognitive disorder.
Although the nonrestored group had a higher proportion of defendants diagnosed with a psychotic disorder, more than 90 percent in both groups received an oral antipsychotic medication during the course of treatment. Both groups were similar in the proportions of defendants who received a long-acting injectable antipsychotic medication, a mood-stabilizing medication, an anxiolytic medication, or an anticholinergic medication. The difference in the proportion of defendants who received an antidepressant medication between the two groups almost reached significance.
Forensic Characteristics
Table 3 highlights the forensic characteristics of the misdemeanor defendants. There were no statistically significant differences between the two groups in the types of charges, the total number of charges, and whether the judge authorized involuntary treatment with medications. The difference in the mean number of previous restoration attempts between the two groups almost reached significance. For most defendants, this hospital admission was their first for restoration of competence to stand trial. Therefore, we cannot make inferences about differences in outcomes of previous restoration attempts.
Forensic Characteristics
Logistic Regression Analysis
The p values for the individual tests are shown in Tables 1, 2 and 3. After backward selection, the final model included single marital status (p = .012), length of stay (p < .001), and global assessment of functioning (p < .001). Single marital status was associated with a 34.5 percent increase in the odds of nonrestorability in this cohort. Further, for every day's increase in length of stay, the odds of nonrestorability increased by about 4 percent. Similarly, for every unit's increase in the global assessment of function rating, the odds of nonrestorability decreased by about 12 percent.
If the final model estimated a probability of restoration greater than 50 percent, then it predicted that the defendant was restored. Otherwise, the model predicted that the defendant was not restored. The final model was 87.7 percent concordant, meaning that the model was almost 88 percent correct in predicting the outcome using logistic discrimination.24,25
Discussion
Strengths of the Study
We were able to examine demographic, clinical, and forensic characteristics associated with restoration of competence to stand trial of misdemeanor defendants in a diverse patient population treated in a naturalistic setting. We examined the outcomes of a misdemeanor defendant population treated to restore competence to stand trial in an inpatient psychiatric facility staffed by academically oriented psychiatrists and trainees. To our knowledge, this is the first study to examine differences between restored and nonrestored misdemeanor defendants in multiple characteristics, including the proportion of forced-medication orders issued by the referring court.
Almost 70 percent of defendants regained competence to stand trial during the study period. When restorable, defendants regained competence in less than three weeks, on average, which informs current thinking in the field regarding time limits for restoration of competence to stand trial. Our multivariate analysis confirms results of a previous study examining characteristics associated with restoration of competence to stand trial.9
The results suggest that not all misdemeanor defendants are created equal. Both univariate and multivariate analyses suggested an association between marital status and restorability. Perhaps, marital status, and more specifically, the ability to maintain a long-term relationship, provides some indication of defendants' overall level of functioning before restoration attempts.17
Implications
Based on the results of this study, state and local policymakers may support further exploratory analyses in their jurisdictions to guide policymaking regarding time limits to determine restorability and to provide treatment to restore a defendant's competence to stand trial. We expect attention to refining time limits to have substantial implications for the allocation of mental health resources, particularly in areas where such resources are limited. Although it is costly to treat misdemeanor defendants with previous failed attempts at restoration, with the purpose of restoring competence to stand trial, the court system faces the challenge of upholding the Dusky and Jackson rulings in a cost-efficient manner. States may design and use different interventions, such as mental health court, to treat defendants with less likelihood of achieving competence, with a goal of minimizing recidivism and improving functional status. For defendants who may have a greater likelihood of achieving restoration, states might consider outpatient treatment in their communities.4
Further, policymakers can more confidently balance protection of defendants' right to stand trial in a competent mental state with their right to due process by examining current length of stay in their jurisdictions when developing policies to establish time limits for assessing restorability and for providing treatment to restore competence to stand trial. Based on the results of this study, perhaps the treating facility might provide an earlier report to the court about the defendant's progress in treatment and an assessment of the likelihood of achieving competence within a designated amount of time. The Sacramento County Superior Court currently requires such a report from the treating facility within 90 days of referral for treatment. Perhaps, the time limit for making such an assessment could be reduced significantly, thereby expediting the legal process while administering treatment more thoughtfully and cost efficiently.
Limitations
We examined, retrospectively, the naturalistic conditions under which treatment to restore competence to stand trial occurs in a specific setting. Different competence evaluators offered opinions to the court regarding defendants' competence to stand trial, and defendants were referred for treatment based on these assessments. Upon admission, different teams treated these defendants using a variety of interventions and treatment approaches. We reviewed the charts independently to collect clinical data. We met frequently and consulted within the team regarding coding of ambiguously documented clinical data, but we did not cross-verify coding of such data. Also, the treatment team did not refer many defendants for psychological testing and did not use formal competency testing for most defendants, so we could not make accurate inferences about differences in intellectual ability or performance on competency testing between the two groups. In general, retrospective review of data creates challenges in determining predictors of restorability, but such review offers insight that may be useful in informing state and local policy, nonetheless, as previously discussed.
Ideally, we would perform a prospective study with standardized procedures and interventions, including routine competency and intelligence testing, and such a study may be possible in the future. However, this approach offers unique challenges, particularly in satisfying institutional review board and ethics guidelines in protecting the rights of the incarcerated and mental health patient populations.
Conclusion
We need more research to compare outcomes of restoration in misdemeanor defendants in various treatment settings under different treatment conditions. We can examine the length of stay in other counties and states to inform policy regarding time limits, to assess restorability and to achieve restoration, if restoration is likely. Finally, we can explore more deeply the factors associated with nonrestorability to guide treatment interventions and state and local policy.
Acknowledgments
We thank Dawn Williams of the Sacramento County Department of Health and Human Services for her assistance with data collection and the University of California, Davis, Department of Psychiatry Research Track for their time support of this project. We also thank Debbie Wing, John Grozdanic, Wanda Feltus, and Bettijo Vela at the Sacramento County Treatment Center for extending access to the data.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2016 American Academy of Psychiatry and the Law





{kind=link}