


Abstract
In this study, we compared three groups of women admitted to a public forensic inpatient facility over the course of a two-year period. Detailed and systematic examination of social and psychiatric histories revealed that the group with the most persistent levels of aggression differed from the other two groups with respect to frequency of self-harming behavior, intellectual impairment, hypothyroidism, a childhood diagnosis of attention deficit-hyperactivity disorder (ADHD), and age of onset of psychiatric and behavioral symptoms. The high-aggression group also had the highest rate of childhood physical and sexual abuse, but the difference between that group and the two lower aggression groups did not achieve statistical significance. From the standpoint of childhood adversity, 94 percent of those in the high-aggression group had been placed outside of the original home by age 11. Eighty-nine percent were intellectually impaired. At admission, physical examinations revealed that 50 percent had a history of hypothyroidism and two-thirds were obese. Before admission, most had manifested severe aggression and emotional dysregulation, as evinced by high levels of self-harm, suicide attempts, and aggressive behavior in previous institutional settings that was both frequent and intense. Patients who share these characteristics are currently placed on a ward at the hospital with a milieu and individual therapy programs that are based on a dialectical behavior therapy approach that targets key symptoms of emotional and behavioral dysregulation.
Although a large body of empirical evidence supports the contention that, in general community settings, males are more likely to engage in aggressive behavior than females,1,–,3 data are equivocal regarding whether women are more or less aggressive than men when samples are limited to psychiatric institutions.4,–,6 However, there have been a few descriptive reports pointing to the existence of a subset of female patients who are among the most aggressive individuals (regardless of gender) at the facility being surveyed. For instance, in an early study, Ionno7 documented a high frequency of assaultive behavior reports on a 23-bed ward for severely impaired patients hospitalized at Hartford Hospital's Institute of Living and noted that a limited number of individuals (20–30% of the population) seemed to account for most of the aggressive incidents and that these patients were more likely to be female and to have severe personality disorders. In addition, Adshead8 described a sample of 16 women referred to a forensic psychiatry department in the United Kingdom, where chart reviews revealed that many had histories of violence and threats directed against hospital staff, childhood sexual abuse, self-harm, and diagnoses of borderline personality disorder and posttraumatic stress disorder (PTSD).
More recent empirically driven evidence of such a group of women was uncovered in a study of patients residing at a public forensic psychiatric facility that contained the only maximum and intermediate security forensic units in a state with a population of approximately 6 million. In that investigation, Beck et al.9 examined the seclusion and restraint records of 622 patients of both genders over a two-year period and, using a novel statistical approach to the data,10 found strong evidence of three discreet groups of patients with dramatically different trajectories of seclusion and restraint frequency (Fig. 1). The first of these groups (the low-aggression group, 71% of the sample) consisted of individuals who averaged less than 0.15 seclusion/restraint incidents per month over the course of their hospitalizations. Patients in the medium-aggression trajectory (22% of the sample) averaged approximately two incidents per month during the first two months of their hospitalizations, but rates declined to an average of about one incident per month by the end of the study period. Patients in the high-aggression trajectory group (7% of the sample) averaged six incidents per month during the first two months, followed by a gradual decline, but still averaged two to three incidents per month by the end of the study period. It is noteworthy that most of the incidents that prompted seclusion/restraint involved violent behavior on the part of the patients; in fact, a survey of hospital incident and injury reports revealed that patients in the high-trajectory group were 30 times more likely to have caused an injury during their hospitalizations than patients in the low-trajectory group.9
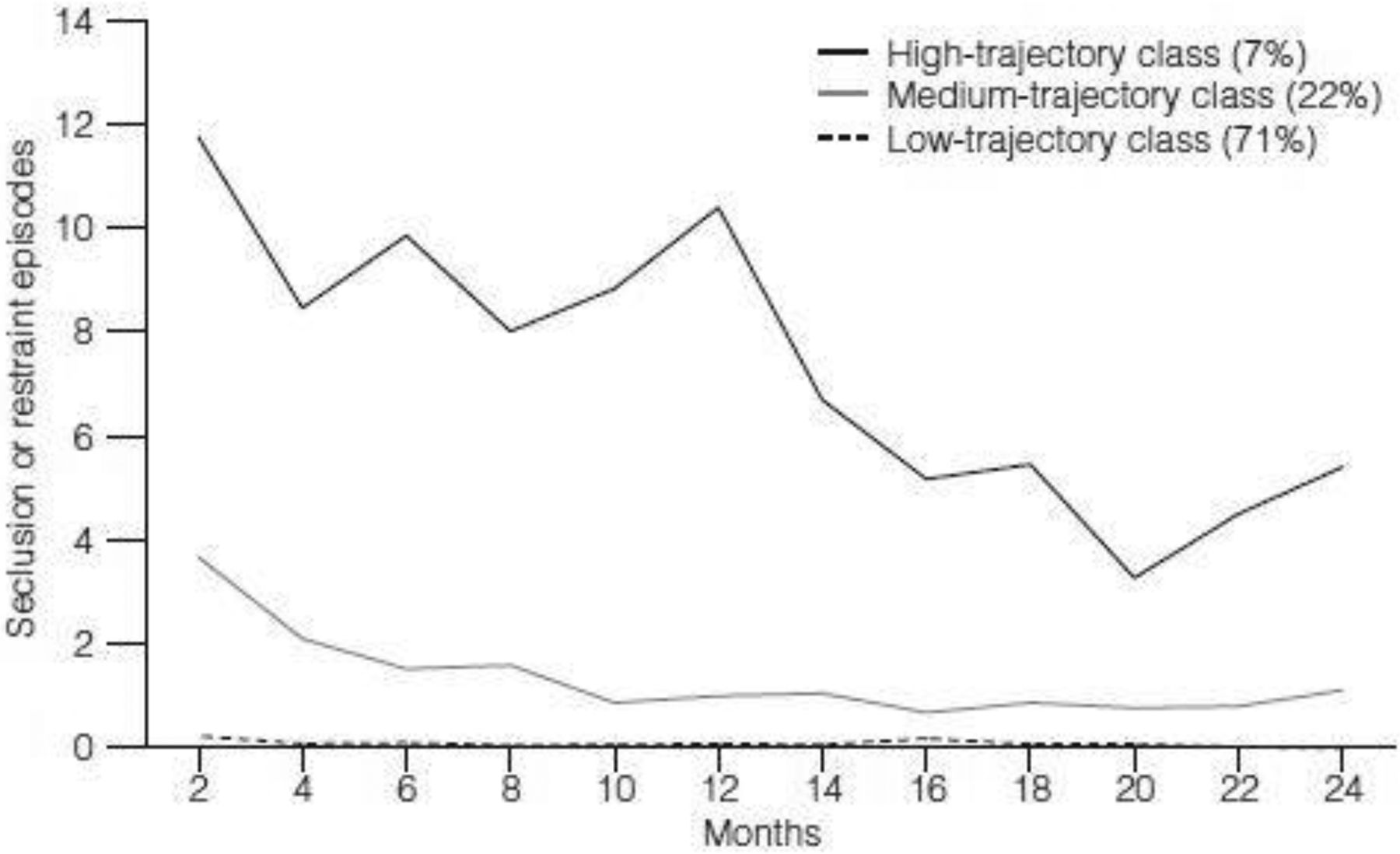
Latent class trajectories of frequency of seclusion of restraint episodes among 622 patients hospitalized at a psychiatric facility.
In a follow-up study, Hammer et al.11 compared the groups in Beck et al.9 with respect to gender and trauma history, making note of prior studies in the area that indicate that patients with histories of trauma are more likely to be secluded or restrained. When comparisons were made among the trajectory groups, which included patients of both genders, significant differences were noted between the groups' physical and sexual abuse rates, with the high-aggression group having significantly higher rates of both sexual and physical abuse than either of the other two groups. However, when patients were separated by gender, differences between groups failed to achieve significance, although trends in the data for both genders pointed to higher rates in the high-trajectory group. Hammer et al. further reported that relatively dramatic and statistically significant differences emerged with respect to the proportion of males versus females in the groups. In terms of gender, 13.8 percent of the total sample was female, a rate consistent with that found in other forensic settings.4,7,8 However, an examination of the distribution of gender by trajectory group revealed marked differences; 11.5 and 12.3 percent of the low- and medium-trajectory patients, respectively, were female, as compared with 43.9 percent of the high-trajectory patients.
Following the publications of Beck et al.9 and Hammer et al.,11 two members of the investigative team (N.C.B., J.H.) undertook an exhaustive review of the admission notes and social histories of the 18 females who were members of the highest trajectory group. When social histories were reviewed for the presence of physical or sexual abuse in childhood or adolescence, virtually all of the patients had reported abuse of some kind and, in many cases, the intensity of abuse was severe and long-lasting. Typically, abuse first occurred at the hands of biological parents who themselves were psychiatrically impaired, followed by placements in multiple foster homes and residential care facilities, where abusive experiences oftentimes continued.
Preadolescence in these patients was marked by the onset of aggressive and self-destructive behavior that accelerated throughout the teenage years. Many patients had been admitted (some repeatedly) to psychiatric institutions, at least briefly, by adolescence or early adulthood. Their institutional conduct was marked by a combination of aggressive behavior toward staff and other patients (in many cases involving injuries that required medical treatment, hospitalization, and lost days from work), elopement attempts, the need for frequent employment of seclusion/restraint and property destruction, as well as suicide attempts and self-harming behaviors. By early adulthood, most patients were transferred to forensic psychiatric settings, where they were placed on maximum- or medium-security wards somewhat better suited to managing their behavior.
Few patients had extensive histories of arrests or patently antisocial behavior or psychopathic personality characteristics. Instead, most evinced patterns of aggressive behavior characterized by impulsivity that seemed to be associated with interpersonal strife that generated various degrees of affective dysregulation. The group had primary Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV),12 diagnoses ranging from schizoaffective disorder to intermittent explosive disorder.
Examination of admission physicals of the patients indicated a high incidence of medical illness in childhood or early adulthood, including asthma and hypothyroidism. Many of the patients were morbidly obese. A final characteristic of patients in this group worthy of mention was a high rate of intellectual impairment. Many patients had been placed in special education classes by the time they were in middle school, and most carried diagnoses involving borderline intellectual functioning or mild intellectual disability.
In summary, historical data gained from a variety of information sources revealed that virtually all high-trajectory females manifested patterns of behavior characterized by intellectual impairment and severe and persistent behavioral and affective dysregulation, against the backdrop of chaotic early- and middle-school environments that included parental mental illness, severe physical or sexual abuse or both, neglect, and multiple foster home and residential care placements.
The study reported herein represents an attempt to confirm the a priori hypotheses derived from the records review described above. Specifically, we hypothesized that high-aggression trajectory female patients would have significantly higher rates of intellectual impairment; childhood sexual and physical abuse; hypothyroidism and obesity; early-onset behavioral problems and placements outside the home; and dysregulated aggressive and self-harming behaviors during previous hospital admissions than would women in the medium- and low-trajectory groups.
Method
This project was reviewed and approved by the University of Missouri Health Sciences Center Institutional Review Board as an exempt review of de-identified medical records, with a waiver of consent.
Checklist
Based on a series of discussions after their chart review of the high-aggression trajectory patients, two of the authors (N.C.B., J.H.) drafted a brief checklist (available on request) that measured variables thought to be characteristic of this patient group (intellectual impairment, childhood physical and sexual abuse, obesity and hypothyroidism, early behavior problem onset, and history of aggressive and self-harming behavior).
Given the preliminary and exploratory nature of the study and variations in terminology associated with clinical record keeping, alternate and somewhat overlapping checklist items were developed to address some of these patient characteristics. For example, in the clinical record, cognitive impairment was sometimes indicated via terms such as “intellectual disability” or “borderline intellectual functioning” and at other times could be implied from the fact that a patient had received “special education” services.
Subjects
The sample in this study consisted of 86 women hospitalized on forensic psychiatric units at a large Midwestern state psychiatric facility. These individuals represented all persons of the female gender included in a sample of 622 patients assembled by Beck el al.9 The mean age of the female patients in the sample was 33.5 (SD 10.46) years. Racially, 30.2 percent were black, 67.4 percent were white, and 2.3 percent were Latina. The average educational level was 11.0 (SD 2.37) years. In all, there were 51 patients in the low-aggression trajectory group, 17 in the medium-aggression trajectory group, and 18 in the high-aggression trajectory group.
Procedure
Admission physical examinations, psychiatric admission notes, and social work admission and assessment reports were coded according to the checklist. Items on the checklist addressed each of the a priori hypotheses generated by the authors' record review. Three undergraduate research assistants who were blind to the patients' trajectory classifications performed the chart reviews. Approximately 10 percent of the records were overlapped and rated independently by the assistants. Inter-rater agreement averaged 90 percent across rater pairings. Differences among the three groups were assessed via a series of Kruskal-Wallis nonparametric analysis of variance tests. We used follow-up Mann-Whitney U tests for a priori planned comparisons of mean ranks and a Bonferroni-adjusted significance level for post hoc unplanned comparisons of mean ranks.
Results
Group Demographic Characteristics
The three groups were compared with respect to demographic characteristics (age, race, educational level, and employment history). A Kruskal-Wallis test (p = .02) with follow-up Mann-Whitney U tests of the data revealed that medium-aggression group subjects had significantly less education than those in the high-aggression group (p = .01). The same statistical procedure (p = .001) revealed that the high- and medium-aggression groups (p < .001 and .03, respectively) had lower employment rates than in the low-aggression group, but the medium- and high-aggression groups did not differ (p = .22).
A Priori Hypotheses
Intellectual Impairment
Two checklist items assessed the hypothesis with respect to intellectual impairment (Table 1). The first was a dichotomous categorical item regarding any indication in the medical record that the individual had received special education or intellectual disability/developmental services. A Kruskal-Wallis test of this variable was significant (p < .001), with 89 percent of the patients in the high-trajectory group scoring present on this variable, compared with 41 percent of patients in the medium-trajectory group and 22 percent of those in the low-trajectory group. Follow-up Mann-Whitney U tests revealed that the high-trajectory group rate differed significantly from the rates of the medium- and low-trajectory groups (p = .003 and < .001, respectively). The rates of the two lower aggression groups did not differ significantly (p = .115). A second item was coded as any mention of impaired cognitive/intellectual capacity (present/absent). A Kruskal-Wallis test of this variable was also significant (p = .002), with rates of 72, 47, and 25 percent of cognitive impairment in the high-, medium-, and low-trajectory groups, respectively. Follow-up tests indicated that the high-aggression group rate differed significantly from that of the low-aggression group (p < .001), but that the medium-aggression group rate did not differ significantly from the high- and low-aggression (p = .134 and .098, respectively) group rates.
Trajectory Class Comparisons
Physical or Sexual Abuse in Childhood and Adolescence
Three items were used to assess this hypothesis. The first item was coded categorically (present/absent) and was scored such that if either physical or sexual abuse was mentioned, the item was coded present. If both were present, then this item was also coded present. If neither physical nor sexual abuse was noted, the item was scored absent. A Kruskal-Wallis test of this variable failed to achieve significance (p = .142), although the rates of physical or sexual abuse were in the predicted direction, with rates of 89, 67, and 67 percent in the high-, medium-, and low-trajectory groups, respectively. The remaining two items were scored on a four-point Likert format. One of these items assessed the frequency of sexual abuse and the second assessed the frequency of physical abuse. Neither of the Kruskal-Wallis results achieved statistical significance (p > .313), although differences were again in the predicted direction, with the high-trajectory group receiving the highest mean frequency ratings of all three groups.
Hypothyroidism and Obesity
This hypothesis was assessed by computing body mass index (BMI) data for each subject, based on the height and weight recorded at admission. The result of a Kruskal-Wallis test of this variable was significant (p = .005). Mean BMIs were 36.79, 40.21, and 31.86 for the high-, medium-, and low-aggression group, respectively. Post hoc tests revealed that the medium-aggression group's BMI differed significantly from that of the low-aggression group (p = .001), but that the high-aggression group did not differ significantly from either the low- or medium-aggression groups (p > .084). Hypothyroidism was assessed with a dichotomous (present/absent) item reflecting any indication, past or present, of hypothyroidism in the medical record. The result of the Kruskal-Wallis test of this variable was significant (p = .043), with hypothyroidism rates of 50, 24, and 20 percent in the high-, medium-, and low-aggression groups, respectively. Post hoc comparisons revealed that the rate encountered in the high-aggression group differed significantly from that in the low-aggression group (p = .014), but that the medium group did not differ significantly from either of the other two groups (p > .110).
Early Onset of Psychiatric/Behavioral Symptoms and Multiple Placements
Two variables were used to evaluate this hypothesis: the first involved recording age at first mention of psychiatric symptoms. The Kruskal-Wallis test result for this variable was significant (p < .001). In the high-aggression group, the average age of onset was 12 years, as compared with 16 and 22 years of age in the medium- and low-aggression groups, respectively. Both the high- and medium-aggression groups (p < .001 and .021, respectively) differed significantly from the low-aggression group on this variable, but these two groups did not differ significantly (p = .060). A second item assessing this hypothesis was coded categorically and related to the presence or absence of placements outside the home (foster homes, detention centers, group homes, and residential care facilities) at or before age 11. The result of the Kruskal-Wallis test of this variable was also significant (p = .003), with 94 percent of high-aggression group subjects experiencing placements at or before age 11 versus 59 and 49 percent in the medium- and low-aggression groups, respectively. Post hoc comparisons revealed that the rate in the high-aggression group differed significantly from that in the medium- and low-aggression groups, respectively (p = .013 and .001, respectively), but that the medium- and low-aggression group rates did not differ significantly (p = .487).
Aggressive and Self-Harming Behaviors
Five items were used to assess this hypothesis, including items related to self-injury attempts, suicide attempts, elopement attempts, and aggressive behavior observed in institutional settings before admission.
Self-injury attempts and completions were measured on a six-point Likert scale, with higher ratings reflecting greater frequency of self-injurious behavior (0, never; 3, five to six times; 5, ten or more times). The Kruskal-Wallis result for this item was significant (p < .001). Mean scores were 2.56, 0.94, and 0.43 for the high-, medium-, and low-aggression groups, respectively. Post hoc testing revealed that the high-aggression group mean differed significantly from the medium and low group means (p = .005 and < .001, respectively), and that the medium- and low-aggression group means did not differ significantly (p = .193).
Suicide attempts were also measured on a six-point Likert scale, with higher ratings reflecting higher frequency of suicide attempts (0, never; 3, five to six attempts; 5, ten or more attempts). The result of a Kruskal-Wallis test of this variable failed to achieve significance (p = .090), although the frequencies of suicide attempts were in the predicted direction, with means of 1.67, 1.12, and 0.90 for the high-, medium-, and low-aggression groups, respectively.
An item measuring elopement attempts, scored present or absent and subjected to a Kruskal-Wallis test, was significant (p = .019), with rates of 61, 71, and 35 percent in the high-, medium-, and low-aggression groups, respectively. Post hoc comparisons revealed that rates in the medium-aggression group were significantly higher than in the low-aggression group (p = .012), but that the high-aggression group did not differ significantly from either of the other two classifications (p > .058).
Frequency of aggressive behavior in prior institutional contexts was measured on a five-point Likert scale. The Kruskal-Wallis result for this item was significant (p < .001) with group means of 4.56, 3.47, and 1.90 for the high-, medium-, and low-aggression groups, respectively. The Likert anchors on this scale were 1, never; 3, occasionally; and 5, frequently. Post hoc tests revealed that both the high- and medium-aggression groups (p < .001 and .002, respectively) differed significantly from the low-aggression group, but not from each other (p = .104). A second item also measured prior aggression with a Likert format, but on this item, higher values reflected the seriousness of the aggression (1, no treatable injuries; 3, outpatient treatment; and 5, hospitalization required). The Kruskal-Wallis result for this item was also significant (p < .001), with mean values of 2.50, 1.29, and 0.37 for the high-, medium-, and low-aggression groups respectively. Post hoc tests revealed that both the high- and medium-aggression groups (p < .001 and = .003) groups differed significantly from the low-aggression group, and that the high-aggression group mean differed significantly from the medium-aggression group mean, as well (p = .011).
Other Variables
Several other variables were included on the checklist, but a priori hypotheses were not developed for them, because we believed that they did not bear directly on the core symptomatology of the high-trajectory patients. These results are also reported in Table 1. Because these items were essentially speculative and were not the subject of specific directional a priori hypotheses, a Bonferroni-adjusted significance level was used for group contrasts.
A childhood diagnosis of attention deficit disorder was assessed according to a dichotomous (present/absent) variable. The result of a Kruskal-Wallis test of this item was significant (p < .001), with rates of 44, 0, and 6 percent in the high-, medium-, and low-aggression groups, respectively. Post hoc tests revealed that the high-aggression group rate differed significantly from both the medium- and low-aggression group rates (p = .002 and lt] .001, respectively), and that medium- and low-trajectory group rates did not differ significantly from each other (p = .310).
School behavior problems were assessed with a dichotomous (present/absent) item reflecting any aggressive or disruptive behavior in a school setting reported in the medical record. The Kruskal-Wallis result for this item was significant (p < .001), with rates of 44, 53, and 10 percent in the high-, medium-, and low-aggression groups, respectively. The high- and medium-aggression groups differed significantly (both p < .001) from the low-aggression group on this variable, but the two groups did not differ significantly (p = .620).
Discussion
The results of this study provide confirmation of many of the hypotheses generated by the clinical review of patient medical records. From the standpoint of childhood adversity, almost 90 percent of patients in the high-aggression trajectory group experienced some sort of sexual or physical abuse and 94 percent had been placed outside of the home at least temporarily by age 11; by age 12, most had experienced the onset of psychiatric symptoms. These findings suggest that many of these patients grew up in early-childhood environmental conditions that were extraordinarily toxic.
Certainly, results of the oft-cited Adverse Childhood Experiences (ACE) study portend that such high levels of childhood trauma may be associated with a wide range of adverse outcomes later in life, including aggressive and antisocial behavior.13,14 Although the current investigators were not in a position to assess the wide spectrum of maladaptive behaviors and adverse health outcomes addressed by the ACE investigation, it is noteworthy that there were high rates of suicide attempts and obesity in the sample, although these did not always differ significantly when comparisons were made across groups.
From a diagnostic and symptomatic standpoint, 89 percent of patients with a high-aggression trajectory manifested intellectual impairment. By the time of admission to a forensic psychiatric facility, which occurred at a mean age of 27, physical examinations revealed that 50 percent had a history of hypothyroidism and two-thirds were obese. From a behavioral standpoint, before admission, most had manifested severe aggression and emotional dysregulation, as evinced by the high levels of self-harm, suicide attempts, and aggressive behavior in previous institutional settings that was both frequent and intense.
After admission, patients in the high-aggression trajectory group continued frequently and persistently to engage in aggressive and self-harming behaviors at rates far in excess of patients in the other two trajectories, with resultant higher rates of incident and injury reports, including substantial physical injuries to staff and other patients, a number of which resulted in significant medical interventions, disability claims, and institutional costs.9,15
Across the three trajectory groups, planned comparisons involving many of the variables noted herein demonstrated that the high-aggression trajectory group had higher frequencies of these characteristics and behaviors. In some cases, the high-trajectory group differed significantly from both of the other groups, and, in others, the high-trajectory group differed significantly from the low-trajectory one, with the medium-trajectory group falling into an intermediate range.
Several variables are noteworthy for their failure to achieve statistical significance, most notably those related to physical and sexual abuse and obesity. A variety of factors suggest themselves as potential explanations for these findings. First, base rates of these characteristics across all three groups was very high; for instance, although the rate of physical and sexual abuse in the high-aggression trajectory group was 89 percent, almost two-thirds of the patients in the other two groups had also been abused. With regard to the failure to find significant differences among trajectories with regard to BMI, it is possible that medication played a confounding role, as some of the psychoactive drugs prescribed in psychiatric treatment settings carry substantial risk of metabolic symptoms and weight gain.16
The high degree of homogeneity within patients with a high-aggression trajectory with regard to the above-mentioned constellation of salient historical, behavioral, and physical characteristics suggests the possibility that they had a previously unrecognized syndrome characterized by cognitive impairment, chronic and severe aggressivity, and self-harm. Although speculative at this point, a potentially relevant body of empirical evidence with regard to this factor is the literature on childhood adversity and aggressive behavior. More specifically, several studies have documented an interaction between childhood adversity and polymorphisms of genes affecting neurotransmitters that appear to produce various degrees of risk for future aggression.17,18
Candidate genes in this regard include a variable number of tandem repeat polymorphisms affecting monoamine oxidase-A (MAO-A) production on the X-chromosome,17 a 44-bp insertion/deletion polymorphism on chromosome 17 that has an impact on serotonin metabolism (5HTTLPR;5- human serotonin transporter gene linked polymorphism), and the valine/methionine (Val/Met) substitution polymorphism on chromosome 22, thought to affect dopamine metabolism (COMT; catechol-O-methyltransferase).18 It is worth mentioning that recent developments in the technology of genotyping that have enabled genome-wide association studies may ultimately be more fruitful than the candidate gene approach, as there is some evidence that the latter method may have generated false-positive associations.19
From the standpoint of possible environmental mediators of a gene/environment interaction, one particularly fruitful line of approach may lie within the substantial body of literature pertaining to attachment theory and aggressive behavior (reviewed in Ref. 20).
Conclusions
In closing, it is noteworthy that the clinical management of patients with high rates of aggression and self-harm has undergone significant evolution at our hospital over the years, and there is some evidence to indicate that parallel changes are occurring elsewhere.21 Until recently, before the high degree of homogeneity in the problems surrounding their behavioral management was fully recognized, these patients were essentially scattered throughout the hospital, oftentimes on wards with patients manifesting diverse forms of pathology. Over the past decade, however, a specialized therapeutic milieu program (New Outlook) has been developed that addresses core therapeutic factors related to emotional dysregulation in a dialectical behavior therapy model.22 Certainly, the results of this study and the prior findings of Beck et al.9 have helped staff to recognize newly admitted patients with the aforementioned characteristics and to move them onto treatment wards that use the New Outlook treatment paradigm. However, it should be acknowledged that, although this approach has some advantages from the standpoint of staffing a discrete number of units with individuals who have received specialized training in the management of patients with chronic behavioral and emotional dysregulation, arguments can be made that placing a large number of chronically dysregulated patients on the same ward may lead to the development of ward atmospherics that facilitate the contagion of violent and self-harm behaviors.22 However, recent adaptations in the New Outlook program provide for a variety of contingencies when a contagion effect seems evident, such as taking vulnerable patients to quieter areas and engaging them in alternate activities, thus reducing the impact of adverse ward atmospherics.
Related work at our facility has focused on another facet of dealing with chronically and persistently aggressive individuals: namely, staff behavior and interactional patterns that may, at least partially, drive a cyclical process involving patient aggression, followed by the application of seclusion and restraint, followed by further aggression.15 In at least some cases, application of this approach has led to reductions in the use of seclusion and restraint, although many challenges remain in the long-term management of these patients.22
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2017 American Academy of Psychiatry and the Law





{kind=link}