


Abstract
The projected expansion of the nation's elderly population necessitates the revision of health care and policy strategies for safeguarding the health and assets of this community. The elderly are at greatly increased risk for developing mild cognitive impairment and Alzheimer's disease. These conditions are associated with diminished complex decision-making abilities that adversely affect patients, their families, and society, even during early stages of Alzheimer's disease. We present three composite patient histories that demonstrate problems routinely encountered by families, health care providers, and legal professionals during the course of early AD and MCI. We review the prevalence of cognitive and behavioral symptoms associated with MCI and early AD. Obstacles to early detection of cognitive decline, limitations of current testing modalities and benefits of earlier detection are discussed. Central themes common to medical and judicial approaches toward capacity assessment are discussed. We argue that an emphasis on earlier detection will result in benefits for patient health and result in financial savings to patients and the country as a whole. Finally, we recommend national guidelines for the evaluation of task-specific decision-making capacities to reduce the variability of outcome and improve quality of evaluations found among medical professionals, forensic evaluators, and legal actors.
The right to make decisions governing our lives, property, and assets is a central tenet of American society. When decision-making abilities begin to decline in association with age or illness, families and clinicians may hesitate to recognize the change and take the necessary steps, ones that would inevitably compromise certain rights.1 As advances in medicine, nutrition, and hygiene increasingly prolong the human life span, we face a new social dilemma: how do we effectively care for the increasing number of elderly, whom we expect will now live to experience a host of neurodegenerative conditions that are associated with behavioral changes and impaired decision-making?
In 2013, there were an estimated 44.7 million persons over the age of 65 living in the United States.2 By 2050, this figure is expected to increase to 83.7 million.3 The United States is not alone in experiencing this monumental demographic shift. Persons over the age of 60 are expected to constitute 21 percent of the global population by 2050.4 This demographic shift is anticipated to affect social welfare programs, as these programs were first created when life expectancies and worker-to-beneficiary ratios were very different. In 1935, when the U.S. Government established the Social Security program, the age of eligibility for old age benefits was 65, and many citizens did not live long enough to receive benefits based on life expectancy at that time.5 Of those who did, men lived 12 years and women 14 years in retirement. For the year 1940, it was projected that 46 percent of males and 39 percent of females living to age 21 would die before age 65. In 1990, the percentage of those deceased before age 65 was reduced to 28 and 16 percent, respectively. Therefore, of those persons living to age 65 in 1990, men were expected to live 15 years and women 20 years in retirement. This amounts to an increase of 25 percent for men and 43 percent for women.
Many Americans are now living to an age that makes them increasingly vulnerable to both decision-making impairments and behavioral changes caused by dementing illnesses. The most common of the dementing illnesses affecting persons over the age 60 is Alzheimer's disease (AD). AD is currently estimated to affect 5.3 million people in the United States and is predicted to affect 11 to 16 million people by 2050.6 AD is preceded by a period of subtle cognitive decline termed mild cognitive impairment (MCI), which may endure for months to years, and may be poorly recognized by family and clinicians because of the relative preservation of function in some areas.
Research on AD and MCI has largely focused on the study of cognitive decline. A growing body of data, however, shows that associated behavioral and neuropsychiatric symptoms, such as apathy or anxiety, are of equal importance when assessing the patients' and their families' quality of life. Subtle behavioral and cognitive changes often occur in AD and may occur in MCI, years in advance of the clinical diagnoses.7 These changes may impair complex decision-making, with significant medical, financial, and legal ramifications. Health care providers, families, financial planners, and legal professionals may erroneously conclude that a person's judgment is intact, based on casual conversation or adequate performance on basic cognitive tasks. We review recent research demonstrating a high prevalence of comorbid behavioral symptoms in MCI and early AD, outline the impact of these symptoms on complex decision-making, and discuss the consequent dilemmas faced by health care providers, patients, families, and communities. We focus on MCI and early AD in this analysis, but it is important to note that the topics discussed are also relevant to the care of persons with other dementing illnesses and medical conditions that alter behavior, including vascular dementia, frontal temporal dementia, Huntington's disease, traumatic brain injury, and HIV encephalopathy.
Of note, although the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) has recently established new terminology for cognitive disorders, we will be using pre-DSM-5 diagnostic labels in this manuscript in accordance with their predominance in the research cited in this analysis and their greater familiarity to readers.8 The DSM-5 replaced the terms “mild cognitive impairment” and “dementia” with “minor neurocognitive disorder” and “major neurocognitive disorder,” respectively. These broader labels include cognitive disorders that are acquired and nondevelopmental, but represent a decline from baseline (such as cognitive impairment following traumatic brain injury). The equivalent DSM-5 diagnostic labels for the disorders we discuss in this article are as follows: MCI is equivalent to the DSM-5 diagnosis of mild neurocognitive disorder (NCD); mild, moderate and severe dementia are equivalent to the DSM-5 diagnoses of mild major NCD, moderate major NCD, and severe major NCD. Etiologies or pathologies of cognitive disorders are listed as specifiers under DSM-5. For example, Alzheimer's dementia that is moderate in severity would be equivalent to the DSM-5 diagnosis of moderate major NCD due to Alzheimer's disease.
The three vignettes that follow are designed to raise the challenging questions that face caregivers and professionals who encounter impairments in decision-making capacity. These cases are fictionalized composites that raise common dilemmas and are not actual cases. The vignettes will illustrate opportunities for early detection of behavioral abnormalities that often signal deficits in decision-making capacity and will anchor the discussion of revised evaluation guidelines. For forensic evaluators charged with evaluating transactional capacity, testamentary capacity, or vulnerability to fraud or undue influence, the ability to identify milder and sometimes occult impairments that are interfering with task-related competencies will enhance the quality of the evaluation process.
Neuropsychiatric Symptoms in Early AD and MCI
Vignette 1: Effects of AD and MCI on Family, Occupation, and Finances
J. D. was a 70-year-old married man with a history of hypercholesterolemia and hypertension and a family history of AD (mother diagnosed in her early 70s) who presented to primary care, at his wife's behest, for evaluation of four to five years of mild short-term memory difficulty and progressive irritability. He continued to run his own business but had been less attentive to details, resulting in several financial losses. He was less interested in starting new projects or initiating social interactions with his family and became less amenable to advice and guidance from others. His Mini Mental Status Examination (MMSE) score was 26, with points off for orientation, serial sevens, and recall. Six years earlier, his MMSE was 30. He endorsed occasional mild feelings of sadness, reported that he had no problems, and attended the appointment only after a year of “pestering” from his wife and children. He was referred to the psychiatry department for evaluation of possible depression because of irritability, apathy, and sadness. His memory did not improve despite treatment for depressive symptoms. J. D. was eventually diagnosed with amnestic MCI, and a year later with early AD. Two years later, he developed paranoid ideation that his wife and brother were conspiring to control his business. It became progressively more difficult for J. D.'s brother to keep him abreast of business decisions. Conflict ensued between J. D.'s brother and daughter about who should run the business and what percentage of ownership each should have. J. D. had not written a will. He had had a somewhat turbulent relationship with his brother throughout his life, but their relationship had never been as difficult as it had recently. J. D. wished to challenge his brother's ownership interest in the family business, despite having worked with him for most of 40 years. J. D. lived with his wife and eldest daughter and did not wish to see his doctors; he believed that he had no problems unusual for his age. He took his antihypertensives and lipid-control agents sporadically.
AD- and MCI-associated alterations in behavior and function adversely affect family relationships and occupational performance. Family distress, financial losses, a decline in the care of medical conditions and legal conflicts may result. These are recurrent themes during management of neurodegenerative dementing conditions. The subtle signs and symptoms of a neurodegenerative dementing illness may appear years before overt dementia. If these symptoms are recognized early, there is an opportunity to minimize suffering and financial loss. However, as demonstrated in the vignette, the earliest stages of AD may be difficult to diagnose or differentiate from nondegenerative conditions, such as depression, in a standard clinical encounter. For example, the Mini-Mental Status Exam, a commonly used brief cognitive screen for dementia in primary care settings, has been shown to have relatively poor sensitivity for early AD or MCI and is particularly weak at detecting early deficits in executive function.9,10 Other factors that may impede early diagnosis include the masking of deficits by compensatory behaviors,11 the subtlety of personality changes,12 and a relative preservation of the capacity to complete basic activities of daily living.12,13
Behavioral symptoms may herald the onset of AD and are present throughout the disease course. In the above vignette, the patient's early memory decline was accompanied by irritability and mild depression. One study of 100 autopsy-confirmed patients with AD found that 74 percent had neuropsychiatric symptoms at the time of initial evaluation, 51 percent experienced apathy; 36.8 percent demonstrated verbal aggression; 25 percent, hallucinations; 20 percent, delusions; 17 percent, physical aggression; and 6 percent, depressed mood.14 In another study of patients who were not taking psychotropic medication or cholinesterase inhibitors, apathy (74%) was identified as the most frequent symptom in early, probable AD and was suggested as an early diagnostic indicator. In addition, anxiety (48%), agitation (35%), irritability (32%), depression (29%), and delusions (16%) were noted, as were disinhibition (6%) and hallucinations (3%) (Fig. 1).15 Other early, but dramatic, lapses in behavior and judgment, such as giving large sums of money to telemarketers, may herald dementia.6
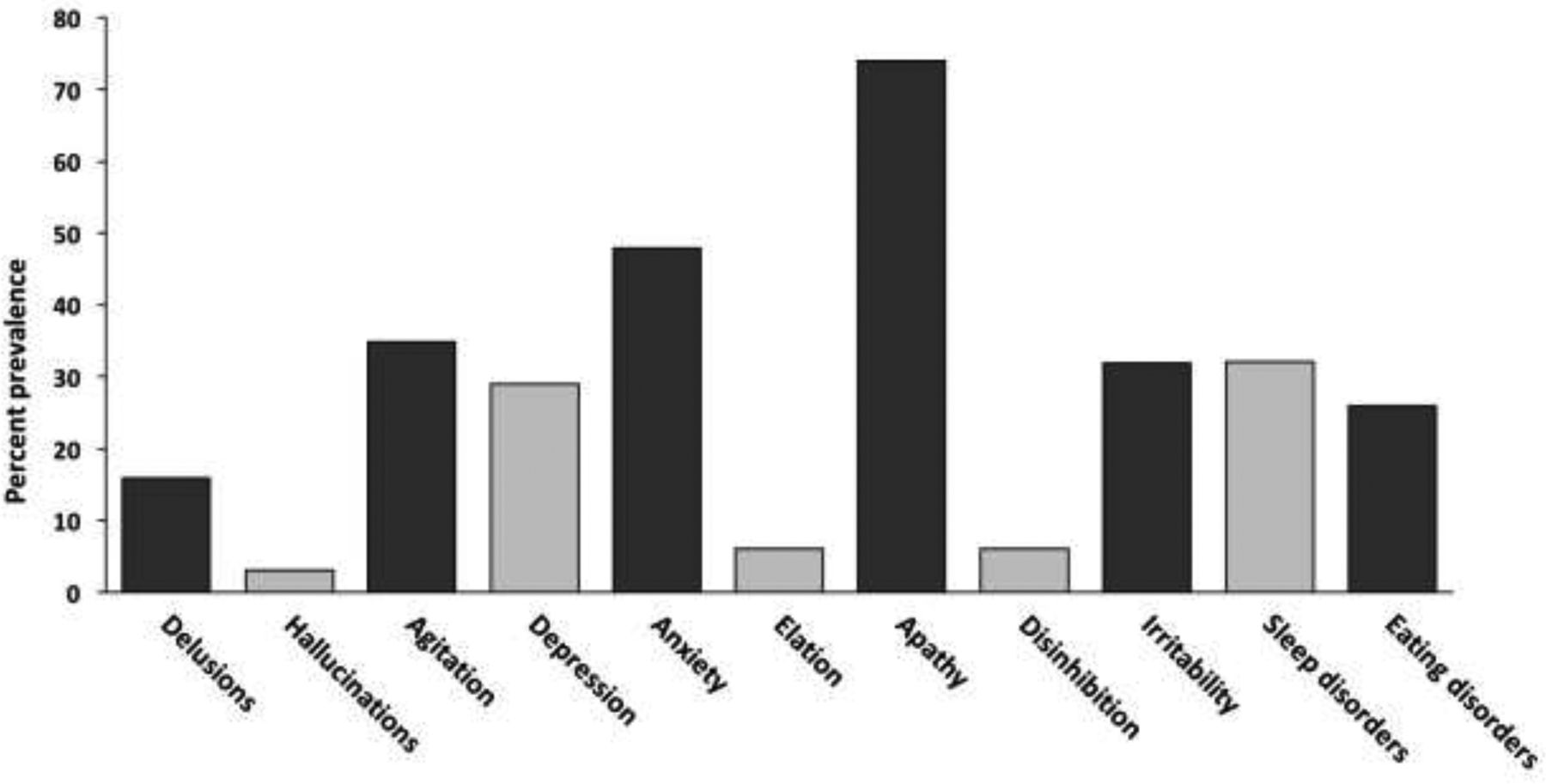
Neuropsychiatric symptoms in mild Alzheimer's disease. Adapted from Bruen PD, McGeown WJ, Shanks MF, Venneri A: Neuroanatomical correlates of neuropsychiatric symptoms in Alzheimer's disease. Brain 131:2455–63, 2008.15
Especially noteworthy is the high prevalence of apathy, which can be defined as a reduction in motivated behavior that is not directly attributable to a diminished level of consciousness, cognitive impairment, or emotional distress. Apathy is often manifested by decreased motivation, drive, and task persistence; diminished interest, initiation, and social engagement; increased passivity and withdrawal; and indifference to the environment. Apathy, coupled with impaired judgment and depression, may interfere with the completion of detailed financial tasks, reduce effective communication with family members and business associates, increase acquiescence to the decisions of others, and result in the neglect of one's health.
Functional changes may lag behind behavioral symptoms and subtle cognitive impairment. The most important and predictable early functional change in people developing dementia may be confusion and difficulty with money and finances, as was the case with J. D. in the vignette.16,–,18 The American Academy of Neurology's common warning signs for dementia include memory loss that affects job skills, difficulty performing familiar tasks, problems with language, disorientation in time and place, poor or decreased judgment, problems with abstract thinking, and misplacing things.19 Many of these changes are closely tied to mood and personality changes. Other subtle deficits in early AD may include blunted self-awareness, a lack of insight and concern,20,–,22 denial of illness, an overestimation of one's cognitive skills (such as visuospatial ability and memory),23 diminished appreciation of prosody,24 impaired recognition of facial expressions,25,–,28 and executive dysfunction (including reduced planning and foresight).29,–,32
Neuropsychiatric deficits increase with the advancing stages of the disease.33,–,36 One observational study noted a 90 percent prevalence of neuropsychiatric symptoms during the course of the disease; depressive symptoms, dysphoria, or major depression eventually occurred in approximately half of patients.14 Psychosis has been reported in 30 to 50 percent of patients at some time during the course of the illness, and more commonly in the later stages37 (Fig. 1). Other late-stage symptoms include anxiety, social withdrawal, agitation, reduced speech output, alteration of long-standing family relationships, and loss of humor.
Patients who manifest significant depression, anxiety, or aberrant motor behaviors have greater limitations in instrumental activities of daily living.38 These behavioral changes, which have no clear correlation with MMSE scores, have been shown to precipitate earlier nursing home placement and are linked to more rapid cognitive decline.39,–,42 Behavioral changes may alter family and peer relationships, leading to diminished contact and decreased monitoring of the affected individual. For example, a patient who develops irritability, social withdrawal, and depressive symptoms may be less apt to pursue routine medical treatment and follow-up for conditions responsive to therapy. Increased dependence on others may result in their coercive influence over patients' financial affairs or estate planning.
MCI is an intermediate state of cognitive function between normal aging and dementia, when objective cognitive difficulty is present without significant functional impairment. It is recognized as a potential prodromal phase for AD, with an annual risk for progression to frank AD of 12 to 15 percent in people aged 65 years or older.43,44 Almost half of MCI patients demonstrate neuropsychiatric symptoms coincident with the onset of cognitive impairment.45 Depression occurs in 20 percent, apathy in 15 percent, and irritability in 15 percent. Increased levels of agitation and aggression are also present. Impaired awareness of memory dysfunction may be present to a degree comparable with that found in persons with early AD. 36,46 Difficulties with medical decision-making have also been identified in this population.47 In summary, mood and behavioral symptoms are highly prevalent in MCI and early AD; may sometimes make diagnosis of dementia more difficult; and may have psychosocial, financial, and legal consequences for patients and their families.
Medical and Financial Decision-Making
Vignette 2: Medical Decision-Making
M. J. was a 69-year-old woman who had been experiencing mild, progressively worsening forgetfulness for four or five years. She had had mild paranoid ideation about the bad intentions of a neighbor whom she thought was watching her, but otherwise she had properly managed her social activities, finances, and home maintenance. She was driving much less often than she used to because she felt less comfortable driving. On a routine physical examination, her primary care doctor discovered a breast nodule that subsequently proved to be metastatic breast cancer. She was counseled that the best chance for successful treatment for this type of cancer would be surgery, radiation, and chemotherapy. She completed the 10th grade and had always been able to understand her primary care doctor's careful explanations of medical information. Now, M. J. had difficulty in remembering the details of the alternative medical treatments, as her doctor explained them to her. She forgot significant pieces of information and seemed mildly confused. She rejected treatment, believing that her doctors wanted her to undergo treatment because they need more patients for their research studies. M. J. had never manifested any distrust of her health care providers, and according to her daughter, this distrust seemed to reveal a change in her personality. Her oncologist was stymied. Her primary care physician felt that she was not behaving entirely rationally, but not to the extent that she lacked the capacity to make medical decisions. At her daughter's urging, M. J. consented to a neurological evaluation to exclude possible causes of cognitive and behavioral changes. The workup included laboratory studies, neuropsychological testing, and a brain MRI. Paraneoplastic processes were excluded. The neurologist concluded that M. J. had single-domain amnestic MCI.
As this vignette illustrates, subtle behavioral and cognitive changes may occur in MCI and AD, years in advance of the clinical diagnosis of dementia, frequently affecting multiple domains of decision-making, including decisions about health care. Studies indicate that the proportion of elderly with undetected impairments in medical decision-making may be large, and may go under-recognized. Raymont and colleagues48 surveyed 302 consecutively admitted medical inpatients and found that 40 percent appeared to lack the appropriate mental capacity for making medical decisions; these patients were older, were more likely to have cognitive impairment at the time of testing, were less likely to live independently, and had fewer years of education compared with those who maintained capacity. Family members and clinicians rarely recognized decision-making impairments in acutely ill hospital inpatients who appeared alert and had some ability to communicate.48
Similarly, in a community-based study, Fazel and colleagues49 assessed the competence of outpatients with dementia to complete advance medical directives compared with normal elderly controls. Of the latter group, 22 percent were deemed incompetent to complete the advance directives compared with 80 percent of the patients with dementia.
However, medical decision-making is one area in which legal and clinical standards for capacity are relatively well defined. For medical decision-making, the patient is required to give informed consent to, or refusal of, any treatment. The physician is required to explain a proposed intervention or treatment; disclose its rationale, risks, and benefits; and mention alternative treatments. To demonstrate capacity in this context, the patient must be able to communicate a decision to the medical provider, comprehend the relevant information, appreciate the situation and its consequences, and rationally manipulate information about treatment options.50,51 Despite these clear standards, there can be considerable interclinician variability in determinations of patient competence. When physicians in the subspecialities of geriatric psychiatry, geriatric medicine, and neurology conducted detailed bedside testing of persons with early AD for the purpose of determining competence to make informed medical decisions, the agreement rate was only 56 percent.52 Also, the most common forms of bedside mental status testing may reveal only minor abnormalities in persons with MCI and early AD, leading health care providers, family members, and legal authorities to erroneously conclude that the persons' judgment and complex medical decision-making capabilities are intact.47,53,–,55
Standards of competency vary across contexts and relevant state law. In addition, courts and clinicians draw an important distinction between global and task specific limitations on decision-making ability, preferring to limit a declaration of incompetence to the specific task undertaken. For example, a court may determine that a person's impairment is primarily in the domain of financial management and that other domains of personal decision-making are intact. This approach results in an evaluation of specific decision-making capacities on a case-by-case basis, with little predictive power.
In light of these varied and vague parameters for determining decision-making competence, many different medical and legal frameworks are used for evaluating competence for different activities. In practice, capacity evaluators disagree least often about patients' capacity to understand the matter at hand and most often about patients' appreciation of context and the quality of their reasoning.56 Evaluators often disagree on which dimensions of competence are important, the measurement of the individual dimensions of competence, and the thresholds for impairment. Important variables include differences in testing methods, the context-dependency of performance (especially when executive function is impaired), and fluctuations in performance (especially those related to medical illness or mood). Assessments will always be most difficult in crisis situations.
Vignette 3: Testamentary Capacity and Financial Decision-Making
K. O. was an 89-year-old man with mild-to-moderate AD. His wife, age 83, had probable early AD. K. O. managed most financial matters without conferring with his wife or children. He engaged in estate planning for the couple of years before his cognitive decline. The children were aware of their parents' plan to leave 10 percent of their assets to deserving charities that the parents had supported in the past. After K. O.'s death, the bulk of his estate passed outright to his widow. Under the influence of a charismatic leader of a charity and in the context of continued cognitive decline, his wife altered the charitable donations to comprise 60 percent of the estate. The children voiced concerns about their mother's mental state to her primary care physician of many years, who concluded, without a formal examination, that she lacked the capacity to make changes to her estate plan. Mrs. O., upset by this opinion, had her estate attorney engage a geriatric psychiatrist, who performed a brief evaluation that consisted of a 15-minute interview without psychometric testing. The psychiatrist offered the opinion that Mrs. O. retained the capacity necessary to change her estate plan. She executed a new will, with the assistance of her estate lawyer and the encouragement of the charitable organization. She also instructed her financial advisor to “cash out” of long-term investments to make her estate more liquid for eventual distribution, generating adverse tax consequences. This will withstood subsequent antemortem and probate legal challenges. The children, who feel that their mother's fragile testamentary capacity and vulnerability to undue influence are obvious, have been frustrated by their inability to protect their mother and their inheritance.
Testamentary capacity refers to the capacity to make or alter a valid will. According to the Uniform Probate Code in the United States, a person who makes a will must be aware of the individuals, such as children, who would be the natural beneficiaries of the will; understand the nature and extent of the property at stake; understand the disposition the will is making; and form an orderly plan for disposition of the property.57 Testamentary decisions made by MCI and early AD sufferers will have far-reaching consequences for individuals, society, and financial markets, as an estimated $59 trillion passes down from the estates of the U.S. elderly over the next 55 years.58 In addition to writing wills, this population will make complex financial decisions with far-reaching consequences.
Cognitive and behavioral impairments in the elderly, along with subsequent difficulties with decision-making, render them especially vulnerable to financial exploitation, a problem with enormous social and personal costs. Criminals have been among the first to seize upon opportunities created by the vulnerabilities of this population. More than 7.3 million Americans over 65 have been victims of financial fraud, according to a 2010 survey by the Investor Protection Trust, a nonprofit investor education group.59 Consumer Action, a national consumer advocacy group, reports that persons over the age of 60 constitute 15 percent of the population, but an estimated 30 percent of financial fraud victims.60 In state surveys of financial fraud and abuse, women and older seniors are more likely to be victimized, and dementia is a significant risk factor for this abuse. The National Center on Elder Abuse estimates that only 1 in 25 cases of financial exploitation is reported, suggesting that there may be 5 million financial-abuse victims each year.61 The Metropolitan Life Company estimated that older Americans lost at least $2.9 billion to financial fraud in 2010.62
Financial advisers may also regularly confront the question of their older clients' capacity to make financial decisions. In 2009, 350 investment advisers were surveyed by Fidelity Investments.63 They were asked whether they suspected that any of their clients had dementia and, if so, whether they had responded to the situation. Eighty-four percent felt that they had clients with symptoms of dementia; 96 percent stated they did not feel prepared to deal with those clients; and 50 percent acknowledged that they were not comfortable raising the subject of dementia. Many noted that their first duty was to protect their clients, that they were prohibited from disclosing information about their clients without their clients' permission, and that referral to clinicians for evaluation requires the clients' consent, which could be traumatic for clients and unsettling for the relationship. Expense was also cited as a deterrent.63 Recent evidence indicates that elderly victims of financial abuse are less likely to discuss their finances with a trusted individual, compared with those who do not become victims.64 State governments have been attempting to address these concerns through regulations that allow brokers to report financial abuse to authorities.65 The Financial Industry Regulatory Authority (FINRA) has also launched a phone helpline for seniors, enabling them to share their concerns with a neutral third party.66
Despite the growing magnitude of these concerns, courts have not yet developed a uniform approach toward assessment of elderly people's capacities to make financial and other decisions. Several scholars in this area have developed well-normed psychometric instruments designed to reveal and quantify impairments in financial decision-making67; however, they have not been widely used by forensic or other medical professionals.
Assessment Challenges
Across domains, assessments of capacity are beset with certain shared difficulties. The MMSE, the most common office-based test, is generally inadequate to assess complex capacities as it does not evaluate executive function, which plays a prominent role in most of the abilities discussed herein and it is relatively insensitive to mild cognitive impairment.17,47,68,–,70 The clinical variance of AD and MCI at onset, as well as the fluctuating intensity of deficits, is well known and can complicate assessments of capacity. As illustrated above, it is sometimes not clear what combination of cognitive and behavioral deficits are predictive of decision-making difficulties. Challenges to competence may escalate into legal disputes, but the capacity standards and legal frameworks governing assessments differ from task to task and state to state. These challenges to determination of capacity contribute to the variability of outcomes in both the doctor's office and the courtroom.
Diminished mental capacity is often situation specific. An individual who has diminished capacity in one decision-making realm may have the capacity to make another type of decision, depending on the complexities and on the risks and benefits associated with that decision. In its early stages, incapacity is rarely detected by clinicians or relatives, both of whom tend to overestimate abilities.48 Depending on their specialty or role, clinicians may not formally assess mental capacity at the bedside or may be reluctant to do so because of potential legal, ethics-related, and practical consequences. More generally, assessing mental capacity quickly, efficiently, and accurately can be difficult, particularly with more complex decisions or domains. Yes/no answers on screening tests are desirable, but clinical assessments often place patients on a continuum with varying strengths and weaknesses in reasoning and cognitive abilities, an approach clearly unsuited to the more subtle and variable deficits of those who have AD and MCI.
Future Research Directions
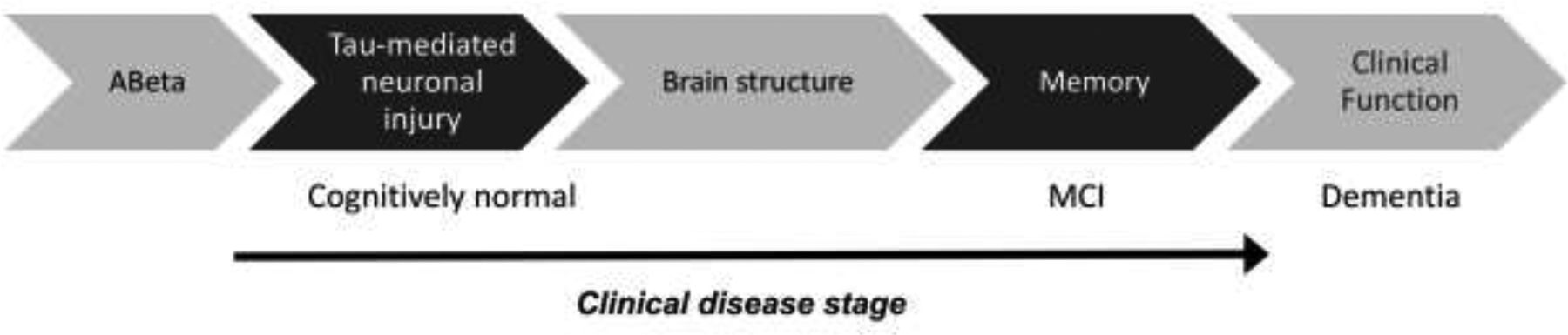
Recent advances in our understanding of the neurobiological substrate of AD have led to the development and refinement of neuroimaging and biological markers for early diagnosis.71 It is now known that AD neuropathology evolves over a long period in cognitively normal adults, causing cell death and neuronal dysfunction for years before the clinical syndrome begins to manifest (Fig. 2).72,73 Subtle abnormalities may be detectable in asymptomatic individuals nearly a decade before AD dementia is diagnosed.74

Progression of disease markers and their correlation with disease stage. MCI, mild cognitive impairment. This figure demonstrates a rough order of appearance of biomarkers, and their respective disease stage. In preclinical stages of illness, a person may be positive for disease biomarkers while being cognitively intact. Adapted from Jack CR Jr, Knopman DS, Jagust WJ, et al: Hypothetical model of dynamic biomarkers of the Alzheimer's pathological cascade. Lancet Neurol 9:119–28, 2010.88
Some means of early detection are in clinical use, such as markers for cerebrospinal fluid and fluorodeoxyglucose (FDG)-positron emission tomography (PET) scans, whereas others are undergoing further testing and development, such as amyloid imaging. Although these methods may diagnose dementia in patients years before symptom onset and allow them to plan for the future, early detection will present psychosocial, legal, and financial challenges for both individuals and society.
As we move toward earlier diagnosis, it becomes increasingly difficult to distinguish the process of AD and related disorders at their very earliest stages from the processes of normal aging. Concerned families are often left in limbo; they are unable to plan for the future, not knowing whether their loved ones have normal aging, MCI, AD, or something else. Because the pathophysiology of AD begins years before the clinical diagnosis of dementia and because disease-modifying therapies are likely to be most efficacious before the point of irreversible neuronal loss, the challenge is to discover biomarkers that, before symptoms appear, can accurately predict whether patients are developing AD or MCI. The signature biomarkers, independent of clinical diagnosis, such as reduced Aβ 1-42 and increased phospho-tau in the cerebrospinal fluid, may offer that promise.75 Early identification of AD patients through biomarkers may, in turn, prompt sweeping changes to current conceptual guidelines regarding AD.
In this context, three new stages of AD have been proposed, including preclinical disease, MCI, and late-stage dementia.7 If these guidelines were to be adopted, a two-to-threefold increase in the number of persons diagnosed with probable AD would be likely to ensue. The costs of such predictive testing would have considerable impact, and not only in financial terms. For example, such testing could have adverse psychological effects and compromise patients' ability to obtain long-term care insurance. These costs must be balanced against any potential benefits, including the current absence of therapy with proven effectiveness. The proposed new guidelines are largely intended to inform research rather than clinical assessment, but the expectation is that they may ultimately guide clinical diagnosis and management.76 It is hoped that the new guidelines and ongoing research will move the field forward, to allow the earliest intervention with disease-modifying therapeutics.
Earlier, more reliable detection of cognitive impairments in the elderly may also minimize costs, measured in time, resources, and dollars,77 thus providing important benefits for patients and society. Earlier detection and care management for people with newly diagnosed cognitive impairment and dementia may reduce outpatient medical costs substantially. The delay of onset and progression of AD for just one year would translate into nearly 9.2 million fewer cases by 2050, with potentially significant social, demographic, and financial implications.78 Earlier diagnosis may create a greater opportunity for a healthy emotional adjustment to the diagnosis on the part of the patients and their families, and allow for changes in health habits. Early diagnosis and accurate prognosis also allows for the arrangement of better social supports and the development of a more comprehensive medical care plan.
For forensic evaluators, as well as financial and probate professionals, the prospects of earlier and more specific detection of impairments points to two imperatives. The first is to refine and standardize capacity parameters across the medicolegal divide. These efforts are already well under way, with the production of task-specific instruments for the measurement of financial and medical decision-making.79 Although it is particularly difficult to detect or measure susceptibility to coercion as distinct from cognitive deficits, some recent work has focused on financial assessment models that take into account personal values and preferences, along with more standardized measures of cognitive impairment.80 In a large-scale research effort to breach the medicolegal divide, the American Bar Association, in concert with the American Psychological Association and The National College of Probate Judges, has produced a three-volume series of handbooks to review and standardize the appraisal of various capacities, including medical decision-making and financial and testamentary acumen. These provide a promising roadmap for the highest quality of legally and medically informed capacity assessment.81,–,83
The second imperative surrounding early detection of future cognitive decline is the development of strategies that encourage individuals to make early and binding expressions of intent and dispositions of assets. To the extent that early dispositions depend upon intact cognition and unfettered expression of choice, forensic evaluators may be engaged early in this process to “contest proof” these dispositions (Ref. 84, p 397). These include durable powers of attorney, living revocable trusts, living wills, antemortem probate, and other forms of advance directives.85
Finally, longer life spans will require more funding for the treatment of neurodegenerative diseases, more extensive accommodations for the disabled, and restructuring of retirement, insurance, and social security plans. By 2030, those who are 85 years old or older will constitute 19 million, or 21.6 percent, of the elderly population in the United States, representing the fastest growing population in the world. Many institutions will have to change as the elderly population expands. The challenges are daunting but necessary.
Conclusions
Adequate data are lacking regarding the specific effects of early neuropsychiatric changes in MCI and AD on domain-specific, complex decision-making. Clear and consistent, widely accepted instruments and guidelines are not always available to measure task-specific decision-making capacities in the context of MCI and early AD. Nor are there reliable instruments to measure this population's susceptibility to undue influence or coercion. The lack of such instruments and guidelines results in a spectrum of common medical, legal, and financial situations whose outcomes can vary greatly, often to the detriment of patients and their families. The above vignettes illustrate some of the areas in which further clarity, guidelines, regulations, and research would be helpful. Neuropsychiatric symptoms, such as paranoia or apathy, can complicate the diagnosis and psychosocial management of MCI or AD for both clinicians and caregivers, as in Vignette 1. Determination of capacity, even in relatively well-defined areas such as medical decision-making, can still become complex, especially in MCI or when patient preferences change. Finally, the ageing of the population will amplify the problem of financial exploitation of cognitively impaired individuals, as demonstrated in Vignette 3, and current regulations are still evolving to handle this reality.
Remarkable advances in neuroscience are transforming and challenging the current legal and financial policies and structures. As new neuropsychological instruments, biomarkers, and neuroimaging protocols emerge, perhaps leading to earlier diagnosis and treatment, it will be increasingly important to develop better guidelines and evidence-based methods that translate medical concepts into legal practice and financial management settings. The development of future health care policies is thus dependent on collaborations between modern neuroscience and the legal and financial professions.86,87
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2017 American Academy of Psychiatry and the Law
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵





{kind=link}
{kind=link}