


Abstract
Competency restoration in jails has grown steadily over the past decade, driven primarily by cost considerations and long wait times for inpatient restoration programs. Although jail-based programs may offer an attractive temporary solution to the shortage of beds, a longer-term solution involves enhancing the continuum of competency restoration services available outside of the correctional system. Such a continuum includes inpatient, supportive residential, and outpatient services. If these services were adequately funded and managed, jail-based competency restoration services would provide no additional benefit to patients, mental health professionals, or the criminal justice system.
In 2011, I wrote about jail-based competency restoration from a largely theoretical perspective,1 as at that time there were few data points about the practice to examine. Only a handful of jail restoration programs had been developed around the country, and they were too new to draw firm conclusions about their value. Even at that early stage, it was clear that jail restoration had the potential to save money. Many important questions, however, such as the efficacy of jail restoration compared with inpatient treatment and its feasibility on a large scale, had yet to be answered.
In the intervening years, jail restoration has steadily gained in popularity. Arizona has transferred the majority of its competency restoration services from the state hospital to jails, admitting an average of just 10 patients per year to the Arizona State Hospital for restoration between 2013 and 2017.2 Although accurate data about other states are hard to obtain, it appears that at least eight states have developed jail restoration services,3 and the pressure to do so has been mounting because of the shortage of inpatient restoration beds around the country.4 Some of these programs report remarkable success rates, such as a Virginia program that reported an 83 percent restoration rate and an average length of stay of just 77 days.5 Similarly, a Colorado program reported a 90 percent restoration rate in less than 90 days.3 Results from California were slightly less robust, with 55 percent of patients being restored to competency in an average of 57 days, but these results were achieved at less than a third of the cost of inpatient treatment.6
Despite these impressive results, some have been less optimistic about the prospects for jail-based restoration. For example, in Trueblood v. Washington,7 the plaintiffs cited numerous deficiencies in two jail restoration programs that had been implemented by the state as a solution to the shortage of inpatient beds, and in 2018 the state agreed to close the programs as part of the Trueblood settlement agreement.8 Felthous and Bloom9 have raised concerns about the capacity of jails to manage involuntary medications and the slow creep of mental health services from health care settings into correctional settings. Even the popular press has commented on the crisis of competency restoration, reporting on stories of patients languishing in jail while awaiting treatment and advocating for more outpatient services.10
In their new article,11 Ash and colleagues have essentially taken a middle ground, reporting on the success of their Georgia jail restoration program while acknowledging its limitations. Even under the near-ideal conditions that the authors were able to create for their program, including a dedicated housing unit in the jail, multidisciplinary staff, educational and therapeutic groups, psychological testing, round-the-clock assessment capacity, and the support of a university-based forensic psychiatry fellowship program, the rates of restoration in jail were substantially lower than in an inpatient setting (40% versus 85%). Patients did, however, benefit from beginning treatment in the jail-based program much more quickly, even before a formal finding of incompetence, and they were restored to health sooner than if they had waited for a hospital bed. After weighing the pros and cons of their program, Ash and colleagues concluded that a continuum of services is appropriate for competency restoration, including jail settings.
I find the conclusion by Ash et al.11 about a continuum of services for competency restoration entirely sensible; not every patient referred for restoration requires an inpatient level of care. I disagree, however, that such a continuum should include jail-based programs. My perspective is informed by my experience overseeing a state hospital–based competency restoration program in Connecticut, which some may perceive as a bias toward the status quo of inpatient treatment. I have also worked as a psychiatrist in a Connecticut jail and served as a consultant and court-appointed monitor of jail mental health services around the country, which has taught me much about the limitations of jail-based treatment, no matter how well funded or professionally managed. Because of these experiences, I now stand firmly against moving mental health services into the correctional system when viable community alternatives exist.
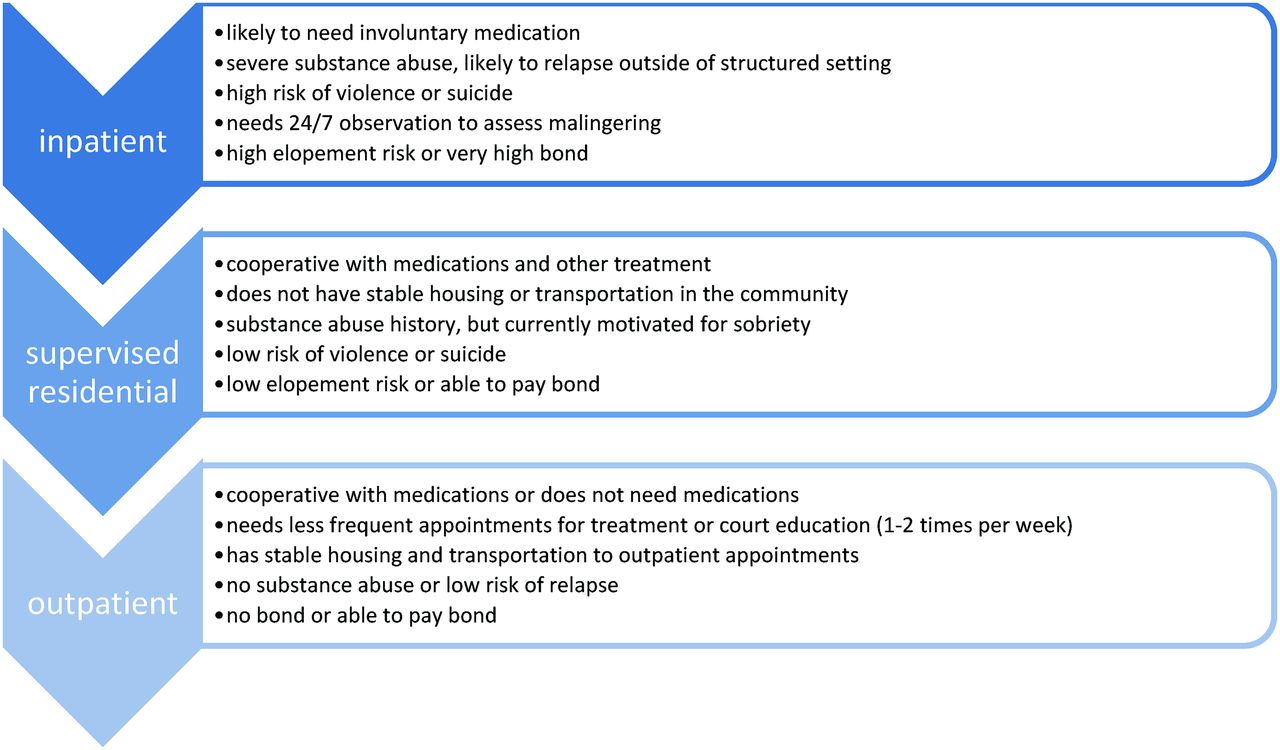
In my opinion, a finding of incompetence means that the individual is simply “too sick for jail,” and their criminal detention should be halted while they are restored to health. Therefore, instead of advocating for more jail-based competency restoration programs, I would develop a continuum of services that functions entirely outside of the correctional system and consists of different levels of care: inpatient treatment, supervised residential services, and outpatient treatment (Figure 1). These three levels of care are familiar to most mental health providers, so I do not describe their essential features here. Implementing them in the context of competency restoration would provide adequate flexibility to treat patients based on their treatment and risk-management needs. Figure 1 outlines characteristics of patients who would likely be appropriate for each level of care.

Competency restoration levels of care and characteristics of appropriate patients.
In a scheme where these three levels of care are readily available, a jail-based program provides little benefit, if any. Some may argue that jail-based restoration provides easier access and a quicker start to treatment once a patient has been determined to be incompetent, as in the program by Ash et al.11 In a well-resourced forensic mental health system, however, wait lists for inpatient or community-based programs would not exist. For example, in Connecticut, patients are admitted to inpatient or outpatient restoration services on the same day that they are found incompetent. In addition, when a competency evaluation is ordered by the court, some defendants have the option of voluntary admission to the state hospital even before the assessment takes place, which allows them to begin treatment immediately in the hope that they will be competent by the time of the formal evaluation. If such a scheme were widely implemented and hospital-based or community-based treatment programs were available, the early-intervention advantage of jail-based programs would be eliminated.
Some may also argue that keeping patients in jail for competency restoration provides greater continuity of care and potentially eliminates the cycle of repeated transfers from hospital or outpatient programs to jail. Technically, this is true; keeping people in jail for restoration does result in fewer transfers in and out of the jail. But in a jail-based restoration program that functions separately from the remainder of the jail's mental health services, as the program by Ash et al.11 in Georgia does, are there really any fewer handoffs between treatment providers than if the patient had been admitted to a hospital or outpatient program? In addition, would we not trade the small risk of information being lost in a hand-off between providers for the opportunity to treat the patient in a more therapeutic environment?
Others have noted that jail-based restoration programs eliminate the incentive for defendants to malinger incompetence (Ref. 5, p 78). Based on my experience in correctional environments, that assessment is overly optimistic. Although it is still in a jail, the competency restoration program described by Ash and colleagues11 offers substantial advantages over the typical general population housing unit, most notably single cells, enhanced therapeutic programming, and the presence of enthusiastic young forensic psychiatry trainees. At best, we might expect a slight decrease in malingering, but total elimination seems unlikely.
Finally, Ash and colleagues11 note that their jail-based competency restoration program offers an opportunity for mental health staff to intervene on patients' behalf and advocate for diverting them out of the criminal justice system. In fact, 31 percent of the patients in their Georgia program were diverted rather than restored to competence (Ref. 11, p 47), leading to the patients' quicker release from criminal justice custody. Nobody would find fault with this positive outcome, but admission to a jail-based restoration program is not the only way to identify appropriate candidates for jail diversion. In Connecticut, for example, social workers and other appropriately trained mental health professionals work in every arraignment courthouse in the state, actively identifying candidates for diversion and collaborating with judges and attorneys to arrange alternative dispositions. Most of these diversions occur at the arraignment stage, but a second set of jail-diversion professionals also interview candidates in jails around the state who may have been missed earlier, arranging placements in substance abuse programs, halfway houses, and other alternatives to incarceration. Clearly, robust jail diversion can and should occur independently of competency restoration, as it does in Connecticut.
I use my home state as an example not in an effort to boast, but rather to urge my forensic colleagues around the country not to give up on the idea of a functional, therapeutic competency restoration system that exists entirely outside of the correctional system. I know it is possible because I work in one every day. Furthermore, as litigation like Trueblood continues to expand around the country, courts and advocates are beginning to demand change to the underlying problems that drove competency restoration into jails in the first place: long wait times caused by insufficient community- and hospital-based programs to meet the needs for restoration and mental health services in general. My hope is that mental health professionals will continue this push, advocating for what we know is right, which is the development of a continuum of care that allows patients to be treated in noncorrectional settings whenever possible.
The reality is that jails simply do not need the additional burden of taking on competency restoration. Even in the smallest and least busy jails, new patients come in and out of the facility throughout the day, requiring fast-paced screening and triage. The first few days of incarceration are associated with a high risk of suicide, which requires careful assessment by skilled mental health professionals. In addition, many patients go through potentially life-threatening withdrawal from drugs and alcohol in the early stages of incarceration. All of these challenges create more than enough work for mental health professionals without adding additional tasks like competency restoration. As Felthous and Bloom eloquently noted, “If a jail has the resources to develop and staff a competency restoration program, it should first ensure that it is meeting the mental health needs that are properly and traditionally within its purview” (Ref. 9, p 369). I could not agree more.
Ultimately, I urge us to leave competency restoration where it properly belongs, in the mental health system. This does not mean that all patients should be restored to competency in inpatient settings; they should be matched to a level of outpatient or hospital-based care according to their clinical and risk-management needs. Although it is tempting to include jail-based restoration services in a continuum of care for justice-involved patients, doing so creates additional burdens for already overwhelmed correctional mental health systems. In addition, it creates the impression that jail-based restoration is the preferred method of service provision rather than what it really is: a temporary solution developed by well-meaning mental health professionals working in broken systems who simply could not bear to see patients wait months for treatment in alternative settings. In the coming years, I hope to see our profession collaborate with courts and legal advocates to find a permanent solution to this problem, enhancing both jail diversion services and noncorrectional competency restoration programs to meet the needs of this vulnerable population.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2020 American Academy of Psychiatry and the Law





{kind=link}