


Abstract
In March 2015, a co-pilot flying Germanwings Flight 9525 deliberately pointed his airplane into a descent, killing himself, five other crew members, and 144 passengers. Subsequent investigation and review teams examined the incident and considered potential lessons to maximize air safety. In this article, aviation industry clinical leaders, including the U.S. Federal Air Surgeon and Chief Psychiatrist from the Federal Aviation Administration (FAA), along with a professional pilot and collaborating forensic psychiatrists, discuss suicide-by-plane, evolving themes related to public safety responsibilities for psychiatrists treating pilots, and forensic trends in pilot evaluation for medical certification from an aerospace psychiatric perspective. We explore how psychiatric aspects of pilot fitness and aviation safety are examined across perspectives, including unsafe acts, preconditions, organizational factors, and unsafe supervision. We explore practices for civilian pilots and offer information related to military pilot fitness. Lessons from Germanwings are presented, as is the need for increased support for pilots who might be concerned about revealing mental health challenges for fear of loss of medical certification and pilot employment. The Air Line Pilots Association Pilot Assistance Network is highlighted as one example of pilots supporting pilots to increase airway safety.
The following is derived from the official reports1 of a tragic incident on March 24, 2015, when Germanwings Flight 9525, an Airbus A-320, crashed in the French Alps, killing six crew members and 144 passengers. This was described as a deliberate act of plane-assisted suicide (i.e., suicide-by-plane) by the co-pilot. At the time, the co-pilot was left alone on the flight deck while the captain went to the back for physiological needs. Due to previous terrorist incidents, this aircraft had a locked door that only could be opened from the flight deck. The co-pilot took this opportunity and refused multiple requests to open the door. He deliberately flew the airplane into the ground. Subsequent investigation lead to identification of the co-pilot's past medical history, which was documented to include known mental health diagnosis and treatment. Toxicology examination of the co-pilot revealed citalopram, mirtazapine, and zopiclone, none of which had been disclosed to the German civil aviation authority.
Reports indicated1 the co-pilot had flown for Germanwings since June 2014. He had learned to fly under U.S. regulations and had transitioned to European regulations as a condition of his employment with Germanwings. His initial U.S. Federal Aviation Administration (FAA) first-class medical certificate was issued in 2008 (a pilot must be certified as medically fit to fly). During the 2008–2009 timeframe, he experienced a severe depressive episode, without psychotic symptoms. In July 2009, he obtained a special issuance FAA medical certificate that reflected this medical history. A special issuance certificate indicates that there may have been some condition noted and that, with certain provisions such as monitoring, the pilot remains fit to fly. Once at Germanwings, his health was followed by European regulators.
In December 2014, five months after his last medical certificate was issued by European regulators, he developed psychotic depression. He consulted several mental health clinicians and was prescribed an antidepressant medication. In February 2015, he was diagnosed with a psychosomatic and anxiety disorder, and he was prescribed a hypnotic. In March 2015, the same month as the accident, the same physician diagnosed possible psychosis and recommended hospitalization. The co-pilot took sick leave for several days in February and March 2015. There was no communication between the clinicians and the German civil aviation authorities due to regulations in place at the time of the accident.1
The Germanwings incident was a watershed moment, with renewed attention from the public, pilots, and policymakers to psychiatric aspects of medical certification for pilots, and with heightened concerns about potential gaps. For mental health practitioners, it also pointed to the complexity of providing treatment or monitoring of commercial pilots. There are risks associated with under-recognizing psychiatric problems if those problems contribute to at-risk behavior. On the other hand, there are also risks associated with stigmatizing mental health needs with overly punitive policies that disallow flying for pilots with psychiatric concerns who would not be at risk, thereby disincentivizing the reporting of pilot mental health problems by those who might be concerned about loss of medical certification and their ability to pilot airplanes. The overarching safety of the airways is considered by regulators as the variable upon which policies must rest, but defining how to get there in practical situations and individual cases can be a challenge.
In this article we review aspects of pilot medical certification regarding mental health, suicide-by-plane, and recent efforts to help foster a culture of shared accountability and support to achieve the goals of airway safety and pilot fitness. Information in this review is offered with the goal of expanding the knowledge of those mental health professionals involved in pilot evaluation and treatment to improve the quality of pilots' lives and improve safety of the skies. Those planning to work with pilots or aviation organizations need to be able to apply their mental health knowledge and experience to this very specialized population. To that end, we review concepts that may be foreign to the average clinician but are essential for understanding the needs of pilots, their culture, and the regulations that govern them. To educate a broader range of clinicians and forensic evaluators about how they can approach engaging in this important work, we discuss mental health concerns for individual pilots as well as context about pilot culture and aviation organizational goals.
Aerospace Safety Culture
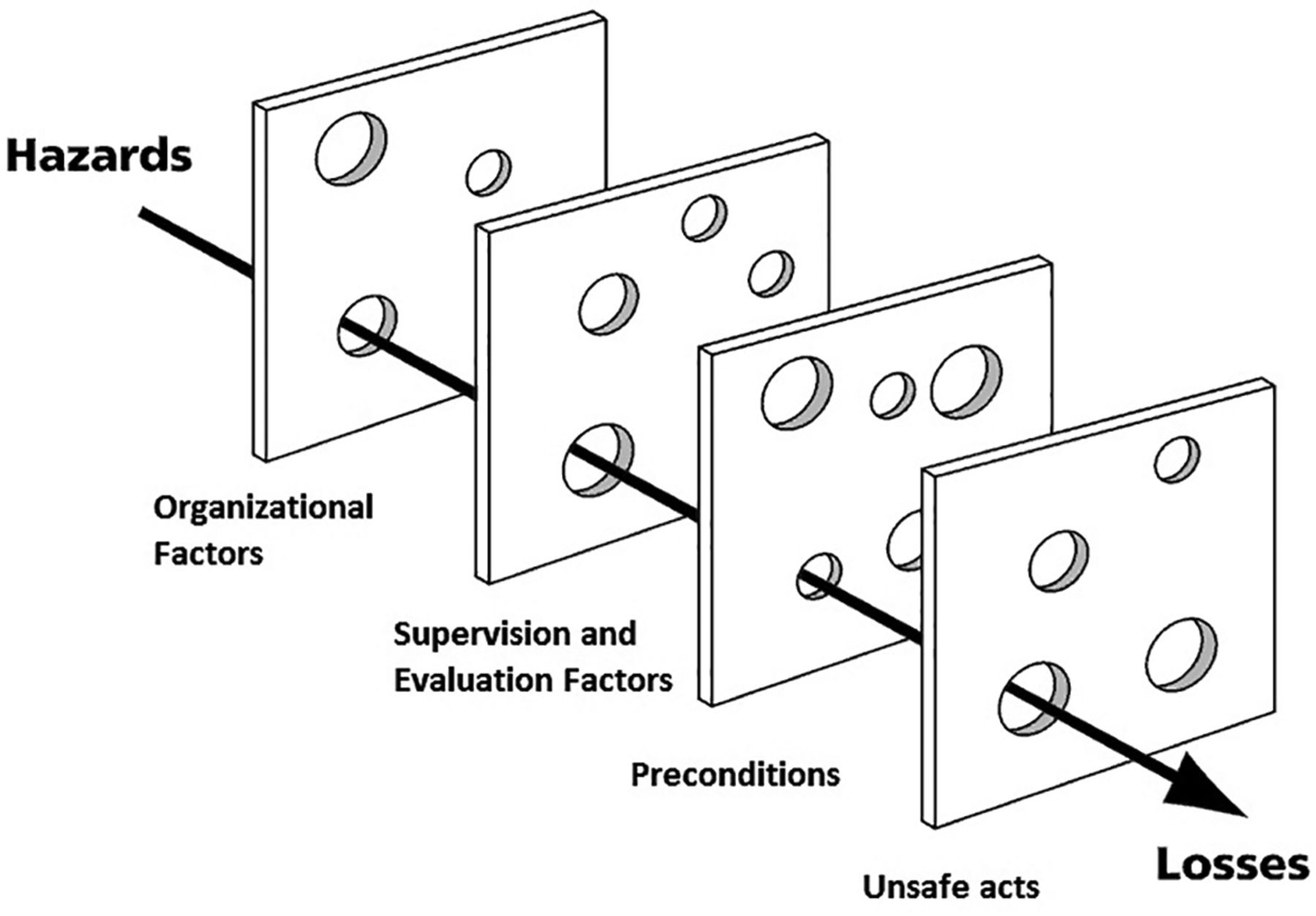
The notion of a “safety culture,” especially in high-risk industries (i.e., in which life and health may be at stake) such as aviation, has become increasingly recognized. A safety culture is an aspirational risk-management process in which organizational and individual factors are analyzed for the potential to increase or decrease risk. One common risk-analysis paradigm is known as the Swiss cheese model of system accidents in which people, policies, and technology can each represent safeguards and “defensive layers” (Figure 1).2,3 Although human error is inevitable, it is only when all the holes in defensive layers align that the risk of an end-state (i.e., irreversible) error occurs.

Swiss cheese model adapted from Wikimedia.org.3
Over aviation's history, the relative proportion of causal factors have shifted from being overwhelmingly machine causes to human causes.4 Just as pilots utilize preflight checklists for aircraft-related safety, the Aeronautical Information Manual (Ref. 5, p 535) recommends a pilot-fitness checklist using the “IMSAFE” mnemonic (i.e., illness, medication, stress, alcohol, fatigue, emotion) in accordance with FAA prohibitions on operations during known medical deficiency.6 Stress management is important for risk management because stress may cause a pilot to ignore all other risk factors. Pilots do not leave their stress and emotions on the ground. Here, we discuss four different preventive layers, emphasizing a psychiatrist's role: unsafe acts; preconditions and individual factors; organizational factors; and supervision and evaluation factors. We then present a potential initiative that is aimed at increasing safety while balancing complex interests.
Unsafe Acts in a Culture of Safety
Studies of pilot mental health are limited because they only capture those referred by self or employer, or they follow a bad outcome. Even anonymous web-based surveys related to pilot mental health have low response rates.7 Although there is a paucity of data on psychiatric disorders in pilots, it is important that psychiatrists consider aeromedical risks if they emerge when assessing and treating pilots.
Suicide-by-Plane
Available data suggest that pilots have up to a 13 percent one-week prevalence of clinically significant depressive symptoms, double the one-year prevalence of depression among all adults in the United States, and a 4 percent two-week prevalence of suicidal ideation.7 Based on findings and hypotheses from the cited study, potential explanations include the high stress of their occupation (e.g., long and continuous work hours) and sleep-related problems (e.g., circadian rhythm disruption, sleep medication use). Females, who account for 4 percent of U.S. pilots, were more likely than men to have depression, similar to the general population.7 Among fatal aviation incidents, 0.33 to 1.42 percent have been determined to be suicide-by-plane.8,9 All pilots completing suicide-by-plane were male, and their average age was 38 years, significantly younger than the average pilot age of 45 years. Most were private pilots with personal aircraft, rather than commercial or military pilots. Most experienced recent life stressors, most often relationship problems (e.g., divorce, separation), followed by legal, financial, and occupational stressors. Among this group of suicides-by-plane, 38 percent involved pilots who had preexisting mental health conditions, 50 percent involved alcohol or drugs, and 60 percent of the pilots had previously reported suicidal ideations to someone.8,–,11
Most instances of suicide-by-plane in these studies resulted in only the pilot's death. That said, plane-assisted homicide-suicides are a particular problem and have resulted in more than 700 deaths across at least 18 incidents. Homicide-suicides account for about 17 percent of pilot suicides, significantly higher than nonpilot suicides. Most commercial plane-assisted homicide-suicides occurred while the pilot was alone in the cockpit.8,–,11 This latter finding, especially in the wake of the Germanwings incident, has led to policy changes throughout the world. For example, many airlines that did not already require it, such as those in Europe, began to require two aircrew members to be in the cockpit at all times.
Flying Impaired
Although suicides-by-plane and homicide-suicides are particularly frightening, not all unsafe acts are so deliberate or malevolent. Substance intoxication or withdrawal can lead to a variety of dangerous symptoms, including sedation, disinhibition, poor judgment, mood changes, psychosis, cognitive impairments, psychomotor impairments, and inattention. Alcohol use has repeatedly been linked with aviation accidents and poor flight-simulator performance, both during intoxication and hours after use when blood alcohol concentrations are low or even after they have returned to zero.12,13 Prescription and over-the-counter medications, such as diphenhydramine, can have even more detrimental effects on driving performance than alcohol.14 These effects have led to stringent regulations on both substance use and allowable medications among pilots, and the FAA has implemented the Human Interventional Motivation Study (HIMS) program designed for pilots with substance use problems (https://himsprogam.com). Understanding of substance- and medication-induced impairments and related regulations are important for clinical treatment and independent psychiatric evaluations of pilots.
Fatigue, whether due to substances, stress, sleep deprivation, or long flights, can have detrimental effects on performance and can cause a pilot to ignore other risk factors. That is why the FAA has developed a policy for fatigue risk management.15 Studies have reported fatigue to be common among aircrew, with 21 percent of military aircrew and 31 percent of civilian aircrew reporting fatigue.16 Subclinical fatigue that may not cause impairment for the general population may cause unacceptable risks in pilots. Likewise, attempts to counteract fatigue, such as the use of stimulants (e.g., caffeine, prescribed, illicit), can cause risks. Unfortunately, the combination of stress, sleep deprivation, and stimulants is a recipe for the occasional presentation of brief psychotic episodes among pilots, such as among military pilots prescribed “go pills” to maintain alertness during flying.17 In cases where the symptoms resolve quickly and there is no recurrence after a prolonged period of time without antipsychotics, and the cause is definitively identified and determined to be preventable, waivers in the military for flying are often granted.
Preconditions and Individual Factors
Preconditions for safety assume that pilots are appropriately suited on any given day to fly. The public image of pilots may be based on media portrayals (e.g., movies such as Top Gun and Sully), and these portrayals and public expectations greatly influence pilot identity and self-expectations. How often do airplane passengers wonder if their pilot is suicidal or intoxicated? How often does anyone think about the pilot at all? Whether engaging in psychological self-protection or simply being unaware, most people do not consider the human factors involved with commercial flight. Because pilots are human, however, only prevention and mitigation of error is possible; the elimination of error is not possible. What happens, then, when pilots do not meet their own perfectionistic standards or those held by the public?
Pilots tend to be reliable, physically fit, highly motivated, and intelligent (e.g., USAF pilots have an average IQ of 125, about the same as physicians).18 These characteristics are partially explained by the type of people who are drawn to aviation and the selection process via medical certification and pilot training.
Despite the high expectations, preconditions that can result in tragic outcomes can occur when a pilot is dealing with a life stressor that destabilizes the ability to function fully. It is possible for pilots to be highly successful at work but dysfunctional at home. For example, pilots may be gregarious with co-workers but emotionally detached with family, they may accumulate both job promotions and divorces, or they may obtain advanced degrees but sleep in their car due to financial trouble. Life dysfunction might be attributed to psychiatric disorders, personality, interpersonal skills, and dysfunctional coping, but it can also be caused or exacerbated by frequent travel away from home and sleep disruption that are inherent to the work, despite regulations that try to mitigate these. Pilots are required and trained to avoid flying if they are facing a life circumstance that could destabilize them. Such self-awareness may not, however, always be inherent. Thus, preconditions for pilots can be a precursor, as in the Germanwings incident, to unsafe airways.
Mental health treatment avoidance and under-reporting of symptoms (e.g., minimization and dissimulation, also known as “reverse malingering” or “faking good”) are risks among pilots. Evidence of under-reporting includes toxicology results from 4,143 civil pilots who died in aviation accidents.19 Only 8 percent of those taking medications and 6 percent taking psychiatric medications had disclosed their medication use to the FAA (via FAA Form 8500-8). The most commonly nondisclosed medication group was psychiatric, followed by cardiovascular and neurologic.
When there is nondisclosure and avoidance of treatment, it may be driven by some combination of occupational factors (e.g., fear of negative career impact, concerns for confidentiality, etc.), psychological factors (e.g., embarrassment or shame, fear of losing identity or purpose, belief that nothing can help), social factors (e.g., fear of losing membership in a select group, of being viewed as unreliable by co-workers or the public), cultural attitudes (e.g., overvaluing self-reliance, stoicism, masculinity; perceiving disorder as a weakness), and general help-seeking deterrents (e.g., stigma, denial, lack of mental health knowledge).20 The significance of the fear of being deemed unreliable cannot be underestimated. Reliability is an essential trait of pilots, an expectation of co-workers and the public, and part of pilots' sense of self. To be viewed otherwise can be devastating, and the fear of such devastation can lead to minimization, denial, and, paradoxically, the very unreliability that was feared. It is essential that pilots (and their supervisors) understand that self-disclosure (e.g., asking for a break on a bad day) is, itself, a mark of reliability.
In a study from Australia, where pilots have been allowed to take antidepressants since 1987, there were no significant differences in aviation accidents or incidents between civilian pilots who did or did not take antidepressants.21 This suggests that neither these medications, nor the conditions they are controlling, reduce safety. And although pilots with mental health problems are less likely to seek treatment, they are more likely to successfully recover. For example, military pilots receiving alcohol-use disorder treatment have 95 percent three-year and 88 to 90 percent lifetime abstinence rates,22 whereas the general population has an 18 percent one-year abstinence rate,23 likely exemplifying pilots' characteristically high motivation and the high stakes involved (i.e., losing medical certification and livelihood). Allowing for psychiatric treatment, while still regulating its limits, should not be viewed as lowering safety standards. In fact, treating medical conditions should be viewed as raising safety standards because inadequate treatment and disincentivizing self-disclosure both increase risk. In this way, mental health treatment and self-disclosure for many pilots can help ensure positive preconditions for flying.
Organizational Factors
For forensic psychiatrists performing pilot evaluations and consulting with organizations, it is important to be aware of aviation industry concerns. In addition to operating within a safety culture, governmental organizations and airline companies have rules and regulations governing mental health that affect pilots' abilities to exercise the privileges of their license. When regulators are faced with mental health-related concerns reported by pilots, they may rely on experts to provide clinical observations and opinion data that subsequently allow them to determine the pilot's fitness for medical certification. The ultimate authority for this regulatory power derives from the public interest in ensuring safety in the skies. Therefore, it is important for psychiatrists seeing pilots, in both treatment and occupational or fitness for medical certification contexts, to have some familiarity with aviation regulations and common safety concerns.
Federal Aviation Regulations
FAA medical exams (i.e., flight physicals) are performed by physicians known as aviation medical examiners (AMEs), who are designated as representatives of the Federal Air Surgeon to conduct exams.24 FAA medical certification is divided into three classes: airline transport pilot (first class), commercial pilot (second class), and private pilot (third class).25 Table 1 presents federal aviation regulations regarding psychiatric disqualifiers.26 According to the federal aviation regulations, the FAA does not use diagnostic codes from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, or the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, but the FAA specifically mentions psychosis, bipolar disorder, personality disorder, and substance use disorders as disqualifiers. Depression and suicidality are notably not mentioned. In fact, federal aviation regulations do not specifically address most psychiatric disorders (e.g., obsessive compulsive disorder, eating disorders, attention-deficit hyperactive disorder). These may fall under a “neurosis, or mental condition” that impacts safety or ability to perform duties, which the Federal Air Surgeon may deem disqualifying. A special issuance medical certificate may be granted on a case-by-case allowance for one of the following: major depressive disorder (mild to moderate), either a single episode or recurrent episodes (if treated); dysthymic disorder; adjustment disorder with depressed mood; and nondepressive disorder for which particular selective serotonin reuptake inhibitors (SSRIs) are used.27 Special issuance certificates that allow a pilot to be on SSRI medications, for example, require stability and no aeromedically significant side effects for six months.27 The FAA allows waivers for only four psychiatric medications, all of which are SSRIs: fluoxetine, sertraline, citalopram, and escitalopram.27 FAA waivers are not permitted when the use of the SSRI is proposed in an individual with a history of psychosis, suicidal ideation, electroconvulsive therapy, multiple SSRI use, or history of use of other psychiatric medications with SSRIs.27 Aviation industry concerns may not always be in sync with the regulatory responsibilities of the FAA and may not be readily obvious to those in forensic practice, but familiarity with regulations and consulting with aeromedical experts and forensic psychiatrists experienced in aeromedical regulations can help guide clinical assessments, treatment recommendations, and occupational recommendations.
Federal Aviation Mental Health Disqualifiers (14 CFR § 67.107)6
Military Regulations
Unlike the FAA, the military classifies all mental disorders as potentially disqualifying.28 Some conditions are potentially “unfitting” for military duty (e.g., psychosis, bipolar disorder, depression) and can result in disability benefits, but others are considered “unsuiting” (e.g., substance use, personality disorders) and can result in administrative separation without benefits.28 Classification of unfitting and unsuiting diagnoses vary between military branches and jobs.28 All disorders require assessment and can result in service members being discharged from service or returned to duty with or without restrictions. In the U.S. Air Force (USAF), flying waiver requirements include “no risk of sudden incapacitation,” “minimal potential for subtle performance decrement,” “low possibility” of progression or recurrence, expected stability even “under aviation stresses,” and condition-dependent time requirements for symptom remission (e.g., at least 1 year for psychotic or somatic disorders; at least 6 months for depression, anxiety, or suicidality; at least 3 months for alcohol use disorder; the flight surgeon's discretion for adjustment disorders).17,29 Often psychotherapy “booster sessions” or antidepressants are permissible or even advisable after symptom resolution.17 In the experience of one author (J.G.), common restrictions for returning to duty included no deployments, no firearms, no alcohol use (e.g., on or off duty, with regular monitoring), no flying, no flying certain aircraft, no stimulants while flying, flying duration limits, preflight mandatory sleep durations, and only being stationed at bases with psychiatric services. Any of these will require at least annual reviews.17 Although these restrictions can reduce risk, clinicians and commanders should be mindful that they can also increase stigma and impact rank promotions, which in turn could increase risk. For example, pilot stress could be exacerbated by co-worker knowledge of the pilot's restrictions, and other pilots may be deterred from self-disclosure. Such matters should be carefully balanced and zero-tolerance, absolutist policies should be avoided in favor of case-by-case evaluations.
Medication policies vary depending on branch of service and job duties. For example, the USAF does not allow any psychiatric medications for personnel working around nuclear material.30 For flyers, the USAF limits psychiatric medications to four antidepressant monotherapies (i.e., bupropion, citalopram, escitalopram, and sertraline), two “go pills” while in-flight (i.e., dextroamphetamine, modafinil), and three “no go pills” for premission sleep (i.e., temazepam, zaleplon, zolpidem).31 Although data related to these medications and accidents are scant, the USAF elected to allow three of the same antidepressants as the FAA but replaced fluoxetine with bupropion in an attempt to avoid longer-acting agents in the event of adverse effects.17 Clinicians must consider medication regulations to guide treatment decisions.
Supervision and Evaluations
Pilot Medical Certification Evaluations
The FAA and military rely on clinicians to evaluate diagnosis, prognosis, treatment, and functioning of pilots. Their professional presentation of objective clinical findings in a systematic fashion allows regulatory bodies to ensure policy compliance, determine potential functioning and safety concerns, and mitigate risk when making individual certification decisions. Data related to medical reliability are essential to pilot certification and supervision.
Appropriately trained psychiatrists (and psychologists or neuropsychologists at times) are called upon by regulators when there is evidence to suggest that a pilot has a disqualifying mental health condition, or when there is a concern requiring additional information for certification. Regular medical certification is based on the premise of safety of the national air space system and defined by regulations unique to pilots. Familiarity with regulations is critical to conducting proper evaluations. Pilot medical certification varies in duration and requirements for type of work, time frame, and age factors for renewal. AMEs are usually primary care doctors, but a few are psychiatrists. Designations are made by Regional Flight Surgeons32 based on the needs of the Office of Aerospace Medicine. The FAA also may refer cases to forensic psychiatrists who are not AME- or HIMS-trained to opine on diagnosis, proper treatment, and prognosis. In the military, treating clinicians (both active-duty and civilian staff) are responsible for regularly assessing fitness for duty, although service members are often referred to nontreating evaluators for occupational assessments.
Aeromedical evaluations by forensic psychiatrists may be particularly helpful in specific cases, especially when there is a debate about diagnosis, dispute between the records and self-reporting, or competing clinical opinions. In other instances, addiction or other specialists might be preferable. Referrals for psychiatric evaluation for aeromedical certification can be based on discovery of a psychiatric history during certificate application or medical examination, pilot-monitoring plans, or pilot-conduct problems. Psychiatric evaluations can enter into legal arenas in that highly motivated pilots seeking medical certification can challenge findings that result in denial of their certification. The FAA has the authority to make final determinations, but cases related to medical certification denial can be appealed to the National Transportation Safety Board (NTSB) and adjudicated by an NTSB Administrative Law Judge, who determines whether regulations were appropriately followed. Even a pilot deemed fit for medical certification might be a poor company employee due to other conduct problems. Employment/administrative and medical/psychiatric concerns may be intertwined (e.g., certain personality factors) or separate and distinct. Employment factors are not relevant, however, for private pilots seeking certification.
Psychiatrists with specific training approved by the FAA are often utilized to conduct evaluations, provide context, sort through disparate clinical information, and render opinions. The FAA often needs psychiatrists to clarify ambiguities in a pilot's medical history and records, and to identify what is and is not relevant to occupational functioning and safety risk in accordance with federal aviation regulations. The AME is often confronted with balancing regulatory obligations with a competing desire for pilot advocacy. Countertransference factors may influence an AME's objectivity. It is important for those psychiatrists evaluating pilots to recognize that subclinical symptoms that would not impair the average person may be aeromedically significant. Symptoms such as mild inattention, fatigue, insomnia, or anxiety may not substantially interfere with the functioning of someone working in an office or stockroom, but these same symptoms could be detrimental to a pilot's ability to function as a crewmember. For example, someone experiencing a panic attack on the ground can take a break from work to employ relaxation techniques, but a pilot needs to remain attentive to maintaining aircraft safety. Evaluators assessing individuals for medical certification should assess how symptoms impact pilot functioning but focus examination on whether there are potential disqualifying factors that are elucidated in the overall assessment.
The Role of Treating Psychiatrists
Treating pilots requires consideration of both personal health and flight safety. There are disqualifying diagnoses and disqualifying treatments. Until relatively recently, all psychotropic medications were disqualifying. The concordance between what may be clinically appropriate and what is aeromedically acceptable is not seamless. Sometimes what the patient wants comes into conflict with flight safety. For example, a patient may have failed with all of the regulation-approved antidepressants and only responded to a medication that is not approved (e.g., a serotonin-norepinephrine reuptake inhibitor, antipsychotic augmentation). If the pilot decides to stop the effective medication to be eligible to fly again, both clinician and pilot must weigh the risk of relapse against the risk of worsened mental health if the pilot is no longer able to fly. Furthermore, both must be aware of the time period off the medication that the aviation regulatory body may require, as well as the risk that the pilot may not be approved to fly again. The best advice for a treating psychiatrist is to first provide the best treatment possible, and then work to support the patient when the treatment may have aeromedical implications. Prescribers should have knowledge of nondisqualifying treatments and try them first, if appropriate. For example, when treatment options are equally efficacious, favoring the ones permissible by regulations can save time and heartache.
Clinicians should ask pilots for details about their job and how they are functioning. Collateral information from an employer can also be helpful, but in civilian contexts this may not be part of routine treatment. Factors to investigate include career progression, awards, disciplinary problems, attendance problems, productivity and performance, the specific skills and tasks required of specific jobs, and sudden or progressive changes in any of the above. Pilots can have unique job demands, so understanding these demands and their performance can allow clinicians to better assess pilot patients and to better focus on specific strengths and vulnerabilities.
Documentation is important when evaluating pilots. Treating psychiatrists should be aware that their notes might be reviewed by an aviation regulatory body, but documentation should be maintained as needed for clinical purposes. Focusing on areas of functioning or dysfunction and supporting diagnoses with clear examples of symptoms can improve the occupational utility of records. Ambiguous or “soft” documentation may seem satisfying to clinicians worried about negatively affecting a patient's career, but when records are reviewed, inaccurate or unclear information can actually delay or prevent medical review processes, lead to incorrect or suboptimal treatment recommendations, or result in inappropriate occupational recommendations (e.g., unnecessary disqualification, unfit pilots putting themselves and others at risk). The FAA wants clinicians to do their job as they would with any other patients. The FAA does not want clinicians to opine on pilot fitness, but to provide factual information to allow the FAA to make determinations (e.g., the diagnosis and how that diagnosis affects the pilot).
When a patient is a pilot, the threshold for reporting concerns about public safety is arguably lower than for average patients. State laws and confidentiality rules may create barriers for reporting, however, and reporting concerns may be limited by fear of breaching confidentiality or concern that the patient will be dissuaded from providing information to help conduct a thorough risk assessment and remain in treatment. Psychiatrists evaluating pilots can face many risk-management challenges, particularly with pilots who are expressing suicidal or violent ideation or conveying risk of harm, but with no expressed plan or intent. Even in states with laws that mandate a duty to protect the public at large when a threat to safety is presented by a patient, beyond addressing the risk with hospitalization when feasible, there may not always be a clear means to take further action in the context of risk to airway safety. The FAA's and military's perspectives on overriding duties are clear in prioritizing aerospace safety, but to a private civilian psychiatrist with no attachment to the FAA or the military, this might not create a clear path of communication. For these regulatory oversight bodies, confidentiality concerns are not thought about in the same way as in treatment contexts; in clinical treatment of pilots, public safety concerns may supersede confidentiality in a way that would not occur in the treatment of people in other professions (e.g., the necessity to report substance use or subclinical symptoms). A full analysis of duty-to-protect statutes as they relate to pilots across jurisdictions is beyond the scope of this article, but consideration of these complexities is critical. Treating clinicians should consult liberally with risk-management entities, the FAA Aerospace Medical Certification Division (405-954-7653), or with colleagues who understand aerospace safety considerations and confidentiality guidelines.
Unlike civilian clinicians, military clinicians not only have a duty to the patient and the public, but also to the military mission. Beyond typical exceptions to confidentiality, such as risk to self or others and suspected child abuse,33 military clinicians are also mandated to report risk to mission (e.g., inpatient care; problems with substance use, impulsivity, insight, reliability, judgment).34 With stakes being as high as national security, such measures are necessary, but they also may deter self-disclosure and help-seeking among military aviation personnel.
Suicide Risk Assessment
It should be noted that suicide by pilots is rare, and most pilot mental health concerns are of a much lower severity. Nonetheless, whether assessing a pilot for treatment or as part of an occupational evaluation, suicide risk must be addressed because it is a potential danger to both the pilot and the public. The basic standards of care in assessing acute and chronic risk factors and protective factors apply here, but with additional considerations for pilots. As noted earlier, pilots may appear functional in many domains of life, hiding dysfunction in other domains. It is easy for clinicians to overlook or dismiss signs of potential problems that may in fact be the tip of the iceberg. Furthermore, pilots are motivated to appear reliable to keep their job, and therefore they have a propensity for intentionally or unintentionally under-reporting symptoms and engaging in positive-impression management. To best address this, clinicians might attempt to gather collateral sources (e.g., spouse, supervisor, commander in military contexts, parents, and friends). Basic clinical suicide and depression screens are often used in general care settings but could be misleading in suicide risk screening of pilots if the individual is motivated to appear nonsuicidal (e.g., it is easy to cite “none” or “never” on screening tests asking for presence or frequency of suicidal thoughts).
Additionally, clinicians should have an understanding of both the real and imagined consequences of self-disclosure. One can start by asking about the pilot's expectations of evaluation and treatment. Responses to and education about the pilot's concerns should be based on knowledge of the actual regulations and consultation with the FAA, aerospace medicine physicians, or military flight surgeons (e.g., the USAF Aerospace Consultation Service at Wright-Patterson Air Force Base). The consequences of having a mental health diagnosis or using certain substances or medications may vary based on diagnoses, the treatment needed, and the applicable regulatory body. Contrary to expectations of most pilots undergoing evaluation by the Aerospace Consultation Service, the USAF's goal is to get grounded pilots (i.e., those with duty-not-involving-flying restrictions) back into the air as quickly and safely as possible, and most of them will receive waivers once their condition is stable with appropriate treatment.17 Civilian standards with the FAA are focused on keeping the airways safe, and the federal aviation regulations will dictate what is disqualifying. Because the mission is to protect national airspace, however, regulatory bodies tend to be very conservative about these matters. Accurate policy knowledge is essential to avoid false promises and to establish trust. Trust and rapport encourage accurate reporting of suicide risk and preventive factors.
Searching for Solutions
With increased awareness, especially after events like the Germanwings incident, many organizations have sought to add extra layers of prevention and to better align or shrink the holes in existing layers.
Aviation Rulemaking Committee (ARC)
In 2015, the FAA Administrator chartered the ARC in response to a recommendation by the Civil Aviation Safety Team following concerns over Germanwings Flight 9525 and Malaysia Flight 370.35 The ARC included 23 members, comprising representatives from industry groups, unions, and the FAA. The ARC met monthly for the following year, both collectively and in working groups of subject matter experts, which reported information back to the ARC. Among these, the Medical Working Group included 12 individuals (i.e., psychiatrists, psychologists, and aerospace medicine specialist physicians).
The ARC report35 recommended creating an environment encouraging pilot self-disclosure; improving access to health care and support; expanding pilot-support programs; educating air carriers and pilots on mental fitness for duty; ensuring that pilot care is confidential and nonstigmatized; building risk-mitigation processes on top of existing safety management system principles; and addressing pilot mental fitness using a holistic approach. On the basis of these recommendations, the FAA instituted enhanced mental health training for AMEs in 2016 and advocated for a uniform national policy on mandatory reporting of medical concerns that affect public safety, which was passed by the Aerospace Medical Association in 2016. On the basis of the ARC findings, the FAA determined there were no convincing data to suggest routine psychological testing would be helpful in periodic medical certification evaluations, and that no changes were needed regarding existing FAA standards for aircraft or flight deck door design, standard flight deck access, and the requirement for two persons to be on the flight deck at all times.35,36 Progress is ongoing in the FAA's implementation of other ARC recommendations, such as the implementation of mental health education programs to improve awareness, reduce stigma, and promote available resources; the development of effective pilot assistance programs; and the creation and dissemination of information on pilot-support programs.
Pilot Support Programs
The Air Line Pilots Association (ALPA) is a union representing more than 58,000 pilots across 33 U.S. and Canadian airlines. ALPA's mission is air safety, security, advocacy, representation, and pilot assistance. Pilot-assistance programs include HIMS, the Critical Incident Response Program (CIRP), Professional Standards, and Aeromedical. HIMS began in the 1970s as a joint partnership with airlines, FAA, and ALPA to assist pilots diagnosed with substance use disorders to regain medical certification.37 CIRP developed after the Origins 1988 Aloha Flight 243 incident and relies on trained peer volunteers who target pilots experiencing unexpected stressful events that overwhelm coping skills.38 ALPA's Professional Standards uses peer volunteers who target pilot behavior and conflict resolution in the workplace. ALPA Aeromedical has a peer-assistance program that helps pilots with FAA medical concerns and with reporting medical conditions and treatments to the FAA for continued certification.39
One author (H.M.P.) was instrumental in the development of an ALPA-sponsored, single-airline, peer-support program for pilots facing aeromedical, psychological, and physiological challenges.40 It is called the Pilot Assistance Network (PAN) and began as a grassroots effort in 2000. “PAN,” like “may day,” is a pilot distress signal. A similar support program was adopted across ALPA.41 Unlike the more common phrase of “may day,” PAN refers to a slow or insidious onset that eventually overwhelms. Pilot peer volunteers are available at all times to provide strictly confidential support and encourage the utilization of all available resources. PAN encourages pilots to be mindful of their own mental health with the goal of helping pilots help themselves as they safely navigate treatment of an unfamiliar medical or mental condition that is perceived to be career-ending. Common pilot concerns seen in PAN include depression, anxiety, divorce, child-related stressors, elder care, training difficulties, and cognitive impairment. Common fears expressed among pilots seeking PAN support include concerns about loss of pay, job loss, negative action against the pilot, potential denial or loss of FAA medical certification, and embarrassment.
An equally important aspect of this program is that, by allowing pilots access to appropriate medical care, safety of the skies is increased. The reason this model appears to be so successful is the ability to leverage the value of peer support for a pilot in need. To be successful, the program requires mutual trust from union officials, the company, and regulators. With PAN, the airline has placed an incredible amount of trust in the peer volunteers and takes a hands-off approach, initially allowing pilots the space needed to obtain appropriate health care treatment without interference. This trust is enhanced through training supported by and attended by the leadership of administrative groups, aviation companies, and the FAA. In this way, the network provides additional layers of protection against holes in the defensive layers aligning in the overall system. Once a plan is in place to approach personal problems, pilots can approach their chief pilots (i.e., supervisors) in a confidential manner. The FAA has also provided assurance that the pilot will be treated fairly and in all likelihood can be requalified to fly after appropriate reporting. The PAN model was touted as an example of good practice in the final report on the Germanwings Flight 9525 investigation.1 PAN′s future goals include improving mental health education for the pilot community, assistance in access to high-quality treatment, and enhancing safety nets to encourage accessing care before problems become more significant (e.g., removing risk to pay if a pilot engages in treatment, ensuring that psychiatric disability coverage is on par with medical disability).40,42
Peer support allows for empathy with an understanding of how best to speak another pilot's language. As only other pilots can truly know, obtaining pilot medical certification and completing the FAA Form 8500-8 disclosing medical background can be daunting tasks. Confidential peer support and encouraging pilot access to appropriate care, with cooperation from companies and regulators, can increase the likelihood of treatment and improve aerospace safety, with the eventual goal of returning the pilot safely to the flight deck.
Conclusion
The Germanwings Flight 9525 incident brought to light the importance of pilot fitness, certification policies, and evaluations pertaining to mental health and wellness. Pilots, airlines, the FAA, and the military reexamined how policies and perceptions affect stigma and willingness to self-disclose at the individual and professional levels and at the regulatory level. Pilot health has significant implications for public safety, with mental health factors ranging from subclinical mood, sleep, and attention problems to the rare but alarming and dramatic cases of suicide-by-plane. Aviation safety relies upon a number of prevention strategies (i.e., layers), including proper medical supervision and treatment and reliable pilot self-disclosure. With specialized training in objective evaluations based on the interface between psychiatry and formal rules, forensic psychiatrists are uniquely qualified to navigate challenges associated with pilot safety in complex cases, assisting in medical certification evaluations and policymaking. Knowledge of the unique elements of aeromedical safety is critical in such work, which goes beyond traditional forensic psychiatry training. Understanding of the regulations and familiarity with pilot functioning and identity can also be important for those who provide support, monitoring and treatment of pilots.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2020 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}