


Abstract
This article presents a survival analysis of long-term risk of firearm-related and other violent crime in a large sample of adults with serious mental illness in Florida, comparing those who received a gun-disqualifying civil commitment after a short-term hold, those who were evaluated for commitment but were released or hospitalized voluntarily, and a third group with no holds or commitments. Among 77,048 adults with a diagnosis of schizophrenia-spectrum disorder, bipolar disorder, or major depression, 42.7 percent were detained for psychiatric examination under Florida's Baker Act; of that detained group, 8.4 percent were involuntarily committed while the remainder were released within 72 hours or agreed to voluntary admission. Over a follow-up period averaging six to seven years, 7.5 percent of the sample were arrested for a violent offense not involving a gun, and 0.9 percent were arrested for a violent crime involving a gun. A short-term hold with or without commitment was associated with a significantly higher risk of future arrest for violent crime, although the study population had other violence risk factors unrelated to mental illness. Risk of gun-involved crime, specifically, was significantly higher in individuals following a short-term hold only, but not in those who were involuntarily committed and became ineligible to purchase or possess guns. Policy implications are discussed.
- involuntary commitment
- short-term psychiatric holds
- firearm restrictions
- gun violence prevention
- serious mental illness
- violent crime
The widespread closure of U.S. psychiatric hospitals and general hospital psychiatric units over a period of decades without a reliable community care system to replace them has been recognized as a public policy failure contributing to lack of treatment and poor outcomes for adults with disabling psychiatric conditions.1,–,3 In recent years, some observers have implicated this larger problem in preventable incidents of gun violence and suicide.4,–,6 Deinstitutionalization and a tightening of civil commitment statutes across the country brought a steep decline in use of involuntary civil commitment, which had served not only as a legal means to confine persons with incapacitating mental illness who required inpatient-level treatment to mitigate dangerousness, but also as a mechanism for firearm disqualification applied to such individuals.7 A corresponding increase occurred in short-term involuntary holds for emergency psychiatric evaluation, which usually do not result in extended inpatient treatment or confer loss of gun rights.8
Research is needed to better understand the risk of gun-related and other violent crime among adults who are involuntarily committed to a hospital, compared with the larger group who are held for a psychiatric evaluation but released after a brief period or agree to voluntary admission. Although previous research has shown that individuals with mental illness are more likely to be victims than perpetrators of crime,9 and that mental illness in general accounts for just four percent of the attributable risk for interpersonal violence in the population,10 prominent proposals to reduce gun violence continue to target mental illness.11 Fair and effective violence-prevention policies should be evidence-based and focused on individuals with known indicators of significant risk.
The first part of this article frames the study's research questions with a summary of the historical, legal, and policy context underlying connections between psychiatric hospitalization, involuntary civil commitment, dangerousness, gun violence, and gun rights restrictions. The second part presents an empirical examination of the risk and correlates of violent crime, with and without firearm involvement, in a sample of 77,048 adults with a diagnosis of schizophrenia-spectrum disorders, bipolar disorder, or major depression in the public behavioral health systems of two large counties in Florida between 1998 and 2011. Using these longitudinal data, we conducted a multi-year survival analysis comparing violent crime outcomes across subgroups who underwent a short-term emergency hold followed by a gun-disqualifying involuntary commitment, those who agreed to a voluntary hospitalization or were released following a short-term hold, and those who had neither of these legal interventions. Finally, the article discusses possible interpretations of the study's findings and explores policy implications.
Involuntary Commitment and Gun Rights
Decline of Hospital-Based Psychiatric Care
Patients with a record of involuntary commitment to a psychiatric hospital have been legally disqualified from purchasing or possessing firearms for over 50 years, since Congress enacted the Gun Control Act of 1968 following the assassinations of Dr. Martin Luther King, Jr., and Sen. Robert F. Kennedy. In the era when that law was passed, nearly one in ten adults with a serious mental illness resided in a state psychiatric hospital, a total of about 400,000 patients throughout the United States.12 More than half of them were held involuntarily,13 under permissive commitment laws that allowed confinement of persons deemed to need inpatient mental health treatment, in the years before civil-rights–driven litigation narrowed commitment standards to require dangerousness consistent with use of police powers to protect the public.7
A half-century later, following deinstitutionalization and reform of civil commitment statutes, only an estimated one percent of the 11.4 million adults with serious mental illness in the United States experience involuntary commitment in a given year14,15; less than half of that one percent (about 40,000 individuals total) are treated in state psychiatric hospitals.12 Overall bed capacity has declined and shifted largely from state psychiatric hospitals to general community hospitals with psychiatric units, where the majority of admissions are of short duration and do not involve civil commitment.12,15 For their part, state psychiatric hospitals tend to admit the most severely ill patients who pose safety concerns and need longer stays, which occur disproportionately under commitment. The excess demand for psychiatric beds has prioritized court-ordered and forensic admissions to state hospitals and changed the case mix of these facilities.16 From 1972 to 2014, the proportion of involuntary patients in state psychiatric hospitals increased from an estimated 52 percent to 83 percent, while total admissions dramatically declined.12,13 The net result of these trends for firearm policy is that a much smaller proportion of people with serious mental illness are legally disqualified from purchasing firearms by dint of a recent commitment record, but those who do become disqualified are more likely to have experienced severe symptoms associated with dangerousness and need for a longer hospital admission.
A Changing and Uncertain Legal Landscape
The question of whether persons with a remote history of involuntary commitment should be banned from owning guns, effectively for life, even if they have recovered from mental illness and have no other contemporary indications of risk, remains an open one. To date, three federal appeals courts have come to different conclusions on this question. In 2016, a majority opinion from the U.S. Sixth Circuit Court of Appeals concluded that Charles Tyler, a Michigan man who was denied a firearm purchase due to a single record of civil commitment many years in the past, had a “viable claim under the Second Amendment and that the government has not justified a lifetime ban on gun possession by anyone who has been ‘adjudicated as a mental defective’ or ‘committed to a mental institution’” (Ref. 17, p 699). The court's ruling implied that states must provide a “back door” to gun restriction in such cases (specifically, an opportunity for gun rights restoration for persons who are no longer dangerous) if the longstanding policy of gun disqualification predicated on civil commitment is to be determined constitutional.18 In 2019, the U.S. Third Circuit Court of Appeals addressed a similar question in a different case and concluded that persons disqualified from firearms due to involuntary commitment fall outside the category protected by the Second Amendment right.19 In 2020, the Ninth Circuit Court of Appeals considered research evidence of suicide risk associated with a history of involuntary commitment and concluded that a lifetime gun prohibition for these individuals was a reasonable limitation of the Second Amendment right, consistent with the U.S. Supreme Court's opinion in District of Columba v. Heller.20,21
State commitment laws also authorize courts to direct law enforcement officers to detain and transport individuals thought to be in a mental health crisis to a health care facility for a brief period of evaluation, typically up to 72 hours.8 Several different terms are used for these short-term holds in research literature and in practice across jurisdictions. The State Profiling System Survey of state mental health authorities15 refers to them as “involuntary holds” which is a term distinct from “involuntary commitments.” A research article comparing these laws across all 50 states and the District of Columbia uses the phrase “emergency holds for mental health stabilization” (Ref. 8, p 529).
Under Florida's Baker Act,22 an “involuntary examination” can be initiated by an authorized mental health professional, law enforcement officer, or a circuit court ex parte order when there is reason to believe a person has a mental illness and, as a result, is likely to experience neglect or to cause harm to self or others but is unable or unwilling to participate voluntarily in a psychiatric examination. To facilitate involuntary examination, police may transport an individual to a receiving facility where the person can be held for up to 72 hours, after which the facility must petition for involuntary placement or the person must be released or admitted voluntarily to a hospital.
In 22 states (as of 2016),8 a short-term hold for commitment evaluation creates a legal restriction of a person's subsequent ability to access firearms, at least for a period of time, such as 6 months. Short-term holds for evaluations are far more common than longer-term involuntary commitments. States vary in their practice, but national surveys of state mental health authorities suggest that, on average, more than five times as many adults are briefly detained for a mental health examination (before being released or admitted voluntarily) than receive extended inpatient treatment under a civil commitment order.15
Mental Health Services and Public Safety
Public safety may have been affected by the gradual shift away from hospital-based involuntary treatment in state institutions and toward increased frequency of release following short-term holds. Certain highly publicized incidents in recent years have shone a light on what can go wrong, in the worst-case scenario, when a person who is acutely mentally ill is unable to access a psychiatric hospital bed or fails to meet criteria for involuntary commitment in the midst of a dangerous crisis. In November 2019, a 24-year-old Virginia man experiencing a psychotic episode was evaluated by mental health professionals under an emergency custody order but released because no psychiatric bed was available. A few hours later, the young man stabbed his father in the chest and head before ending his own life with a gun. This incident received national attention because the surviving father was Virginia State Senator Creigh Deeds, who bluntly told authorities and the media: “The system failed my son.”23 Political scientist Norman Ornstein, writing in The Atlantic, used the Deeds case as a prime illustration of the “broken mental health system” and observed that “the lack of beds can have tragic consequences.”5
Beyond anecdotal evidence, an emerging research literature has examined the direct and indirect impact of the psychiatric bed shortage on a variety of poor outcomes, including homelessness, crime, incarceration, and emergency room boarding of acutely ill psychiatric patients.1,–,3,6 A longitudinal study of 23,292 previously hospitalized, public-sector patients with a diagnosis of serious mental illness in Connecticut reported that 96 percent of violent crimes in the study population were perpetrated by individuals who had never been involuntarily committed to a hospital, a group ostensibly receiving less inpatient treatment and who did not lose their gun rights through the mental health prohibitor.24
A nationally representative psychiatric epidemiological study described a group of adults with impulsive anger problems and access to firearms, comprising an estimated 8.9 percent of the adult population of the United States. A substantial proportion of these individuals with destructive and uncontrolled anger combined with gun access met criteria for some type of psychopathology (including personality disorders and substance use disorders), but only one in ten had been admitted to a hospital for a mental health problem; the majority with this risky combination of impulsive anger and access to guns would not have lost their firearm rights through involuntary commitment.25
Choe and colleagues26 conducted a meta-analysis to estimate the average prevalence of any interpersonal violence in adults with mental illness identified in different clinical settings. The study reported that, on average, violent behavior within six to 12 months occurred in eight percent of psychiatric outpatients, 13 percent of discharged inpatients, 23 percent of those seen in emergency departments, 36 percent of involuntarily committed patients. Another systematic review found that, on average across studies, 37 percent of first-episode psychosis patients exhibited violent behavior.27
These studies suggest that violence risk in psychiatric patients is not necessarily inherent or persistent but rather a function of fluctuating risk factors that select people into different clinical settings at different moments in the course of their illness. Violence risk tends to be elevated during times of crisis and is most likely to become apparent in periods immediately surrounding contact with the mental health care system during these crises. Involuntary commitment proceedings tend to occur at such times and result in a legal restriction of firearms. Short-term holds for a psychiatric examination also coincide with crises but, in 28 states, do not affect firearms rights.
“Fixing Mental Health” to End Gun Violence
In recent years, public discussion of the “bed-capacity problem” has become embroiled in the politically charged debate over firearm policy in the United States. Prominent voices in the public square increasingly blame mental illness for acts of mass violence and propose addressing deficiencies in the mental health care system, rather than restricting firearm access, as a way to solve that problem.28 In February 2018, after 17 people were shot to death at the Marjory Stoneman Douglas High School in Parkland, Florida, numerous public officials made statements about what must be done to prevent such tragedies in the future. Senator Joni Ernst of Iowa captured the sentiment of many: “The root cause is not that we have the Second Amendment, it's that we're not adequately addressing mental illness across the United States; we need to focus on that.”29
Injury-prevention experts who support gun restrictions based on evidence of risk have pushed back, arguing that facile proposals to “fix mental health” coming from gun-rights proponents are largely a red herring in the debate over mass shootings, if not a calculated distraction from the central problem of how to keep guns out of the hands of people behaving dangerously.30 Mental health consumer advocates, for their part, point to research findings that mental illness accounts for very little interpersonal violent behavior in the population (i.e., about four percent). From their perspective, mental health system reform (while much needed for other reasons) is largely irrelevant to preventing mass shootings or interpersonal gun violence in general.28,31 Moreover, calls to address mass violence with broad-based mental health screening protocols and more psychiatric hospital beds carry a blunt message that “those people” (not “us”) are responsible.11 This only serves to reinforce the stigmatizing stereotype of dangerousness affixed to mental illness in public opinion.31
Research Questions
The politically fraught challenge of how best to prevent rare acts of gun violence by people with serious mental illness invites several research questions: How common are violent crime arrests in the population of adults with serious mental illness who come into contact with the public behavioral health system, and what role do firearms play? To what extent is risk of violent crime increased, or decreased, in persons who are detained in a short-term hold during a mental health crisis but released or hospitalized voluntarily (without losing their gun rights, under most states' laws), compared with those who go on to receive a gun-disqualifying involuntary commitment? Do these patterns of association differ for gun-related and non–gun-related crime outcomes? Specifically, to what extent is a gun-disqualifying involuntary commitment a long-term proxy for increased risk of violent crime, and to what extent is it protective regarding gun crime in particular? In what follows, we address these questions with empirical data.
An Empirical Examination
Sample
The sample is a subset of a study population assembled for a previous study of adults with a diagnosis of schizophrenia-spectrum disorders, bipolar disorder, or major depressive disorder and receiving publicly funded behavioral health services in either of two large Florida counties (Miami-Dade and Pinellas).32 The current study selected 77,048 individuals from the larger study, including those with a record of at least one short-term involuntary hold for examination under the Baker Act (followed by an involuntary placement order, voluntary admission, or release) and a comparison group of similar individuals who had not experienced a Baker Act examination (with or without commitment). Eligible individuals were selected from the Substance Abuse and Mental Health Information System, which included records of services funded through the Florida Department of Children and Families. Records were linked from several other state agency databases, including Baker Act initiations from the Agency for Health Care Administration, psychiatric hospitalization records and commitments from the Substance Abuse and Mental Health Information System and the Department of Children and Families, criminal arrests and convictions from the Pinellas Criminal Justice Information System and Miami-Dade Criminal Justice Information System, death records from the Department of Health, and incarcerations records from the Department of Corrections.
Data were structured as a matrix of person-month observations with a maximum of 168 months per person (January 1998 through December 2011) used in the analysis. Data were merged and de-identified by the Policy and Services Research Data Center at the Department of Mental Health Law and Policy, Florida Mental Health Institute at College of Behavioral and Community Services, University of South Florida. Data sharing agreements were secured, and the data were assembled with institutional review board approval at the University of South Florida. The Duke University School of Medicine institutional review board declared the analysis of de-identified data at Duke to be exempt from review.
Variables
The main outcome variables were arrests for any violent crime, gun-involved violent crime, and non–gun-involved violent crime. Violent crime included homicide, simple assault, aggravated assault, sexual battery, robbery, and kidnapping/abduction. Gun involvement in violent crime was ascertained by a text search for mention of a firearm in arresting charge descriptions or a concurrent nonviolent gun charge.
The key independent variables were short-term Baker Act holds with and without involuntary commitments.33 We analyzed risk associated with these types of events or legal statuses. As mentioned, involuntary commitment disqualified an individual from purchasing or possessing a firearm; a Baker Act examination alone did not, even if followed by a voluntary admission, under Florida law in effect during the time period covered by the study. An individual could receive multiple short-term holds or commitments during the study period. After the first short-term hold, all subsequent person-month observations were attributed to the short-term hold group in the analysis, unless and until the person received a hold resulting in involuntary commitment. After the first involuntary commitment, all subsequent person-month observations associated with that individual were attributed to the involuntarily committed subgroup.
The following time-fixed covariates were used as controls in the multivariate analysis: age, gender, race/ethnicity (i.e., non-Hispanic white, black or African American, Hispanic/Latinx, or other), psychiatric diagnosis (i.e., schizophrenia spectrum disorder, bipolar disorder, or major depression), and co-occurring substance use disorder diagnosis. Models were adjusted for community tenure, a time-varying covariate that measured the proportion of days each month that an individual was residing in the community, neither incarcerated nor hospitalized, and thus assumed to be available for the occurrence of any of the outcomes of interest.
Methods of Analysis
Survival models were estimated using the PHREG procedure in SAS 9.4 (SAS Institute, Cary, NC) to examine the risk of violent crime following a short-term hold only, a hold resulting in involuntary commitment, and a comparison group of similar individuals who did not experience a short-term hold or commitment. Two sets of analyses were conducted. The first set of analyses used the Kaplan-Meier estimator34 to calculate the survival probability that an individual was arrested for a violent crime from the earliest observed month in the data to each subsequent month. This first set of nonparametric models provides a crude estimate of the risks associated with each type of legal status and does not adjust for study covariates. The statistical significance of the difference in survival curves across the two types of legal status was tested with the log-rank test. The confidence band of each survival curve was constructed with the Hall-Wellner method.35 The second set of analyses used competing risks models to estimate the adjusted hazard ratios36 of violent crime arrest, with early censoring of competing events, including suicide, other death, and other gun-disqualifying felony convictions. Here, all available study covariates were included in the model to estimate the conditional effects of legal status on future risk of violent crime arrests.
Study Results
Table 1 displays demographic and clinical characteristics of the study sample as a whole, those who experienced a short-term hold for psychiatric examination but were released or admitted voluntarily, and those who experienced involuntary commitment following a short-term hold. Regarding age and gender, 72.1 percent were under age 44, and 55.5 percent were female. The sample was of diverse racial and ethnic background: 42.2 percent non-Hispanic white, 35.8 percent Hispanic/Latinx, and 20.6 percent black. Regarding primary psychiatric diagnosis, about half the study sample (51.5%) had major depression, 29.0 percent had a schizophrenia-spectrum disorder, and 19.4 percent had bipolar disorder. Co-occurring substance use disorder was identified in 14.0 percent of the sample. Information regarding substance use disorder was available only if listed as a treatment diagnosis. Epidemiological studies suggest that the true prevalence of alcohol and drug use disorders in adults with serious mental illness is higher. For example, a recent systematic review reported that 42 percent of individuals with schizophrenia have a co-occurring substance use disorder, on average across studies.37
Sample Characteristics by Legal Status Group
Short-term holds and involuntary commitments were significantly associated with being male, younger than 44 years of age, white, having a diagnosis of schizophrenia, and having a concurrent substance use disorder. All of these differences were statistically significant at p < .0001 based on two-sample proportional tests. Compared with people with a short-term hold only, those who were involuntarily committed were also more likely to be male, younger than age 44, white, and with a diagnosis of schizophrenia. All these differences were significant at p < .0001 based on two-sample proportional tests.
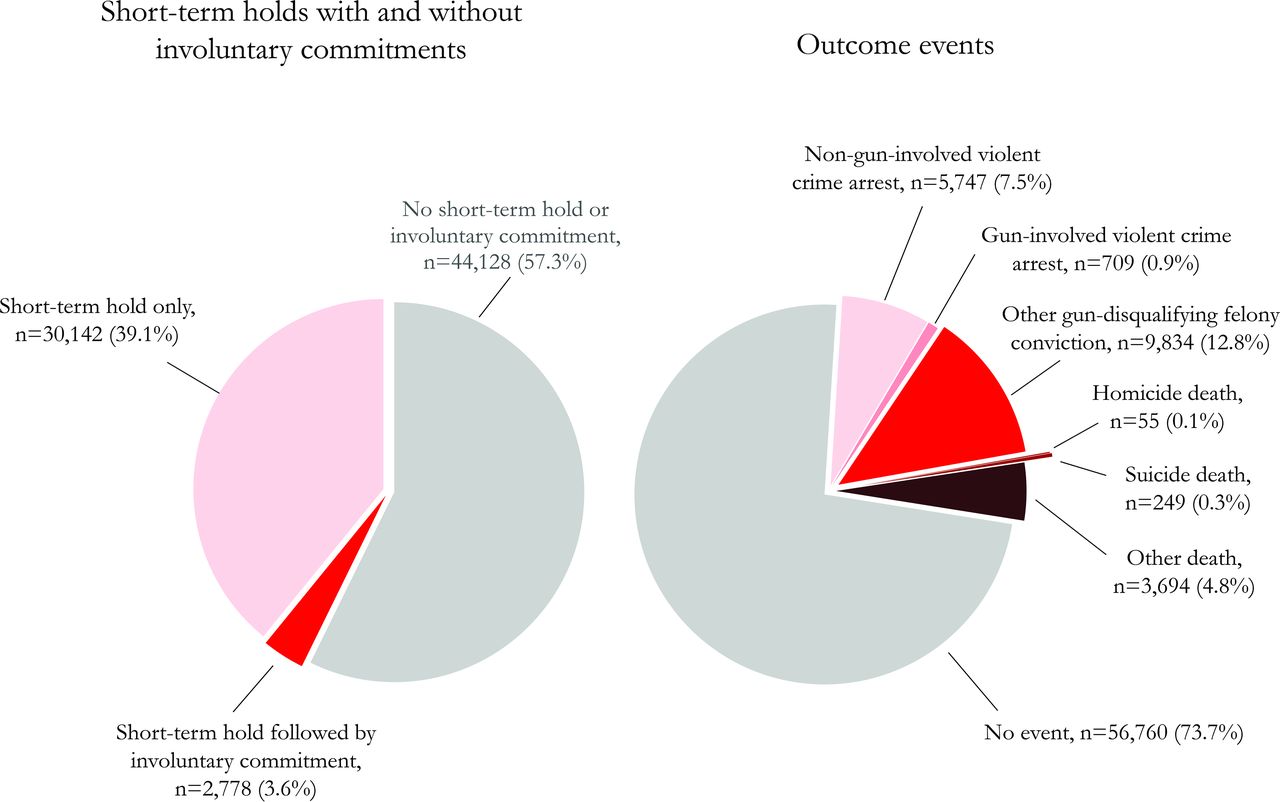
Figure 1 displays the distribution of the sample by legal status and adverse outcomes of interest, including violent crime arrests, with and without gun involvement. It also shows deaths and other gun-disqualifying felonies, which were treated as censoring events in the survival analysis. Notably, 249 individuals (0.03%) died of suicide and 55 (0.01%) were victims of homicide over the period of the study. The majority of the sample (57.3%) experienced neither a short-term hold nor involuntary commitment, and the proportion who had only a short-term hold was larger than the subgroup who were involuntarily committed by a factor of 10 (39.1% versus 3.6%). The majority of the study sample (73.7%) did not experience any of the adverse outcome events of interest. Only 0.9 percent of the study sample was arrested for a gun-involved violent crime, while 7.5 percent were arrested for a non–gun-involved violent crime.
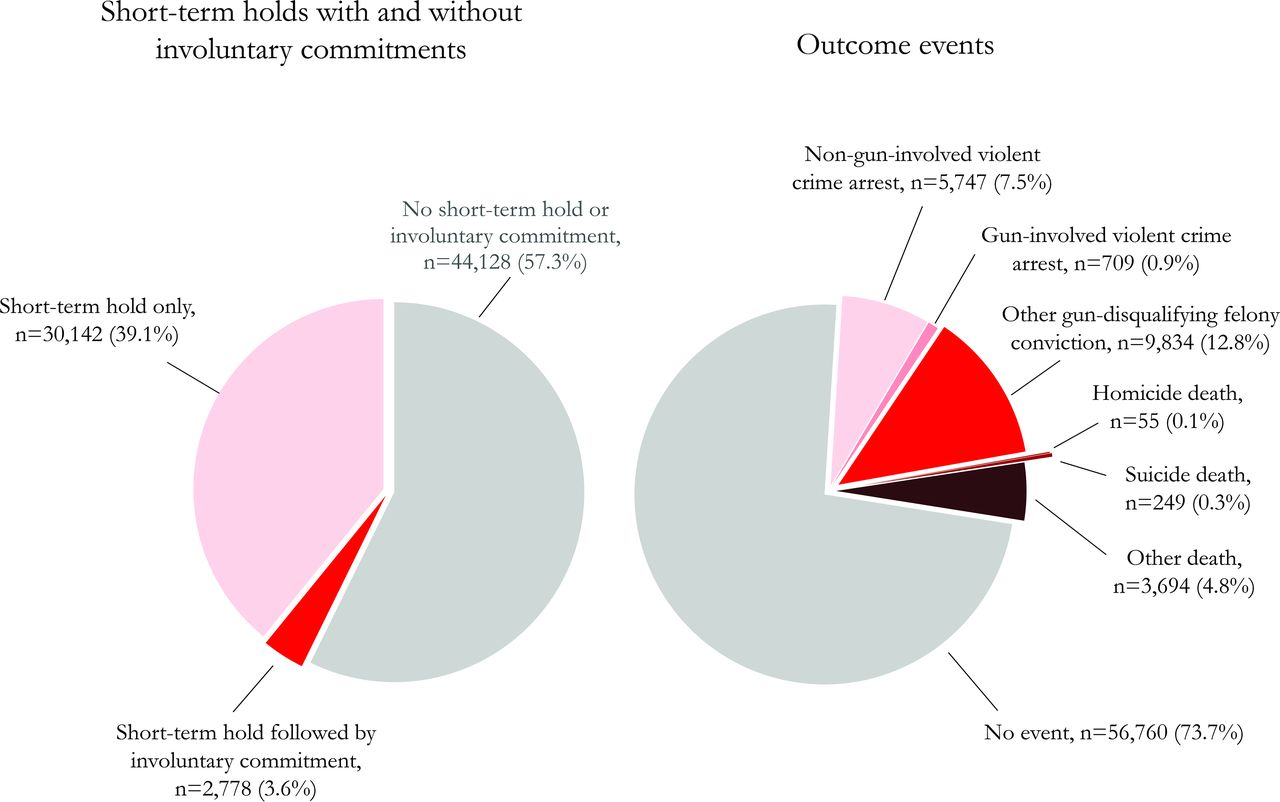
Distribution of sample by legal status and outcome events over the study period.
Among the study population of 77,048, 149 individuals (0.2%) were arrested for a homicide over the years of the study period, and firearms were involved in 44 (29.5%) of these homicide cases. Of the 5,747 persons in the study sample who were arrested for non–gun-involved violent crimes, 105 (1.8%) were charged with homicide; by contrast, of the 709 individuals arrested for a gun-involved violent crime over the study period, 44 (6.2%) were charged with homicide. Thus, guns made violent crime more lethal: among all violent crime arrests, the offenses involving guns were more than three times more likely to be homicides than those not involving guns. Overall, homicide perpetration was rare in the sample, although it was significantly more frequent than in the general population of Florida adults. The annualized estimate of 15.8 per 100,000 is more than twice the average homicide rate of the general population of Florida during the study years (5.7 per 100,000).38
Guns were implicated in less than one-third of homicides in the study population. Of the group arrested for homicide using a gun, 50.0 percent had a history of at least one short-term involuntary hold, but none had been involuntarily committed. Of those arrested for homicide not involving a firearm, 46.7 percent had a history of at least one short-term hold, and 3.8 percent had been involuntarily committed. Viewing the data differently, of the individuals who were arrested for homicide after a gun-disqualifying involuntary commitment, none used a firearm in their crime; all used other means.
More specifically, a total of 2,778 individuals with an involuntary commitment record were observed in the data for an average of about seven years (88.7 months); during that period, four were arrested for a non–gun-involved homicide, and none was arrested for a gun-involved homicide. By comparison, a total of 30,142 individuals with only a short-term hold history were observed for an average of about six years (71.1 months); 49 were arrested for a non–gun-involved homicide and 22 were arrested for a gun-involved homicide. The crude rates of non–gun-involved homicide arrest are similar in the two legal-status groups: 16.3 per 10,000 for the involuntarily committed group and 14.4 per 10,000 for those with only a short-term hold history. The rates for gun-involved homicide arrest, however, were markedly lower in the involuntarily committed group than in the short-term-hold group (0 per 10,000 compared with 7.3 per 10,000, respectively.)
Statistically significant risk factors for a homicide arrest in this sample included being young (age 18–43), male, having a diagnosis of schizophrenia, and being black (all p < .0001). Notably, however, the analysis could not control for a variety of unobserved socioeconomic, environmental, or life-historical risk factors that would have been correlated with both race and homicide, explaining the association between the two factors in these data. Also, due to the infrequency of homicide events, we could not fit a conditional hazard model of homicide risk as a function of commitment status adjusted for covariates.
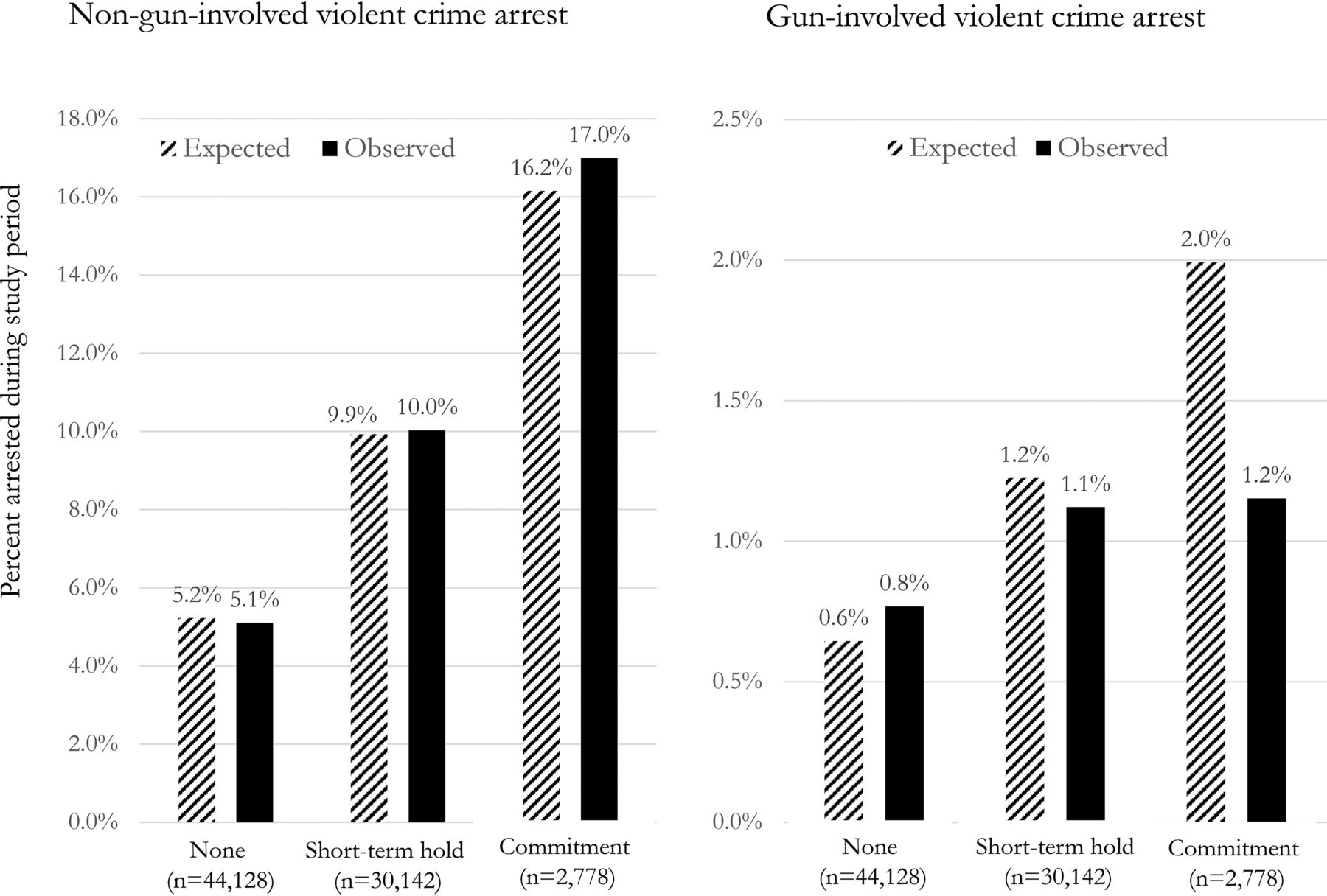
Figure 2 displays the unadjusted prevalence of all gun-involved and non–gun-involved violent crime arrests by legal status. The figure also shows the rates that would have been expected under the assumption that the distribution of violent crime by commitment history is proportionally the same for gun-involved and non–gun-involved violent crimes. The observed prevalence pattern for non–gun-involved violent crimes by legal status closely adheres to the expected prevalence rates based on the observed distribution for all violent crimes: individuals with involuntary commitment records had significantly higher arrest rates than those with only a short-term hold record (p < .0001), who in turn had significantly higher arrest rates than those with no short-term hold or commitment history (p < .0001). This overall pattern is consistent with the fact that dangerousness to others or self is a criterion for commitment. A marked variation in the expected pattern can be seen in the rates of gun-involved violent crime, however, as the arrest rate for those with an involuntary commitment record was substantially lower than the expected rate at p = .0159 (equating to an estimated difference of 24 violent crime arrests for the group over the follow-up period) and did not differ significantly from the arrest rate for those who experienced short-term holds only (p = .2313). These data can also be configured to show that the percentage of violent crime arrests that involved guns was significantly lower among those who were involuntarily committed than among those who were not committed (6.3% versus 10.1%; p = .0467).
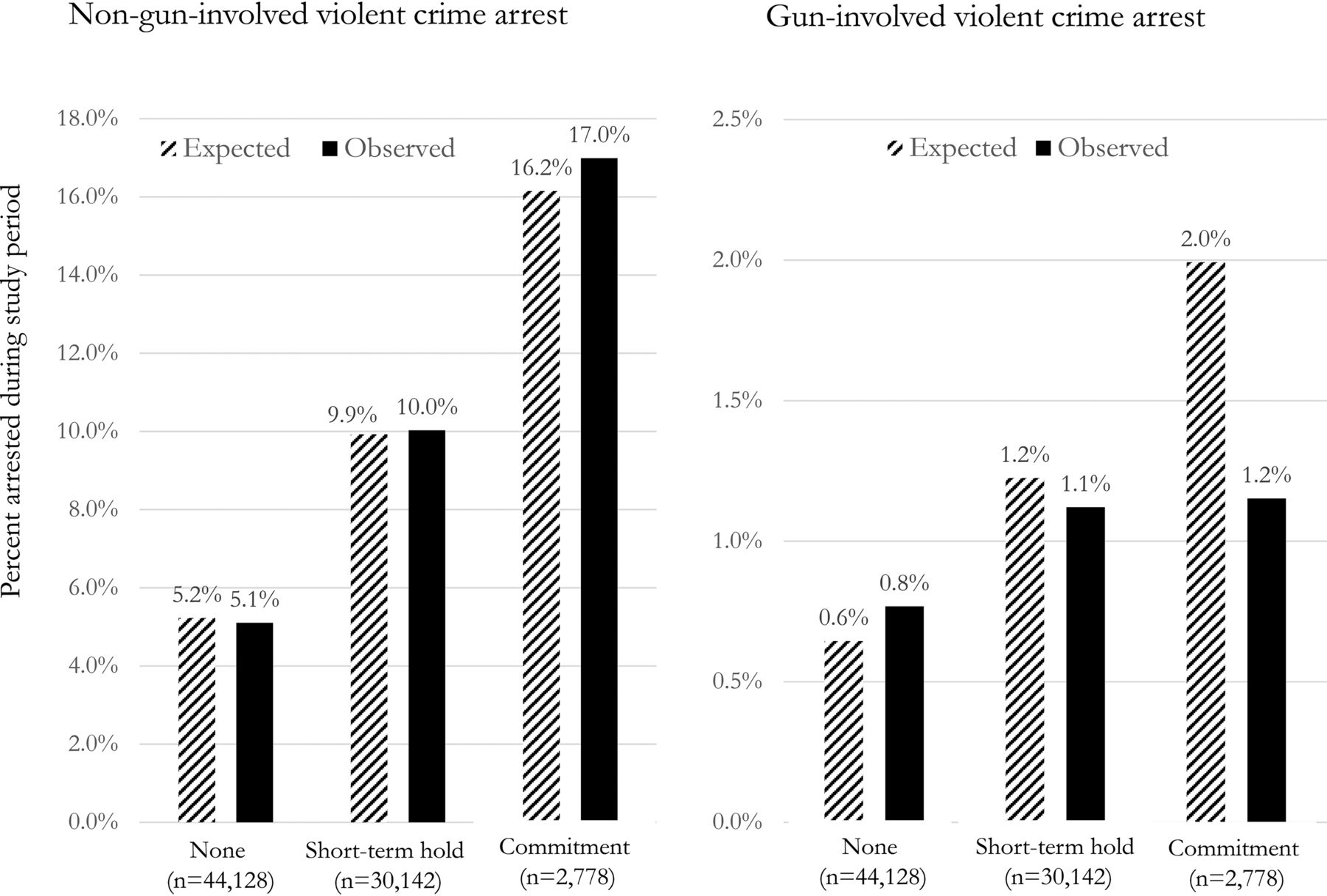
Expected and observed occurrence of non–gun-involved and gun-involved violent crime arrests following short-term hold with and without involuntary commitment, and neither status.
Figure 3 displays the Kaplan-Meier curves, survival probabilities of not getting arrested for any violent crime across the 168 months of the study period for the three legal status categories. These curves did not adjust for study covariates. Results indicate that being involuntarily committed was associated with the highest risk of violent crime arrest over time, followed by having a short-term hold record. People with neither a short-term hold nor involuntary commitment had the lowest risk of violent crime. The differences across the three survival curves were statistically significant at p < .0001 based on the log-rank test.

Kaplan-Meier survival curves for any violent crime by legal status, 1998–2011.
Table 2 presents the results of three longitudinal risk models predicting arrest for any violent crime, gun-involved violent crime, and non–gun-involved violent crime. These models estimated hazard ratios associated with involuntary commitment and short-term holds versus neither of those legal statuses, adjusting for demographic and clinical covariates. Having a record of either a short-term hold or an involuntary commitment significantly increased the risk of future arrest for any violent crime, compared with having neither of these statuses (hazard ratio = 1.84, p < .0001; and hazard ratio = 1.25, p = .0027, respectively.) In these models adjusting for covariates and removing censored observations, the hazard ratios were higher for the involuntary-hold-only group than for the involuntarily committed group. The same pattern was seen in the model predicting arrest for non–gun-involved violent crime (hazard ratio = 1.86, p < .0001, for involuntary holds, and hazard ratio = 1.29, p = .0012, for holds followed by involuntary commitment). The pattern differed in the model predicting arrest for gun-involved violent crime, however. In that model, only a short-term hold was a significant net predictor of gun-involved crime (hazard ratio = 1.55, p < .0001), whereas involuntary commitment history (a gun-disqualifying status) did not significantly predict an increase in gun-involved crime. Figure 4 summarizes these hazard ratio results graphically.
Risk Factors for Violent Crime Arrest, by Gun Involvement in Crime
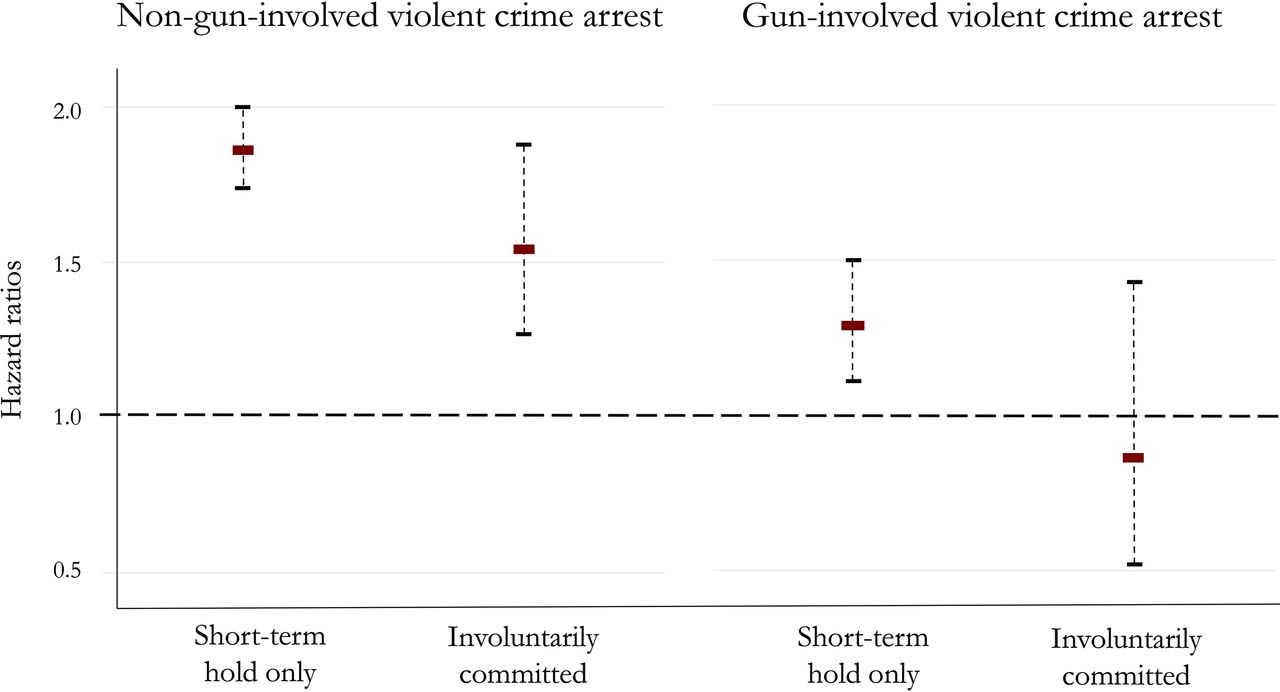
Hazard ratios (95% CI) for violent crime arrest by gun involvement and legal status.
Implications for Safety and Stigma
Most Significant Findings
This research is the first empirical examination of the long-term risk of gun-related and other violent crime in a large population of adults with serious mental illness, followed over multiple years subsequent to their hospitalization under a gun-disqualifying involuntary civil commitment order, in comparison to similar individuals with the same diagnoses who received only a brief psychiatric hold for evaluation. A key lesson from the study is that any violence-prevention policy that is focused on people with serious mental illness and starts with involuntary civil commitment will have a limited population impact for at least two reasons: people with serious mental illness contribute little to the overall problem of violence in the first instance, and few of them get committed (3.6% of the current study group followed over multiple years). By contrast, a much larger proportion (39.1%, in this study) experience a short-term hold, which in most states is not a gun-disqualifying event.
Our results indicate that the occurrence of arrests for firearm-involved violent crime, including homicide using a gun, was less frequent than expected in the small minority of the sample who experienced a gun-disqualifying involuntary commitment. Even though violent crime arrests occurred more often in the committed group in the unadjusted model (Fig. 3), the proportion of these charges that involved guns was significantly lower than among charges against individuals who were not committed. Having a record of a short-term hold with or without involuntary commitment was associated with a significantly increased risk of future arrest for any violent crime. Having a record of only a short-term hold, however, was a significant net predictor of gun-involved crime, while involuntary commitment history (a gun-disqualifying status) was not associated with a significantly increased risk of gun-involved crime. A consistent pattern was seen regarding homicide in particular. The rates of non–gun-involved homicide arrest were similar in the two legal status groups, but the rates specifically for gun-involved homicide arrest were markedly lower in the involuntarily committed group than in the short-term-hold group. An important caveat is that the study was conducted in a single state, Florida, which has an unusually high number of short-term holds for examination not resulting in involuntary commitments.15
A previous analysis of this study population32 described 254 suicide cases that were identified in matching death records. While the study group had a suicide rate approximately four times higher than that of the general population in Florida, firearms were involved in only 20 percent of these suicide cases compared with 48 percent of suicides in the Florida population. Similarly, the current study analyzed violent crime outcomes, including homicides, and found that 149 individuals in the study group (about one fifth of 1%) were charged with a homicide at some time over the study period. This finding equates to an annualized rate of homicide approximately twice as high as that of the general population of adults in Florida (15.8 versus 5.7 per 100,000 population). In line with our earlier report on suicides, however, arrests for homicide in the study group were less than half as likely to involve firearms than homicides in the general population of Florida adults (29.5% versus 67.2%).39 This was also consistent with our previously reported finding that the overall arrest rate for violent crime was higher in the study group than in the Florida population, but not for gun-involved crime in particular.32
It is important for two reasons not to interpret the homicide rate in the study population as evidence that “mental illness causes murder.” First, 99.8 percent of those with the same psychiatric diagnoses in the same dataset were not arrested for a homicide. Second, as persons receiving mental health services in public systems of care, these individuals likely had other risk factors for crime that were not observable and could not be accounted for in our analysis. Such factors, which are not directly related to psychopathology, could include poverty, social disadvantage, unemployment, residential instability, substance abuse problems, previous involvement with the criminal justice system, exposure to neighborhood violence, or history of violent victimization.40
Interpreting the Key Finding
There are at least three potential interpretations or explanations for the finding that gun-involved crime arrests occurred less frequently than expected in persons who experienced involuntary commitment. First, it is likely that involuntarily committed individuals received more intensive treatment in the form of extended hospitalizations; this could have mitigated their subsequent risk of engaging in violent behavior. That interpretation, however, fails to explain why such an effect would be observed only for gun-involved violence and not all violent crime arrests. Second, it could be that involuntary commitment selects for individuals who are less likely to acquire firearms for a variety of reasons, ranging from greater disability associated with psychopathology to having lesser financial means to purchase guns and perhaps limited access to social networks that could assist them in obtaining firearms. It is worth noting, however, that the entire study sample was selected using the same criteria (i.e., all had the same range of disorders and received services in the same public mental health systems) and that the hazard models were adjusted for basic demographic and clinical covariates. There may have been clinical comorbidities, such as antisocial personality disorder, that were not available as control variables. The third potential explanation is simply that involuntary commitment conferred a legal disability to purchase or possess firearms under federal and state law in Florida, thereby limiting gun access differentially in the committed group. In any event, the pattern in these results is at least consistent with a hypothesis that involuntary commitment and the hospital treatment that accompanies it can exert a protective effect in regard to gun-involved violent crime in particular, including homicide.
Beyond “Dangerous Guns or Risky People”
These findings have implications for mental health policy at the intersection with a national debate about preventing gun violence. Policy questions about how best to reduce gun violence in the United States are often oversimplified in today's political climate, reduced to a polarizing choice between limiting access to guns and incapacitating or coercively treating dangerous people. As a result, many good-faith policy efforts to improve the care continuum for adults with serious and disabling mental health conditions are now saddled with political baggage arising from the tension between these competing perspectives.
Public-health-minded proponents of more robust gun regulations have scientific evidence on their side,41 but efforts to implement such solutions for people in mental health treatment settings are fraught with the risk of unintended consequences and misunderstanding. Mental health service providers and policymakers face complex challenges in their ambiguous roles of treating people with serious mental illness in confidential therapeutic settings and meeting societal expectations to somehow protect the public from gun violence.42 Hospital-based treatment, when needed, certainly should be made more available to adults with serious mental illness,16,43 but not primarily to prevent mass shootings and other violent crime.28 Still, improving access to intensive treatment (based on clinical need) and limiting access to guns (based on behavioral indicators of risk) might be complementary strategies.
Evidence-based policy solutions are sorely needed to improve treatment access and to reduce the risk of adverse outcomes for adults with serious mental illness in the community. These solutions should include the judicious use of legal tools to leverage treatment when appropriate, along with serious public reinvestment in a continuum of services. Yet policies in the mental health sphere are hardly the place to start to build a comprehensive policy to reduce gun violence. The large majority of people with serious mental illness, including most who are hospitalized under involuntary civil commitment orders, are never violent. Involuntary civil commitment involves a consequential deprivation of liberty; it is a legal tool that should continue to be used sparingly, and only in cases where inpatient treatment truly is needed to mitigate a dangerous mental health crisis in persons who are unwilling or unable to consent voluntarily to such an intervention.7 That being said, the findings of this study also suggest that the gun-disqualifying feature of involuntary commitment can be protective, specifically in terms of preventing gun-related crime, in a way that a short-term hold alone may not.
Twenty-two states (as of 2016)8 had enacted laws that limit legal access to firearms, at least temporarily and with due process, for persons detained in a short-term hold; such a hold requires that a clinician has found that the patient poses an elevated risk of interpersonal violence or self-injury. Other states could follow suit and adopt such a policy in line with expert recommendations.41,44 At the same time, states should provide a meaningful and expedient opportunity for legal restoration of gun rights to persons who no longer pose a risk.18 In sum, these new research findings suggest that preventing gun violence and improving clinical outcomes for adults with serious mental illness in the community are very different problems with some overlapping and potentially synergistic policy solutions.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2020 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}
{kind=link}
{kind=link}