


Abstract
Since 2004, Connecticut has had two different mechanisms for involuntary medication of defendants hospitalized for restoration of competence to stand trial. In this article, we first describe the development of these two mechanisms and compare their procedural elements. The first procedure required a hearing in criminal court, in a process parallel to the subsequent U.S. Supreme Court holding in Sell v. United States; the later procedure uses a civil mechanism in probate court and was enacted in response to the dicta in Sell regarding the preferential use of alternate mechanisms for involuntary medication orders. To compare the effectiveness and efficiency of the two mechanisms, we examined 1,455 admissions to the state's secure forensic hospital for competency restoration for the calendar years 2005 through 2011. Petitions for involuntary medication of defendants were filed in five cases in criminal court (0.3%) and in 177 cases (12.2%) in probate court. The probate mechanism resulted in a significantly shorter duration of the resolution of the competence matter. Both mechanisms were effective at restoring defendants' competency (i.e., two thirds were restored by the criminal court process, and nearly 74% were restored in the civil process).
- competency restoration
- involuntary medication
- Sell v. United States
- probate court
- Connecticut General Statutes
- length of stay
Prior to late 1993, Connecticut General Statutes included the following provisions: “Voluntary patients may receive medication or treatment but shall not be forced to accept unwanted medication or treatment…. Involuntary patients may receive medication and treatment without their consent, but no medical or surgical procedures may be performed without the patient's written informed consent.”1
By that time, however, it had been years since psychiatrists in Connecticut practiced according to this standard that any involuntary patient could be involuntarily medicated, even though it was still officially permitted legislatively. The reason was the shift in national standards of practice in this area since the 1970s,2 following several right-to-refuse-treatment cases3,–,6 and especially following the Rogers decisions7,8 in Massachusetts, by which involuntarily hospitalized patients could no longer be presumed to be incompetent to make treatment decisions.
No case law or statutory law guided how the process of seeking medication over objection should occur in Connecticut. A group of lawyers, advocates, judges, and psychiatrists met for several years to try to fashion such a legislative mechanism, without success. The psychiatrists argued for a treatment-driven approach, based on some version of a second or independent opinion; the legal advocates argued for a rights-driven model with a jury trial as the vehicle for making the final determination of competence to refuse treatment. When legislative leadership grew impatient with the lack of progress in these efforts, pressure was exerted to force a quick compromise between the parties.9 The result consisted of two independently available mechanisms for seeking medication over objection, one roughly akin to each of the two previously advocated positions.10 One mechanism, related to the rights-driven model, was a probate court hearing for the appointment of a conservator of person with authority to make decisions on behalf of a patient who was unable to give or withhold informed consent to medication. The conservator was to consider several factors in reaching such decisions, including risks and benefits of medication, prognosis with and without medication, and the preferences and religious views of the patient.
Unfortunately, the new legislation specifically excepted patients committed for restoration of competency to stand trial under Connecticut General Statutes § 54-56d from the new procedures, referring to procedures set forth in the competency statute, which consisted only of language stating that “the court shall order placement of the defendant for treatment for the purpose of rendering him competent.”11 There were no specific provisions in the competency statute regarding procedures for treatment over objection. Although this concern was raised by the leadership of the forensic hospital to which all competency restoration patients were admitted, the informal response was that such specific procedures were unnecessary because no one would question the hospital's ability to medicate criminal defendants over their objection who were sent to the hospital specifically for treatment to restore their competence to stand trial. It took less than four months for that speculation to be tested, ultimately all the way to the Connecticut Supreme Court.12
Jose Garcia was charged with murder in January 1993. In September 1993, he was found not competent to stand trial and sent to the hospital for restoration. Mr. Garcia refused medications, and the hospital ultimately filed a report to the court opining that he would not improve to the point of competence to stand trial without administration of antipsychotic medications. The hospital made an unprecedented request for an order from the court to involuntarily medicate Mr. Garcia, essentially asking the trial court to create the missing procedures via case law, or at least to interpret the meaning of “placement … for treatment for the purpose of rendering [the defendant] competent.”11 Additional context for the request was the recent U. S. Supreme Court decision in Riggins v. Nevada,13 which noted that “the State might have been able to justify medically appropriate, involuntary treatment with the drug by establishing that it could not obtain an adjudication of Riggins' guilt or innocence by using less intrusive means” (Ref. 13, p 135). The request for a court order thus anticipated a potential ruling on what might constitute the kind of “overriding justification” that the Riggins Court held was constitutionally necessary in medicating an incompetent defendant over objection.
The trial court initially ordered involuntary medication in January 1994, leading to further hearings and appeals while the order was stayed. The Connecticut Supreme Court heard oral arguments in the case in January 1995 and released its decision in May 1995,12 drawing upon the U.S. Supreme Court involuntary medication cases of Washington v Harper (1990)14 and Riggins (1992).13 The court found that Mr. Garcia had a liberty interest founded in the substantive due process clause of the Fourteenth Amendment, which may not be infringed unless “(1) the administration of the drugs is ‘medically appropriate’; and (2) the state demonstrates an overriding justification for doing so” (Ref. 12, p 964). The court then noted the Harper finding that “[i]dentifying the contours of the substantive right remains a task distinct from deciding what procedural protections are necessary to protect that right” in a given situation (Ref. 12, p 964, quoting Harper, p 220). Riggins had offered little guidance about procedural safeguards. The Connecticut Supreme Court identified not only liberty interests but also general privacy interests of a defendant in such circumstances, and outlined the procedural due process necessary to override those interests:
In order for a court to authorize the involuntary medication of an incompetent defendant to render him competent to stand trial, therefore, the state must demonstrate that: (1) to a reasonable degree of medical certainty, involuntary medication of the defendant will render him competent to stand trial; (2) an adjudication of guilt or innocence cannot be had using less intrusive means; (3) the proposed treatment plan is narrowly tailored to minimize intrusion on the defendant's liberty and privacy interest; (4) the proposed drug regimen will not cause an unreasonable risk to the defendant's health; and (5) the seriousness of the alleged crime is such that the state's criminal law enforcement interest in fairly and accurately determining the defendant's guilt or innocence overrides the defendant's interest in self-determination. The state, moreover, must demonstrate each of these factors by clear and convincing evidence (Ref. 12, pp 966–67).
Observing that “a defendant's medical interests may diverge from his legal interests and, therefore, that representation by counsel may be insufficient to protect adequately an incompetent defendant's medical interests,” the Connecticut Supreme Court also ruled that in most circumstances a trial court should also appoint a “health care guardian to represent the defendant's health care interests to the court” (Ref. 12, p 969); this may not be necessary if the defendant is competent to make health care decisions, despite incompetence to stand trial. Although the trial court had previously utilized much of this analysis, it had not found each of the five factors by clear and convincing evidence, nor had it considered the appointment of a health care guardian (HCG), and thus the case was remanded for further determinations in light of these rulings. These rulings were later adopted into law by the Connecticut General Assembly in 1998.15
These procedures were thus already in place by the time of the U.S. Supreme Court decision in Sell v. United States (2003).16 The five Garcia factors in Connecticut are very similar to the factors announced by the Supreme Court in its holding in Sell regarding necessary procedures for involuntarily medicating a non-dangerous, trial-incompetent defendant (see Table 1). Thus, when Sell was decided, the Connecticut General Assembly was more interested in responding to its dicta than to its holding because major details of the latter had already been enacted. The dicta addressed the notion that alternative grounds for medicating an incompetent defendant may be preferable and are typically addressed as a civil matter, including states' procedures for appointment of guardians with decision-making authority regarding medications when a patient lacks the capacity for informed consent (Ref. 16, p 182).
Sell Factors and Garcia Factorsa
Thus, the Connecticut General Assembly was interested in applying a procedure to incompetent, medication-refusing defendants that was akin to its civil procedures for medicating hospitalized patients involuntarily. It adopted a medication override process for incompetent criminal defendants parallel to that for civil inpatients in 2004.17 See Table 2 for a comparison of the two legislative methodologies.
Procedures in Connecticut for Involuntary Medication
Under the new procedures, if a patient sent to the hospital for treatment to restore trial competence is believed to be incapable of giving informed consent to medication that is deemed necessary to treat the patient, the hospital may apply to probate court for the appointment of a special limited conservator (SLC), who would have the authority to give or withhold consent to medications for the patient. The probate court may appoint an SLC if it finds by clear and convincing evidence that “the patient is incapable of giving informed consent to medication for the treatment of the patient's psychiatric disabilities and such medication is necessary for the patient's treatment.”18 The SLC is required to meet with the patient and the physician and to review the medical record, and then to consider “the risks and benefits from the medication, the likelihood and seriousness of adverse side effects, the preferences of the patient, the patient's religious views, and the prognosis with and without medication.”18 The SLC is authorized to give or withhold consent for 120 days, which may be extended, or until the competence matter is resolved in criminal court, thus making this type of conservatorship both “special” and “limited” when compared with the civil proceedings from which it was adapted.
The new legislation went into effect on October 1, 2004. What follows is a report on the collection of seven years of data on the use of this “Sell hearing” procedure, as it is referred to by practitioners in Connecticut, compared with the earlier “Garcia hearing” procedures, which are now often referred to as “Sell hearings” elsewhere in the United States. To avoid confusion, we will hereafter refer to the post-Garcia procedures in Connecticut as criminal court hearings or procedures, and to the post-Sell procedures in Connecticut as probate court hearings or procedures.
For patients admitted after the SLC statute was available, the practice at the hospital was to first seek SLC appointment through the probate court when a patient is unwilling to voluntarily accept needed psychiatric medications for treatment in restoration cases. Requests are made to the criminal court for appointment of an HCG only when the SLC petition is denied, save for one exception (i.e., Patient Doe), which will be discussed in the Results section. The goal of this study was to compare the effectiveness and efficiency of the two legal mechanisms in resolving the question of competence to stand trial.
Methods
The population studied were patients at the Whiting Forensic Division of Connecticut Valley Hospital, who were committed to the hospital by criminal court order for treatment to restore competence to stand trial. Connecticut Valley Hospital is the major state psychiatric hospital for the state of Connecticut. There are 91 beds in the maximum-security building of the Whiting Forensic Division, used for a variety of forensic and civil patients. Fifty-eight of these beds (on three treatment units), plus an additional unit of 24 beds in a separate lower-security building, are used mostly for court-ordered competency restoration. These units also house patients admitted under criminal court order for various statutory evaluations. Thus, 82 beds across both buildings are primarily focused on short-term hospital stays for competence restoration.
According to statute, when the competency of a defendant is called into question, there is a preliminary evaluation by a team working from the Office of the Commissioner of Mental Health and Addiction Services. Their findings and recommendations are then presented to the superior court where the criminal matter is being heard. From 2008 to 2011, there were an average of 590 screenings per year, and an average of 195 cases per year that resulted in a finding of not currently competent with a recommendation for inpatient treatment. All these patients were brought to the Whiting Forensic Division for inpatient care. According to statute, a defendant can be kept in a restoration-to-competency status for the time of the maximum potential sentence if convicted, up to a maximum of 18 months. After the maximum time is expired, the patient can be returned to the hospital for a hearing in the probate court for possible civil commitment or can be released directly to the community. There is one probate court for the district that includes Connecticut Valley Hospital. Therefore, all petitions for SLC and for possible civil commitment come to the same court.
The study population consisted of defendants who faced a broad range of charges, from misdemeanors carrying a potential sentence of three months incarceration, to serious felonies that could result in 60 years of incarceration. Defendants came from nearly all superior court jurisdictions within the state. The diagnoses of these patients were all serious disorders, including schizophrenia, schizoaffective disorder, bipolar disorder with mania, delusional disorder, and major depression with psychotic features. Almost all patients for whom an SLC was appointed received antipsychotic medications. Some received long-acting depot preparations of antipsychotic medications. Some received mood stabilizers, either as a primary medication or as an augmenting strategy.
The SLC statute went into effect on October 1, 2004. Because the probate court was easier to access and more experienced in handling involuntary medication petitions, we hypothesized that the Whiting Forensic Division would no longer use the criminal court procedures; that there would be an increase in the number of cases with orders for involuntary medication in competence to stand trial restoration cases; and that there would be a decrease in the time from admission to disposition of the competency to stand trial matter in involuntary medication cases.
The current study examines the defendants remanded for competency restoration during the calendar years 2005 through 2011. We wanted to only include defendants for whom the SLC statute was in effect for the entirety of their hospital admission. We therefore chose to begin the study with defendants admitted after January 1, 2005.
For those patients who were the subject of a petition to probate court for the appointment of an SLC, we studied the days from admission to the probate court hearing and from the date of the probate court hearing until disposition of the competency matter. We examined three possible dispositions: the petition is denied; the petition is granted and the defendant is restored to competency; and the petition is granted and the defendant is found not restored to competency. For the patients in the denied group who were the subject of a subsequent petition to criminal court for the appointment of an HCG, we measured the time from SLC denial to criminal court hearing and from criminal court hearing to resolution, to evaluate parallel processes without adding the time spent on SLC denial to the time taken in the HCG process.
The study proposal was reviewed by the State of Connecticut Department of Mental Health and Addiction Services Institutional Review Board and found to be exempt from further institutional board review on July 24, 2012, based upon the criteria of 45 Code of Federal Regulations 46.101(b)(4). The study proposal was also reviewed by the Human Investigation Committee of Yale University and found to be exempt from their review on September 26, 2012, based upon the criteria of 45 Code of Federal Regulations 46.101(b)(1).
Results
The passage of the SLC statute had a profound impact on practice in the hospital. In the 12-month period prior to October 1, 2004, there were three patients for whom an application was filed for HCG in criminal court. In the 12-month period after October 1, 2004, there were two HCG applications in criminal court and 20 applications for SLC in probate court; the two HCG applications were for patients admitted prior to the availability of the SLC statute on October 1, 2004, who are therefore not included in the study population. During the study period, there was only one year with more than one HCG application in criminal court (Table 3).
CSTR Admissions and SLC Petitions
There were 1,455 patients admitted from 2005 through 2011 on court orders for treatment to restore competence to stand trial. The average daily census for patients in a restoration-to-competency status during the study period showed a general downward trend over time ranging from 67 (2005 and 2007) to 48 (2011).
Out of that competency-to-stand-trial restoration group, there were 177 patients (12.2%) for whom petitions were filed in probate court for SLC appointment, comprising our main study population. The percentage of competency restoration patients for whom SLC was sought each year varied over the study period, ranging from 9.5 percent (2009) to 16.9 percent (2011). There were five HCG applications in criminal court during the seven-year study period, an average rate less than one fourth of that in the year prior to initiation of the probate court procedures. Each of the HCG petitions followed SLC applications denied by the probate court (Table 3). It is important to note, however, that the criminal court hearing is not an appeal of the probate court hearing decision; they are separate mechanisms, guided by different criteria. The criminal court hearing is based on restorability, whereas the probate court hearing is based on the inability to give informed consent and the necessity of medication for the patient's treatment (compare the right columns of Table 2 and Table 3). Demographic information for the total probate court petition group is provided in Table 4.
Demographic Information of Special Limited Conservator Study Group
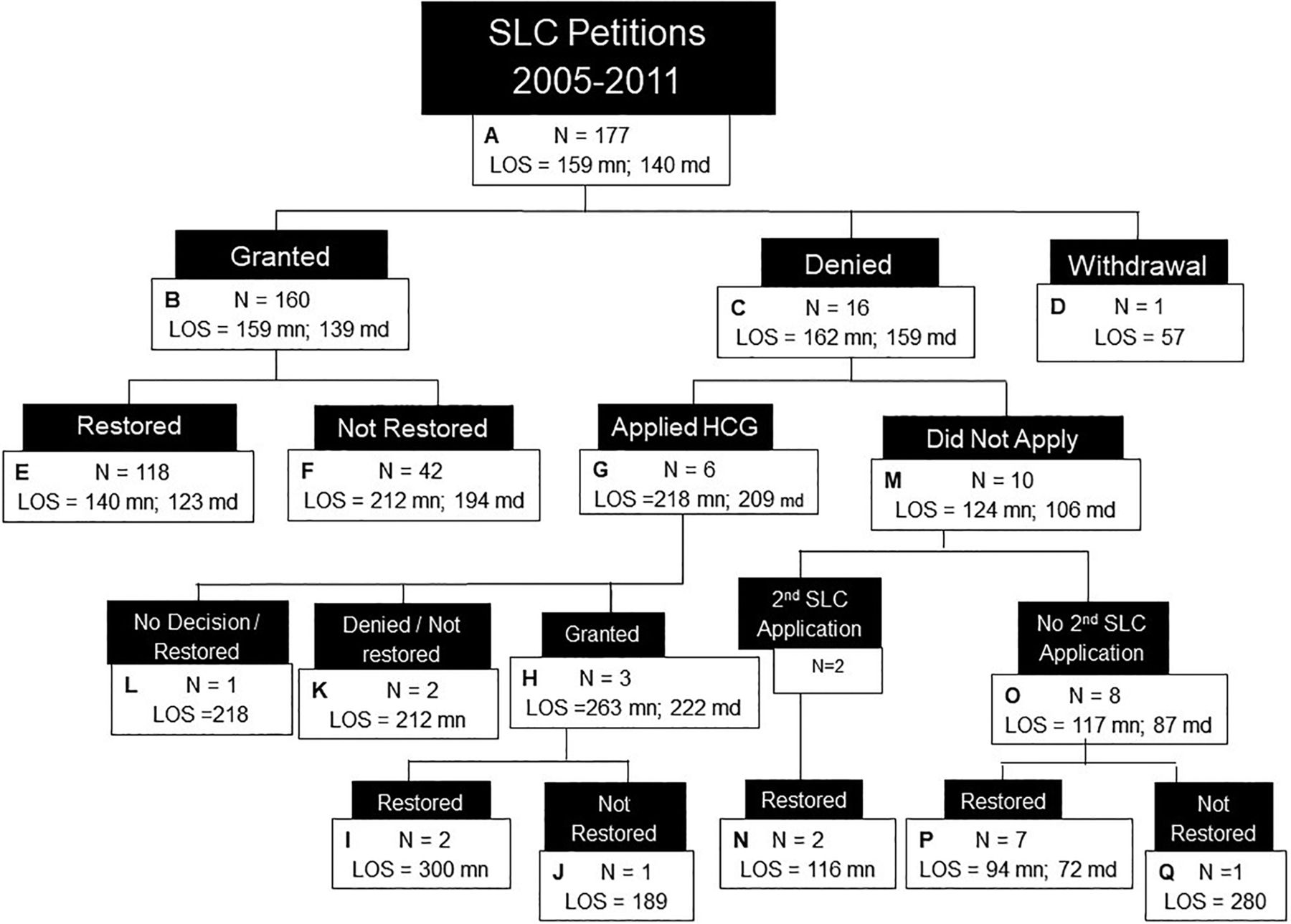
The flow diagram of SLC (probate court) and HCG (criminal court) cases is displayed in Figure 1. Of the total of 177 SLC petitions filed (Box A), 160 (90.3%) of them were granted (Box B). Of those SLC petitions granted, 118 (73.8%) resulted in a criminal court finding that the defendant's competence to stand trial had been restored (Box E). In the one case where the SLC application was withdrawn (Box D), the patient agreed to take medication prior to the hearing and showed subsequent positive response to treatment. The patient was restored in 57 days.
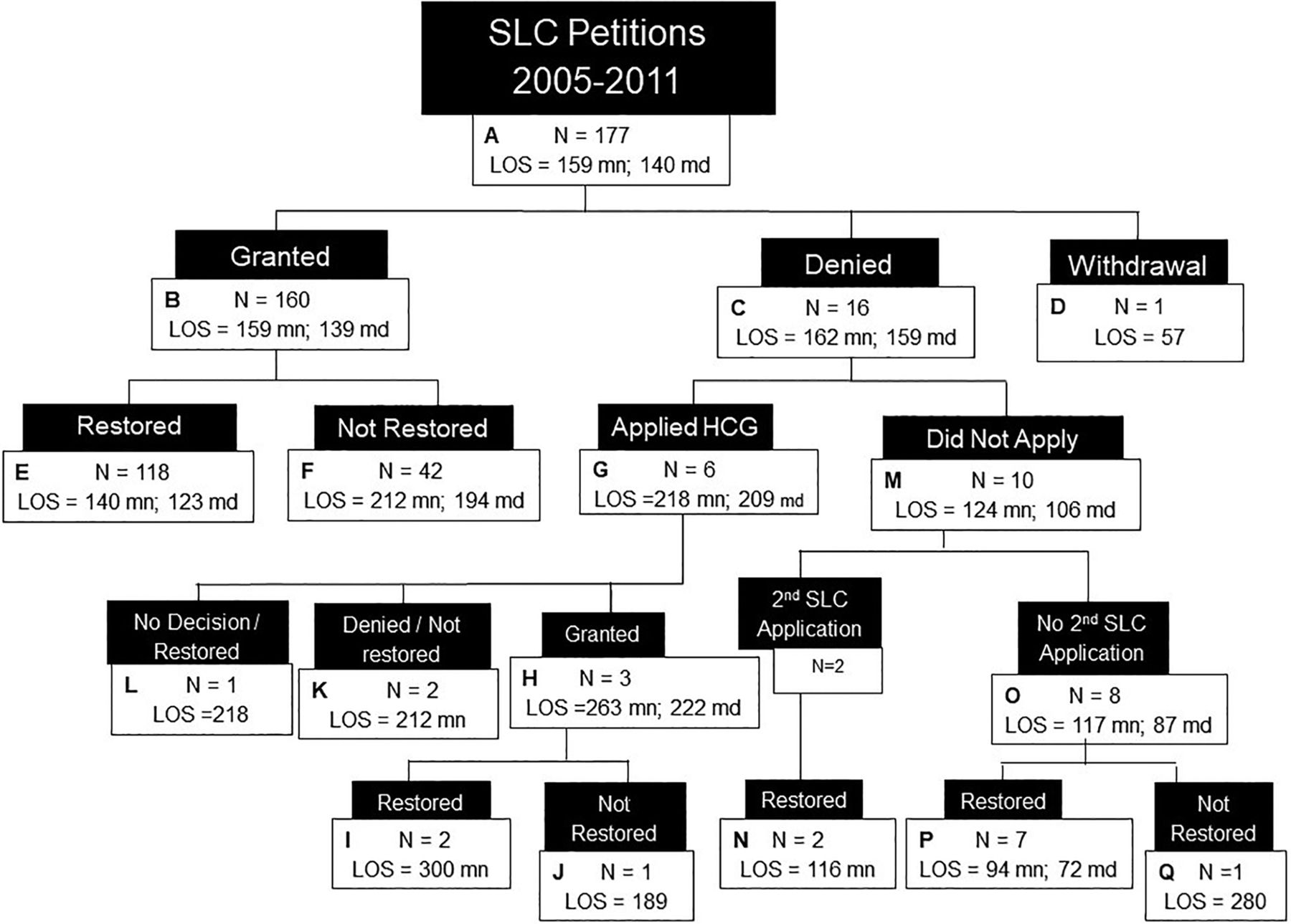
Special limited conservator and health care guardian petitions and restoration of competency to stand trial. SLC, special limited conservator; HCG, Health Care Guardian; LOS, length of stay.
In six of the 17 cases in which SLC was denied by the probate court, the hospital asked the criminal court to appoint an HCG (Box G), believing the statutory criteria for such an appointment could be met. Three of those requests were granted (Box H), of which two were restored after involuntary medication treatment (Box I) and one was found not restorable (Box J). The latter was granted an HCG, but the court never authorized involuntary medication treatment. In another HCG application, the court never rendered a decision about appointing an HCG, but the patient began taking medication voluntarily after the hearing and was ultimately found restored (Box L). In the last two HCG applications, the applications were denied, and the patients were found unrestorable (Box K). One of these two cases involved Patient Doe, whose situation is described below.
In 10 of the 16 cases in which SLC was denied, the hospital did not pursue HCG (Box M). In two of these 10 cases, a second application for SLC was made and approved; both individuals were subsequently found restored (Box N). In the other eight SLC-denial/non-HCG cases, no further SLC appointment was attempted (Box O); seven of these individuals were nonetheless ultimately found restored to competence to stand trial (Box P). This means that clinicians were found to be wrong 3.9 percent of the time (7 of 177 cases) in opining that competence could not be restored without medication (see Discussion). In one of the seven cases, the patient took some medication, which was the reason the SLC petition was denied. Ultimately, the patient reluctantly agreed to a change in medication and was restored after 101 days of hospitalization. If this patient is removed from the calculation, the demonstrated error rate of opining that medications were necessary to competence restoration drops to 3.4 percent.
The case of Patient Doe is a complicated exception to the practice of seeking SLC application as the first step in pursuing involuntary medication. Patient Doe had been denied SLC in probate court and denied HCG in criminal court in one case and had been discharged as not restorable. Three weeks later another court jurisdiction ordered a competency restoration admission for a different set of charges. The hospital chose to proceed directly to HCG application in criminal court in the second admission. This case thus falls outside of the universe of the 177 SLC petitions shown in Figure 1 and is not included in the data analysis, but is nonetheless illustrative of how complicated the HCG process can be. The petition for appointment of an HCG was granted 55 days after admission, and the order for involuntary medication was given by the court another six weeks later. The order was stayed pending appeal, which went to the state's highest court. During the pendency of the appeal, the time allowed for restoration was tolled. The Connecticut Supreme Court affirmed the trial court's order more than 22 months after the original order for involuntary medication. Patient Doe never received involuntary medication; after a two-and-a-half-year admission, Patient Doe was found competent, sentenced, and discharged.
Of the 165 cases in which some form of involuntary medication was authorized by a court, 122 individuals (74%) were restored (Boxes E, I, and N). For the criminal court group, two of the three individuals were restored. For the probate court group, 120 of 162 were restored (74%; Boxes E and N).
The median number of days from admission to a probate hearing for the total SLC petition population (n = 177) was 43. This time period was its shortest in the first year (31 days), increasing for the next several years (peaking at 53 days in 2009) before returning to 31.5 days in 2011. The median number of days from probate hearing to final disposition of the competency question in criminal court was 84. In 2005, this value was 75 days; it spiked to 136.5 in 2006 and gradually returned to the original levels in 2010 and 2011.
The total time from admission to legal disposition of the competency matter, referred to as length of stay (LOS), for all probate hearing patients had a median value of 120 days in 2005, peaked at 187 days in 2006, and dropped gradually to 117 days by 2011. The median value for the seven-year study period was 140 days (Table 5).
Median Number of Days from Admission to Competence to Stand Trial Disposition
For the patients who were ultimately restored to competence to stand trial, these numbers are slightly lower: 116 days in 2005, peaked at 171 days in 2006, and decreased to 114 days by 2011, with a median value for the entire study period of 123 days. For the patients who had SLCs appointed but were not restored, the median numbers were substantially higher with a different pattern than those illustrated thus far: 250 days in 2005, 297 days in 2006, 178 days in 2011, and 194 days for the entire study period. The median LOS for all the patients for whom SLC application was made from 2005 to 2011 was 140 days. For the 16 patients whose SLC applications were denied, the LOS to disposition had a median value of 159 days.
There were only two patients brought back to probate court for a second SLC application; both were approved, and both were restored (Box N). The LOS for these two patients were 91 days and 140 days. The median LOS for those restored on the first SLC attempt was 123 days. Thus, the LOS for these two patients were relatively short considering that their scenarios included two separate SLC hearings. The patient with the 91-day LOS reached the first probate hearing in about six weeks and the second hearing three weeks later, and the patient was restored after three weeks of treatment with medication. This rapid response to treatment was about two months shorter than the median length of time from SLC approval to restoration (77 days) for the SLC restored group (n = 118). The second patient (LOS = 140 days) went to the first SLC hearing one month after admission, to the second hearing one month later, and was restored six weeks after the SLC was approved. The quicker-than-average response to treatment made up for the time spent pursuing two separate SLC applications in this case.
The timeframes (in median days) between various stages of the involuntary medication legal proceedings for the relevant subgroupings of the SLC population are noted in Table 6. The increased duration of restoration via the criminal court process compared with the probate process (Box I versus Box E, Figure 1) is not due to differences in the amount of time taken to get to the probate hearing for the two groups. In fact, the HCG restored group had a slightly shorter time to the probate hearing than the SLC restored group (36 days versus 39 days). It also has little to do with differences in time from medication approval to resolution of the competence-to-stand-trial matter (i.e., the treatment component of the process). The median days from the HCG hearing and approval of involuntary medication to disposition (i.e., 91 days) is only two weeks longer than the time from SLC hearing to disposition (77 days). The difference in LOS between the two groups is found in the amount of time it took to get to the HCG hearing following the SLC denial (median of 173 days). Compare this to the much shorter median time from admission to SLC hearing for the restored group (i.e., 39 days).
Timetable for Stages of Involuntary Medication Proceedingsa
The significant difference noted above between median LOS for SLC patients who were restored and not restored is accounted for by both stages of the probate process (Box F versus Box E). The median time to probate hearing is 10 days longer for the not restored group (49 days versus 39 days). This may mean that earlier SLC applications tend to be made in cases in which the clinical benefit of medication for the patient is more obvious and thus more readily recognized and acted upon. In part, this may also represent prior experience with patients who have been treated in the facility before, although those data were not collected in this analysis. The time from probate hearing to disposition is longer for the not restored group by a full two months (137 days versus 77 days).
Discussion
Involuntary medications, via either legal method, were substantially effective in restoring competence to stand trial. Two of the three criminal court patients were restored, and 74 percent of the 162 probate court patients were restored. But the probate process is a more efficient mechanism for restoration than the criminal court process.
One observation to note from Figure 1 is that the median LOS for patients restored via the probate process (123 days; Box E; n = 118) is significantly shorter than the median LOS for probate patients who were not restored (194 days; Box F; n = 42) (Mann-Whitney U = 1,215.5, P < .001). This makes sense clinically given that patients who do not have a positive initial response to involuntary medication will generally be tried on other or additional medications and for a longer time in pursuit of achieving a positive response.
One limitation of this study is the small number of criminal court procedure cases, as predicted in our first hypothesis. This warrants caution in reaching conclusions about the differences between that group and the probate group. Denials of SLC applications can occur for various reasons, which may signify distinctions with the group for whom SLC is granted. For example, the patient with the longest LOS (Box P, 178 days) was denied SLC by the probate court because the patient was cooperating to some degree with medication efforts. The probate court denied SLC for the patient in Box Q (LOS 280 days), expressing concern over permitting involuntary medications given the low level of the patient's criminal charges. Although this factor is not found in the SLC statute, the probate judge applied rulings in Harper,16 Garcia,14 and Sell1 in interpreting the statute.19
Although the SLC-granted group is larger, it is also heterogeneous. The granted group contains 42 patients (26%) who were not restored and had longer LOS as noted above, thus increasing the average LOS for the granted group. The denied group includes seven different final subgroups (Boxes L, K, I, J, N, P, and Q) of restored and non-restored patients from three different pathways, each with small numbers: HCG application made; second SLC application made; and no application for HCG or second SLC attempt (Figure 1).
The study results demonstrate an error rate of 3.4 to 3.9 percent in opining about restoration without involuntary medication. It is not possible, however, to determine whether any of the patients who were involuntarily medicated might have been restored without the medication; thus, this error rate could be higher. Our subsequent clinical experience with these patients and their response to medication treatment leads us to believe, however, that few might have improved without medication sufficiently to be found competent.
Conclusions
Our hypothesis that following the implementation of the SLC statute the hospital would no longer use the HCG process was incorrect, but it was not misguided. In fact, the hospital used the HCG process in only 0.3 percent of all competency restoration cases during the study period. The probate process was used 35 times more often (in 12.2% of cases). This finding lends support to Slobogin's argument that the consideration of incompetence to make treatment decisions as a factor in involuntary medication decisions for incompetent defendants (as advanced in the dicta in Sell) “comes close to rendering Sell irrelevant” (Ref. 20, p 1533). The availability of the quicker probate procedures made application for involuntary medication to the criminal court unnecessary in all but six percent of restoration cases in which the patient declined to accept medication.
These findings about the utility of the SLC procedures may be relevant to other jurisdictions' consideration of the application of Sell1 to their current statutory schemes. For example, the Wisconsin Supreme Court recently found their existing statutory scheme unconstitutional in allowing criminal courts to order involuntary medication to restore competency to stand trial based on incompetence to accept or decline medication without findings related to the four Sell factors.21 Because the civil process created by the Connecticut General Assembly does not have as its purpose the restoration of competence to stand trial, it avoids the constitutional problem cited by the Wisconsin Supreme Court.
One advantage to the criminal court procedure in Connecticut is that an amendment to the statute in 2007 allowed the court to authorize continued involuntary medication of the defendant to maintain competence after a finding of restored competence and transfer back to either jail or hospital to await trial.22 Because this is not possible for the probate court procedure, where the involuntary medication order ends when the competence matter is resolved, treatment teams may have to consider going to the criminal court procedure first in cases where historical data suggest a defendant may decline continued medication if returned to corrections to await trial.
Our hypothesis that the number of orders for involuntary medication in competency restoration cases would increase is supported by the data. The first year following implementation saw a seven-fold increase in petitions filed; the number of petitions remained elevated, with more than 90 percent being granted.
The hypothesis that the new process would lead to decreased LOS is also supported by the data, with a significantly shorter LOS for patients restored via the SLC process compared with the HCG process. The probate court holds hearings every week and is experienced with psychiatric testimony, the factors involved in medication override decisions, and the required procedures. It takes much longer to docket a hearing in the criminal courts, which rarely hear such matters. The probate court process is the more efficient of the two available mechanisms.
There are other potential avenues for future research related to the probate process. One is to examine the numbers and rates of defendants found not competent and not restorable over several years prior to and after the implementation of the SLC statute to assess whether the availability of the civil procedures decreased the numbers of unrestorable defendants. Another would be to compare the LOS for the probate and criminal court processes to the LOS for individuals restored with voluntary treatment. An extension of these endeavors would examine the risks of not restoring patients to competence to stand trial, such as the percentage of such patients who are civilly committed (and for how long and at what cost) and their criminal recidivism rates once discharged to the community.
Footnotes
Dr. Norko is involved in the editorial leadership of the Journal; however, he did not participate in any aspect of this article's review and acceptance. Dr. Norko and Ms. Hollis acknowledge the support of the Connecticut Department of Mental Health and Addiction Services.
Disclosures of financial or other potential conflicts of interest: None.
- © 2020 American Academy of Psychiatry and the Law





{kind=link}