


Abstract
The Royal College of Physicians and Surgeons of Canada has recently introduced a new model of training for residents and fellows in all specialties and subspecialties, including forensic psychiatry. This model, Competence by Design, is intended to improve the training of residents with the goal of increasing the competence of practicing specialists. In the Competence by Design model, training is broken down into four distinct phases. Residents prompt their supervisor proactively when they are ready to be assessed on a specific task, and the feedback is specific and corrective. A resident's performance of each designated task is reviewed by a competency committee, which decides when the trainee is ready to move on to the next phase. In this article, we review some of the problems with the current model of training and explore how this new model will improve upon this training. We anticipate that this model will prove effective at improving training in forensic psychiatry.
In Canada, all specialty medical training is overseen by the Royal College of Physicians and Surgeons of Canada (RCPSC), which is responsible for both accreditation, like the Accreditation Council for Graduate Medical Education (ACGME), and examination and certification, like the American Board of Psychiatry and Neurology (ABPN). In April 2011, after many years of hard work by stewards of forensic psychiatry in Canada, the College, as it is known, granted forensic psychiatry specialty status, allowing for formalized oversight of training programs. This prompted a transition from informal fellowships to a formal, one-year, post-graduate year 6 (PGY-6) training program dictated by the College.
As in the United States,1 the initial iteration of forensic psychiatry training in Canada has traditionally followed the time-based model of medical training. This traditional model has several problems that affect the quality of physician education. The RCPSC decided a new model was needed that would not only provide quality education to physicians but also address the increasing public concern about the competence of specialists. An outstanding example of incompetence occurred in the field of pathology, involving Dr. Charles Smith. Although Dr. Smith lacked forensic pathology training and even a basic knowledge of forensic pathology, he appeared as an expert witness in multiple high-profile cases in the 1990s. He became an advocate for the prosecution, misleading the court on his knowledge and expertise, criticizing other experts, and providing speculative and unsubstantiated opinions. This resulted in at least 12 wrongful convictions in child and newborn deaths. Dr. Smith was found to have committed such egregious errors as to prompt a public inquiry in Ontario.2 The inquiry, released in 2008, reviewed not only Dr. Smith's work but the state of the profession. Other specialties watched this with a certain schadenfreude, although with enough insight to know that none were above reproach.3
To address these concerns, like many international jurisdictions, the College decided to launch a new model of training for specialty programs: Competence by Design (CBD). In this article, we review the evolution of the Forensic Psychiatry Subspecialty Residency Training Program in Canada, starting with its inception and moving toward the upcoming transition to CBD.
The Traditional Model of Training
As highlighted by the RCPSC,4 the same system of medical training has existed in Canada since the first Faculty of Medicine was founded in 1829 at McGill University in Montréal. Around 1880, the “Father of Modern Medicine,” Dr. William Osler, moved medical education from the laboratory to the bedside, instituting the foundations of our current medical education system. Prompted by stark inconsistencies in educational standards across Canada and the United States in the early 1900s, the first routes of accreditation were the Dominion Medical Council of Canada founded in 1912 and the RCPSC founded in 1929. This allowed for unified oversight of the educational standards for specialty medical training in Canada. The RCPSC still fulfills this role.
The history of psychiatric training in Canada has been well described.5,6 Psychiatry was first recognized as a medical specialty by the RPCSC in 1944. National standards of training were established through the Objectives of Training (OTR), Specific Standards of Accreditation (SSA), and the Specialty Training Requirements (STR) organized through the CanMEDS framework.7 These standards have been regularly updated to keep up with societal needs and advances in psychiatric knowledge. There has been no associated updating of pedagogic methods and evaluation, however, to match the scientific advances in this area. Instead, the old model of time-based training has been maintained, assuming that the acquisition of knowledge and skills is directly proportional to time. This has meant a five-year psychiatry residency in Canada.
In Canada, traditional general psychiatry residencies include some learning objectives related to forensic psychiatry, and some rotations can be completed in forensic psychiatry, but obtaining experience in the forensic psychiatry subspecialty is not mandatory. Similar deficits in ACGME-accredited programs in the United States have also been noted.8,–,10 While the ACGME requires some experience in forensic psychiatry, they limit this to risk assessment, decisional capacity, civil commitment, and involuntary treatment.1,11 When forensic experience is available, it can be quite variable.12,13 This has been identified by residents as a major deficit that has resulted in limited knowledge and skills in forensic areas relevant to all psychiatrists. To address these deficits in ACGME programs, several resources are now available.9,10,14 In addition, in Canada, the lack of forensic experience has been hypothesized to have reduced interest in subspecialty training in forensic psychiatry and likely increased the stigmatization of our patients.12,15
Prior to 2011, Canadian subspecialty training in forensic psychiatry involved informal fellowships of a few months to a year or more (Bradford J, personal communication, 2020). Some trainees sought out specific preceptors, while others sought broader experiences. Interested parties completed general psychiatric training and then extended it in informal fellowship positions, which were funded by a variety of sources. There were no formal requirements, although individual programs designed educational syllabi. Training varied significantly by length, learning objectives, areas covered, landmark cases, and many other areas. There were usually only a few fellows per year nationally.
Given the lack of standardized training, it was recognized that moving to an accredited forensic psychiatry subspecialty through the RCPSC would help to ensure standardized rotations and learning objectives among trainees. Key forensic academics in Canada16,–,18 advocated with other subspecialties, and ultimately a working group was formed by the RCPSC to launch the subspecialty. In 2011, the training requirements (STR, OTR, and SSA) were completed, culminating with the launch of the subspecialty in April 2011.
A one-year PGY-6 (fellowship) training was developed to address the forensic psychiatry subspecialty. As with all time-based training, the experience includes time spent in certain forensic rotations, augmented by lectures (didactic half-day per week), and other learning experiences. The training covers core criminal forensics with selective experiences in civil forensics, correctional psychiatry, research, sexual behaviors, advanced risk assessment, and child and adolescent forensic topics. The final rite of passage is a short-answer examination, which is standard for RCPSC subspecialties.19 Since the inception of the subspecialty, seven accredited programs have been launched in Canada. Although this represents a significant improvement in the standardization of training, some concerns remained, which prompted a search for a new model of training.
Problems With the Traditional Model
While time-based accredited training has long been the traditional model for most medical training, including psychiatry and forensic psychiatry, there are significant problems with this model. Many of these have become apparent with the growth of research on medical education. One concern about the time-based model, in which residents undergo five years of residency training, is that it is unclear when a resident should proceed to the next level of education. Within these residency years, there is no clear trajectory of educational experiences. There is an idea that residents may need some experience in a certain part of the field and some experience in another, but this is rarely expressed in an organized manner. Residents are also not provided with clear expectations of what they need to achieve before moving on to their next educational experience. There are no good data on whether the residents have mastered their present level of education. Even if there were, there is no forum for discussion about the progress of the resident.
Another concern is that educational decisions tend to be based on clinical service needs rather than the educational needs of the resident. Residency placements tend to be guided by the OTR/STR minimum standards of the College but are influenced locally by clinical service needs and the availability of supervisors. Progression through the program tends to be determined by single assessors who are often primary supervisors and may have particular biases. Under the current model of education, some supervisors may also be inexperienced or reluctant to offer regular and timely critical feedback.
In addition, residents might not take advantage of necessary learning experiences if they are not aware that they are expected to practice and become competent in these tasks. Rare cases might be missed when priority is given to routine service. There may be a tendency to approach experiences as a checklist, meaning that residents spend more time observing than actually practicing a skill, with the expectation that they will learn by osmosis. Residents could also be faced with clinical situations without having the appropriate competencies to recognize or manage them.
While time-based training has some practicality for funding and service planning, there is another significant problem related to the assessment of and feedback given to the resident. One of the seminal papers on competency-based training20 highlights the now well-known “Miller's pyramid” (Fig. 1). Medical education focuses on the assessment of knowledge (i.e., what a resident knows) rather than a workplace-based assessment of competence (knows how to do), performance (shows how to do), and action (does). Miller further discussed specific recommendations for how to assess these levels of competence.21
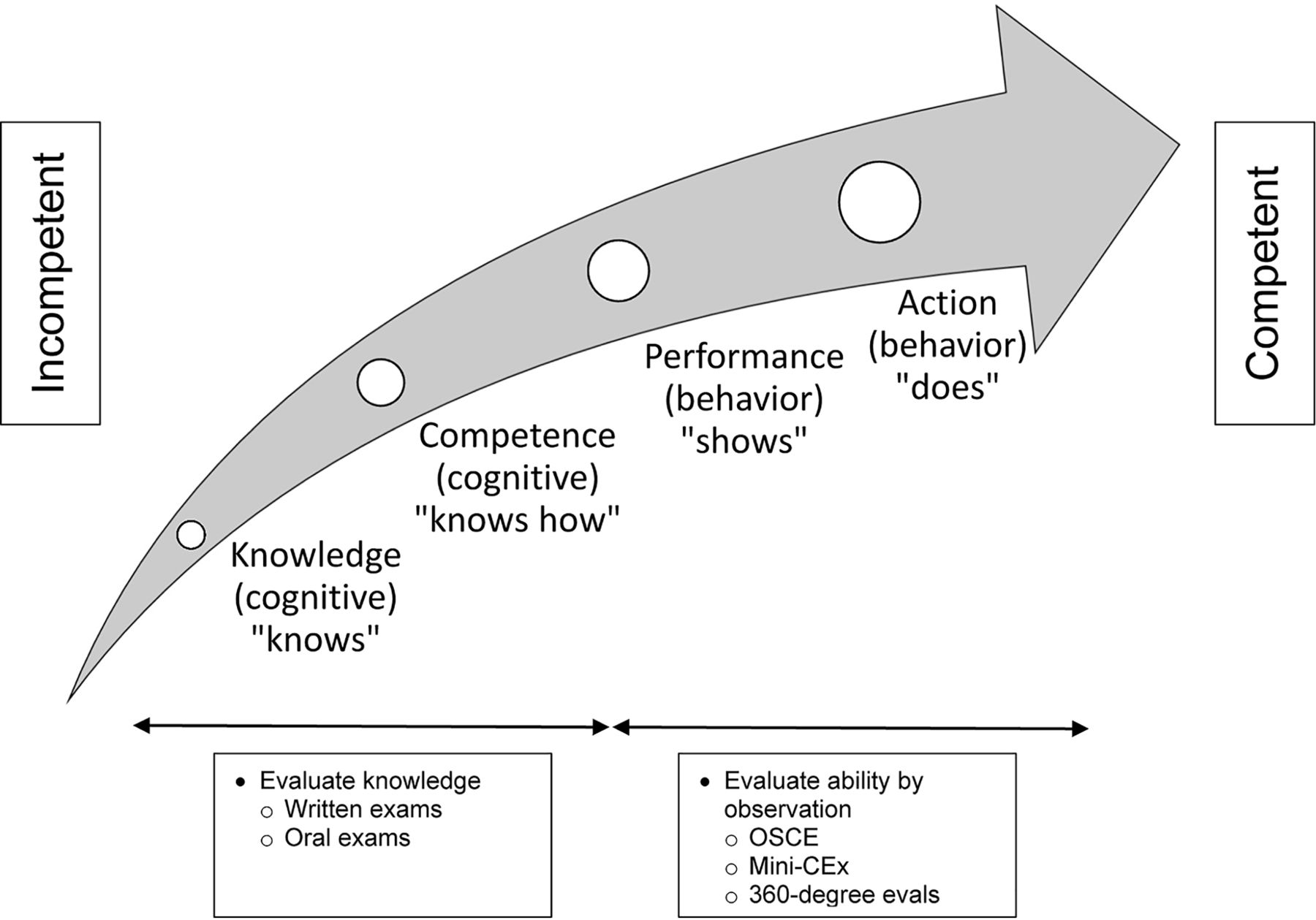
Progression to competency as a forensic psychiatrist based on Miller's Pyramid of Competence.20 OSCEs = objective structured clinical examinations; CEx = clinical evaluation exercise.
Given the service focus of some training, medical residents can easily complete most of their training without being observed or receiving feedback other than in a final written examination. Many of the fundamental physician skills of communication, patient interaction, time management, professionalism, and leadership are not formally observed or assessed, leading to a failure to recognize residents who are struggling early and a failure to provide appropriate remediation. In addition, by allowing struggling residents through, good residents often do not receive the feedback required to become great residents. There is some research literature22 on giving feedback. It suggests that feedback is traditionally given only at the end of the rotation when it is too late to apply any corrections or make practical changes in response.
Traditionally, we have not decided conceptually what we want residents to be required to learn to become competent physicians. Ginsburg et al.23 noted that supervisors expected the following: first, that a resident could be trusted to manage an emergent situation; second, that the resident be adaptable to a changing situation; third, that the resident make the supervisor's life easier; and finally, that the trainee “just get it.” In forensic psychiatry, supervisors would likely say that they want a resident to be able to perform an appropriate assessment interview, write an acceptable report, give expert testimony in a suitable manner, and manage the rehabilitation of mentally abnormal offenders.
Despite these criticisms, Canadian medical schools, as well as those the world over, have generally turned out fairly competent doctors using the traditional methods. The question that has been posed is whether medical training can be improved. It is hoped that CBD is one way in which to achieve such improvements.
Traditional Methods of Assessment
Regarding assessment methods for residents, the medical establishment has long relied on testing learners outside of, but not necessarily in, the clinical setting by a variety of means. These methods have primarily included multiple-choice questions, which have developed into objective structured clinical examinations (OSCEs). Both methods have been established over the decades and have some psychometric support24 if the principles are followed. Focal, circumscribed assessment of performance in clinical contexts has also been developed and has been well received.25 The Mini-CEx, for example, involves direct observation of a learner in a clinical situation with a real patient.
The most common assessment instrument is the In-Training Evaluation Report (ITER), which is a long, end-of-rotation, omnibus evaluation addressing all CanMEDS competencies. These competencies were devised in the 1990s and developed around the framework encompassing the role of physicians as professionals, communicators, scholars, collaborators, health advocates, and leaders.7 Residents are rated in these areas in relation to whether they have satisfied expectations for the objectives of training in forensic psychiatry. The ITER has been criticized for a number of reasons. Primarily, it has been noted to perform poorly psychometrically.26 This is perhaps related to the fact that this assessment is done at the end of each placement and is a high-stakes gatekeeper entity. Therefore, even if the system allowed for the simple administration of the remediation consequences, there would be no time or opportunity to perform them.
In addition, supervisors are often unwilling to record bad ratings. Bogo and colleagues27 note that personal and relational ties make it difficult for a supervisor to fail a learner with whom they have shared experiences over the past many months. This has been termed a “failure to fail.”28 Regehr et al.29 conclude that it is important to develop an administrative structure and prepare faculty for the challenges of assessment. This should be linked to the development of assessment tools that allow supervisors to communicate feedback that is formative and educational. In other words, feedback that is corrective and improves performance is required to facilitate learning.
The challenge we are facing is how to provide good data to determine when a resident can move on to the next stage of education. To arrive at valid educational decisions based on the competence of the learner, we require a forum for discussion based on good assessment.
Competence by Design
Competence by Design (CBD) is a major educational initiative aimed at strengthening the traditional curriculum. In response to the problems surrounding the traditional time-based model of training, key stakeholders in Canadian medical education, including the RCPSC, set about modernizing medical education in Canada by adapting the principles of an international movement known as competency-based medical education (CBME) for the Canadian context. This work was finalized by the Future of Medical Education project.30 One of the main recommendations of the project was a move from time-based training to competency-based training utilizing some concepts similar to those in the American Milestones project.1
While traditional Canadian medical resident education continues to be hosted within a set timeframe, the principles of CBD are designed to graduate trainees who are better prepared for independent practice. Additionally, the goal is to produce graduating physicians who meet the needs of Canadian society and enhance patient care by improving trainee learning and assessment. To accomplish these goals, the emphasis in training is on performance-based assessment methods. These methods include increasing direct observations and feedback from supervisors, collecting multiple points of data to determine resident promotion to more independent stages of training, and implementing formal processes to assist struggling residents. Another innovation is the competence committee, which rules on the promotion of residents, taking decision-making out of the hands of individual supervisors.
We must introduce a note of caution, however, even as we discuss the new model. There is great apprehension about such a massive shift in medical education. In response, the RCPSC and universities have embarked on an extensive educational strategy for supervisors and educators. In the medical education literature, there is a debate about “anatomizing” competence skills versus the global ability to integrate various competencies into a coherent conceptualization of practice.31 Perhaps this is analogous to the teachings of Socrates, the inventor of a model that we have followed for centuries. He emphasized that it is not the sequence of experiences in life but the integration of those experiences that is important, as, in the words of his famous aphorism, “the unexamined life is not worth living” (Ref. 32, p 31).
Some of the complex skills of psychiatry and forensic psychiatry cannot simply be learned. Instead, they are much more akin to the fundamental skills learned by musicians, who continue to improve their skills through practice, mentorship, and evaluation. As one skill improves, another area of skill might diminish; therefore, maintaining and improving becomes a lifelong process. It is, therefore, important to consider that residency training is not just a matter of checking items off a list that, when completed, qualifies the learner.
The Core Elements of Competence by Design
Stages of Training
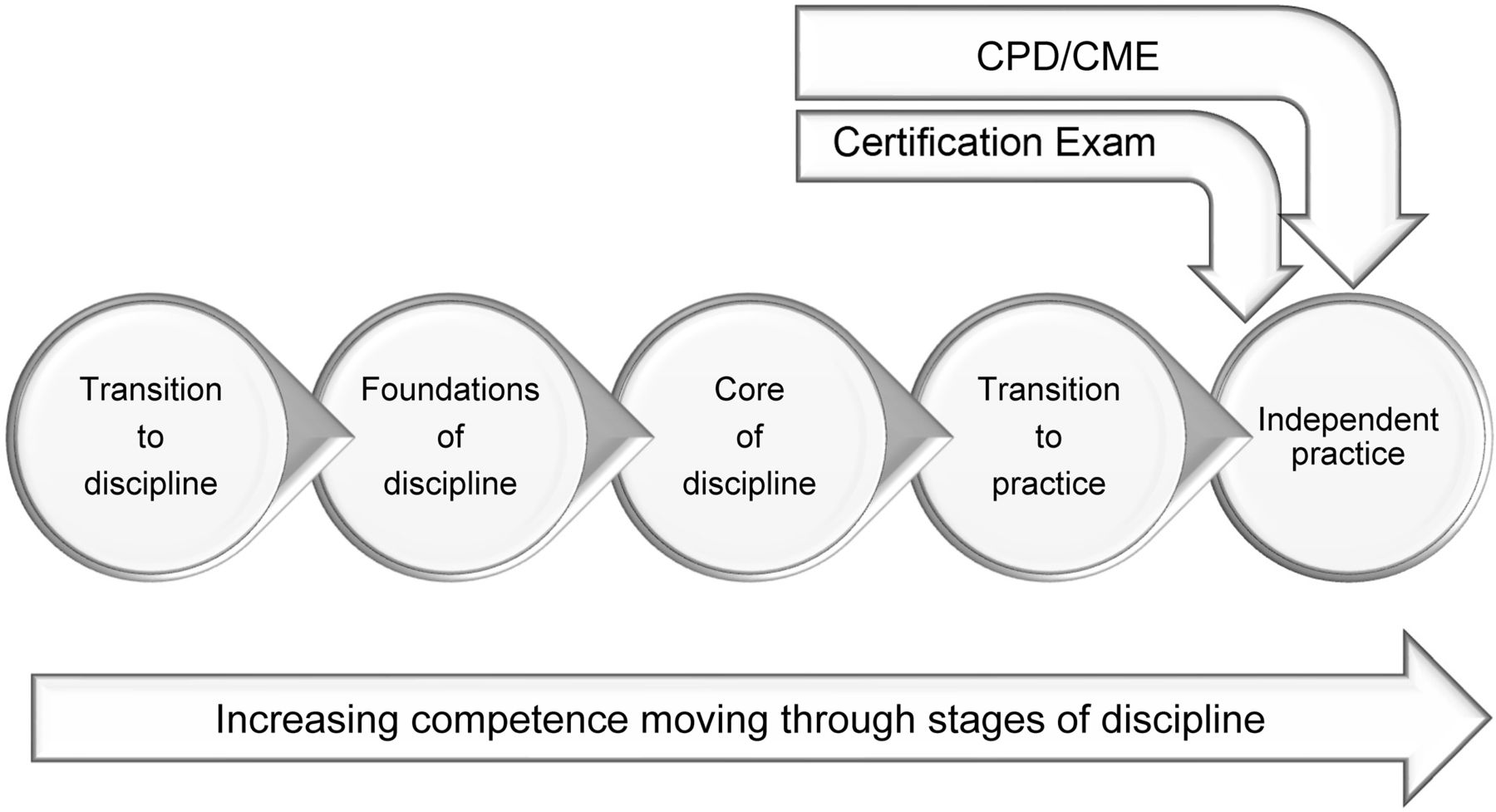
Medical education has been conceptualized in phases, with residency training occupying the central phase, as depicted in Fig. 2. In CBD, all specialties, including forensic psychiatry, begin the medical residency with an initial phase, Transition to Discipline, in which skills learned in medical school or a previous residency are confirmed among students arriving from different programs prior to entering discipline-specific training. The essential skills are observed directly and documented by the supervisor. The next phase, Foundations of Discipline, addresses broad-based competencies that one must acquire before learning highly specific skill sets within a discipline. For example, before general psychiatry residents can learn how to assess and manage a complex forensic psychiatry patient, they must be able to assess and manage an adult patient with a common psychiatric presentation. Learners next enter the Core of Discipline phase, where competencies typically attributed to a senior resident are acquired. In the last phase of residency training, Transition to Practice, a learner prepares for independent practice.
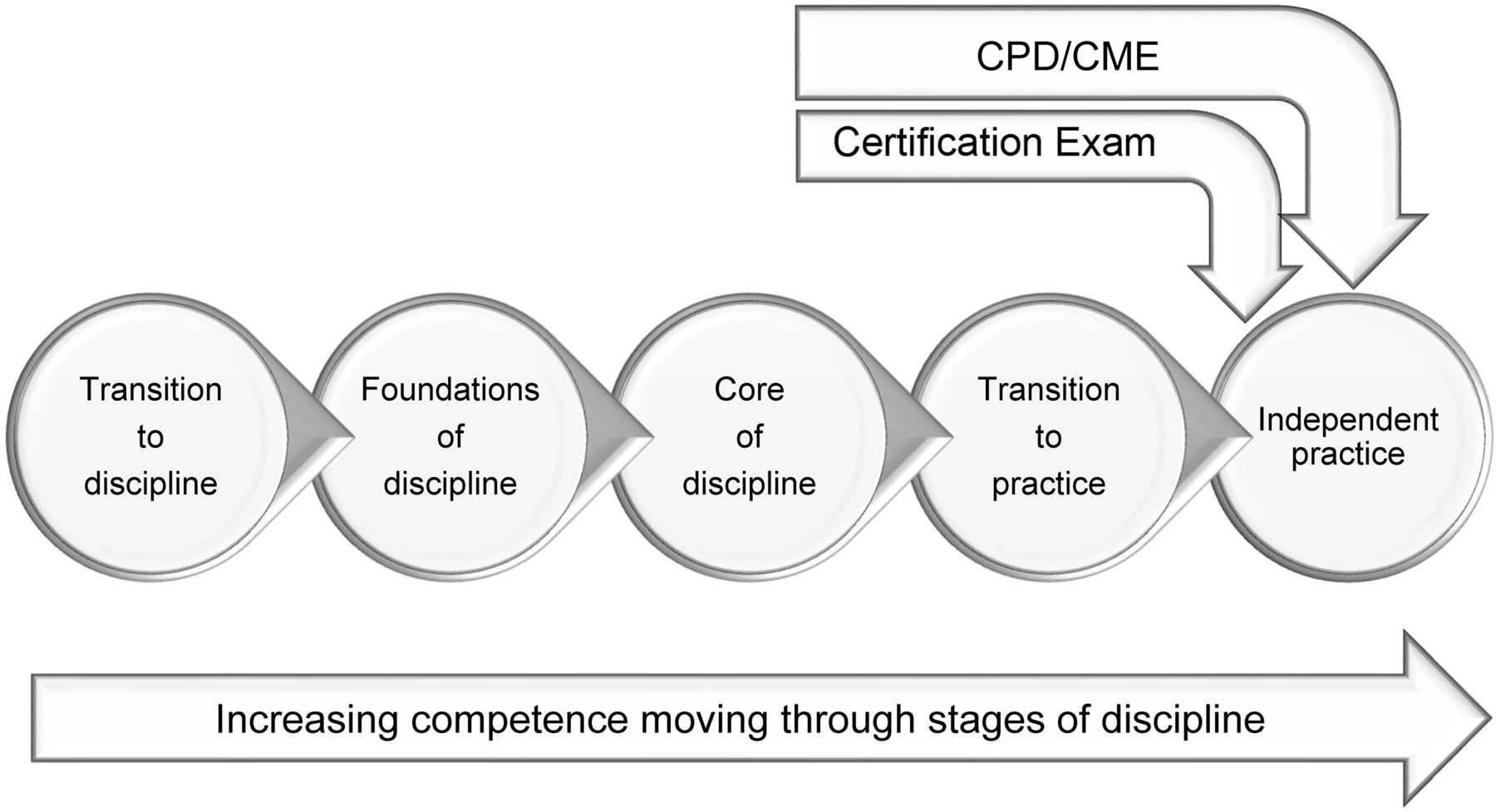
Stages of the Competence by Design model from general psychiatry transitioning to the discipline of forensic psychiatry to independent practice. CPD = continuing professional development; CME = continuing medical education. Adapted from The Royal College of Physicians and Surgeons of Canada.33
Entrustable Professional Activities
A primary goal of CBD is to ensure not only that residents are exposed to different areas of practice but also that they can demonstrate the skills required of their specialty. To achieve this goal, the CBD curriculum requires that each specialty devise entrustable professional activities (EPAs) for each stage of training. An EPA is an observable task of the discipline. Each EPA comprises multiple detailed milestones, which break a complex or multi-step task into its component parts. There are currently 16 EPAs that must be accomplished during the PGY-6 year in forensic psychiatry in Canada. The content for each EPA and milestone was derived by consensus based on the expertise of the working group, existing specialty training requirements, and elements of training requirements that the Royal College has been mandated to superimpose to meet societal expectations.
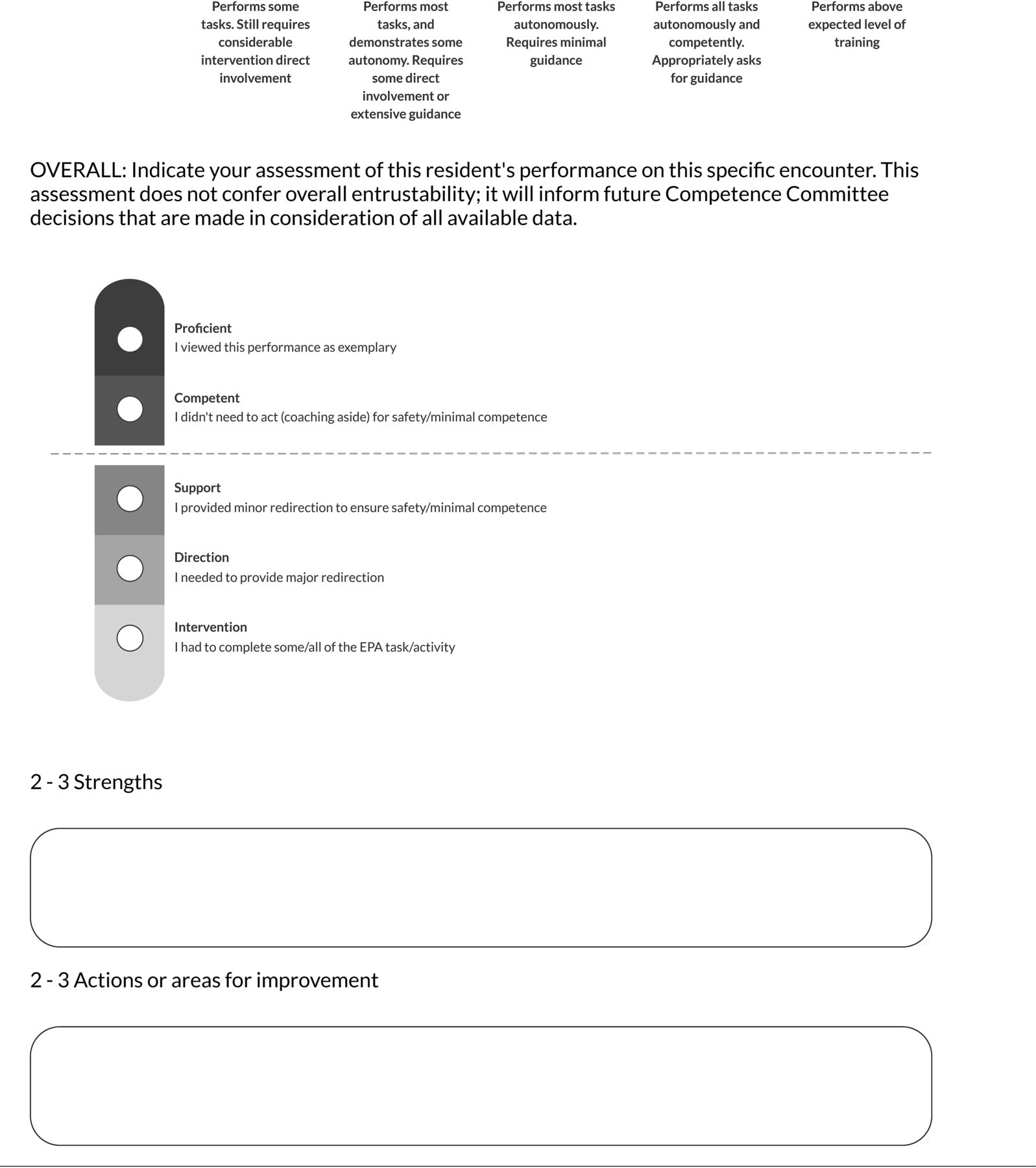
The assessment of EPAs is designed to facilitate the learning and feedback that occurs between supervisors and trainees by highlighting specific areas of strength and areas of continuing development. These EPAs can be utilized to coach a trainee and modify learning plans as needed. Assessment of EPAs also results in multiple data points that are then reviewed by a competence committee, along with other assessment tools, in an aggregate fashion to make decisions about progression and promotion.
Required Training Experiences
To develop the CBD model, each specialty committee of the RCPSC reviewed its discipline-specific competencies and determined which training experiences would be required and which would be recommended or optional. This process incorporated expert opinions from across the country, past training requirements, and clinical training resources within programs nationally. In the new CBD model, each program is required to map out each required training experience and EPA in its curriculum.
Competence Committee
As noted earlier, the traditional model of medical education lacks a formal process by which faculty could discuss the strengths and challenges of a resident based on multiple points of assessment data and form learning plans tailored to those needs. This deficit has led to one of the essential components of CBD: the competence committee.34 The task of this committee is to move toward more valid and fairer evaluations of residents based on the evidence. Specifically, the committee makes decisions and recommendations by integrating multiple data points, such as achievement of EPAs, In-Training Assessment Reports (ITARS), 360° evaluations, formative feedback from supervisors, and personal reflection tasks. The committee uses a decision-making process whereby patterns of performance can be analyzed to reveal a broad picture of a resident's progress to support learning, development, and greater clinical independence over time. This group decision-making process requires the competence committee to meet at regular intervals throughout training.
The review of a variety of assessment tools not only provides a breadth of information on resident performance, beyond what can be determined by any single supervisor, but also allows for identification of specific gaps or areas of acceleration, which can inform future learning plans. The committee provides recommendations regarding progress and promotion to the next stage of learning and offers suggestions of remedial experiences that can strengthen specific learning needs, such as modified rotations and mentorship or coaching. In addition, the competence committee serves as the decision-making body. It allows for the preservation of the clinical faculty teaching role as one of primarily coaching, and the provision of frequent feedback through documented low-stakes but regular observations, thereby promoting a more positive learning climate while maintaining a process for objective and valid evaluation.
The size and composition of a competence committee vary between programs, and there is no single way to set up this committee. Some committees will opt to have the program director present and chair each meeting, while other programs may choose to not have the program director involved. The presence of a resident representative on the competence committee also varies. The frequency of meetings should be sufficient to ensure that promotion through stages of CBD is monitored in a timely fashion. For the one-year forensic psychiatry subspecialty program, this necessitates a minimum of three meetings per year for each resident.
Finally, the implementation of CBD is a large undertaking, and its success will depend largely on effective faculty and resident development plans. Many university programs have CBD lead roles to assist in this process, which requires close collaboration with the RCPSC and local postgraduate medical education offices. Faculty development should occur early and frequently in many domains. It should cover the overarching theory and terminology of CBD, the basics of EPAs and milestones, the role of the competence committee, and training on new technology.
Several educational resources are available centrally, though it is the responsibility of each program to develop a tailored plan of dissemination. Faculty and resident education can take many forms, including educational retreats, webinars, weekly frequently asked questions e-mails, and individual training sessions. Further, programs should commit to a process of iterative feedback and improvement, especially in the initial stages of implementation. It is reasonable to anticipate some resistance, as the expectations of faculty are higher in this new curriculum, with greater direct observation of learners, more frequent in-person feedback, and routine use of technology to complete assessments. At the time of writing, we have not encountered resistance, and faculty appear receptive to the new developments.
Description of Competence by Design
Stages of Training
In forensic psychiatry training, the Transition to Discipline stage will serve to orient the resident to the subspecialty. Training programs will need to verify that PGY-6 residents have the necessary general psychiatry skills to perform forensic psychiatry, and this introductory period will provide a baseline assessment of the learner's previous exposure, skill, and knowledge of the discipline so that their forensic psychiatry training can be individualized. Reviewing previous specific experiential learning, didactic, or shadowing opportunities can assist programs at this stage.9
The Transition to Discipline stage will also serve to orient residents to the CBD principles they will use. In this stage, residents will be introduced to the institutional and program settings where they will train, the teams with whom they will work, and the personal safety policies they will need to follow. Learning about the complexities of the dual role of the clinician and legal expert in forensic psychiatry and the forensic method will be an early required element of this stage of forensic psychiatry training. The required training experiences will involve working on inpatient or outpatient forensic psychiatry services. It is anticipated that, on average, residents will require about two weeks to complete this stage of training.
Residents will then graduate to the Foundations of Discipline stage of training, where they will focus on developing a forensic approach to conducting psychiatric assessments and acquiring a solid knowledge of jurisprudence relevant to Canadian forensic psychiatry. Residents will spend an average of three months at this stage of training. The primary focus will be on criminal assessments in a forensic inpatient service and clinic, remand center, and court. Residents will be required to prepare reports and prepare for expert testimony.
The goals for this stage are for residents to demonstrate competence in completing uncomplicated assessments of adult cases involving fitness (competency) to stand trial, criminal responsibility, and violence risk assessment, as well as assessment, management, and testimony at review boards regarding individuals who have been found not criminally responsible. The required training experiences will continue to be inpatient, outpatient, or remand settings. Residents will be expected to observe and provide testimony before a court and a review board in uncomplicated cases. They will generally participate in a mock trial, which will supplement or replace actual testimony. They will receive formal instruction in data gathering, interviewing, and report writing for fitness to stand trial and criminal responsibility cases. Other formal teaching will include ethics guidelines, basic elements of legal procedure, structure of the legal system, principles of risk assessment tools, and review of landmark cases.
The Core of Discipline stage, which will generally encompass about eight months of training, will focus on the full breadth of forensic psychiatry practice, including diverse case complexity in all forensic settings in both criminal and civil cases. Residents will build on earlier skills and be able to complete legally defensible assessments and reports and testify in increasingly complex cases. They will become competent in the consultation, treatment, and rehabilitation of inpatients; develop their role as leaders of their forensic psychiatry teams; and act as resources for legal, justice, and correctional professionals. Required training experiences will involve both inpatient and outpatient settings, where residents will be exposed to cases of fitness, restoration to fitness, not criminally responsible, risk assessment using actuarial and structured professional judgment tools, dangerous offender and long-term offender assessments (the Canadian equivalent of sexually violent predator legislation), sexual behaviors, civil forensic matters, and correctional psychiatry. Formal training is also expected in landmark cases, the specific subject areas pertinent to this stage of training, and career planning.
The final Transition to Practice stage will likely take anywhere from two to four weeks and will focus on residents' consolidating their abilities to triage referrals and manage a typical workload of cases. They will prepare for nonclinical aspects of practice, including billing, office management, development of their professional curriculum vitae, and plans for lifelong learning and professional development. They will be required to receive formal training and mentorship in billing, practice and office organization, development of a private practice, managing complaints, and licensing. The breadth of experiences they have attained up to this point in training will be reviewed to identify potential gaps and to plan further professional development based on career prospects and interests.
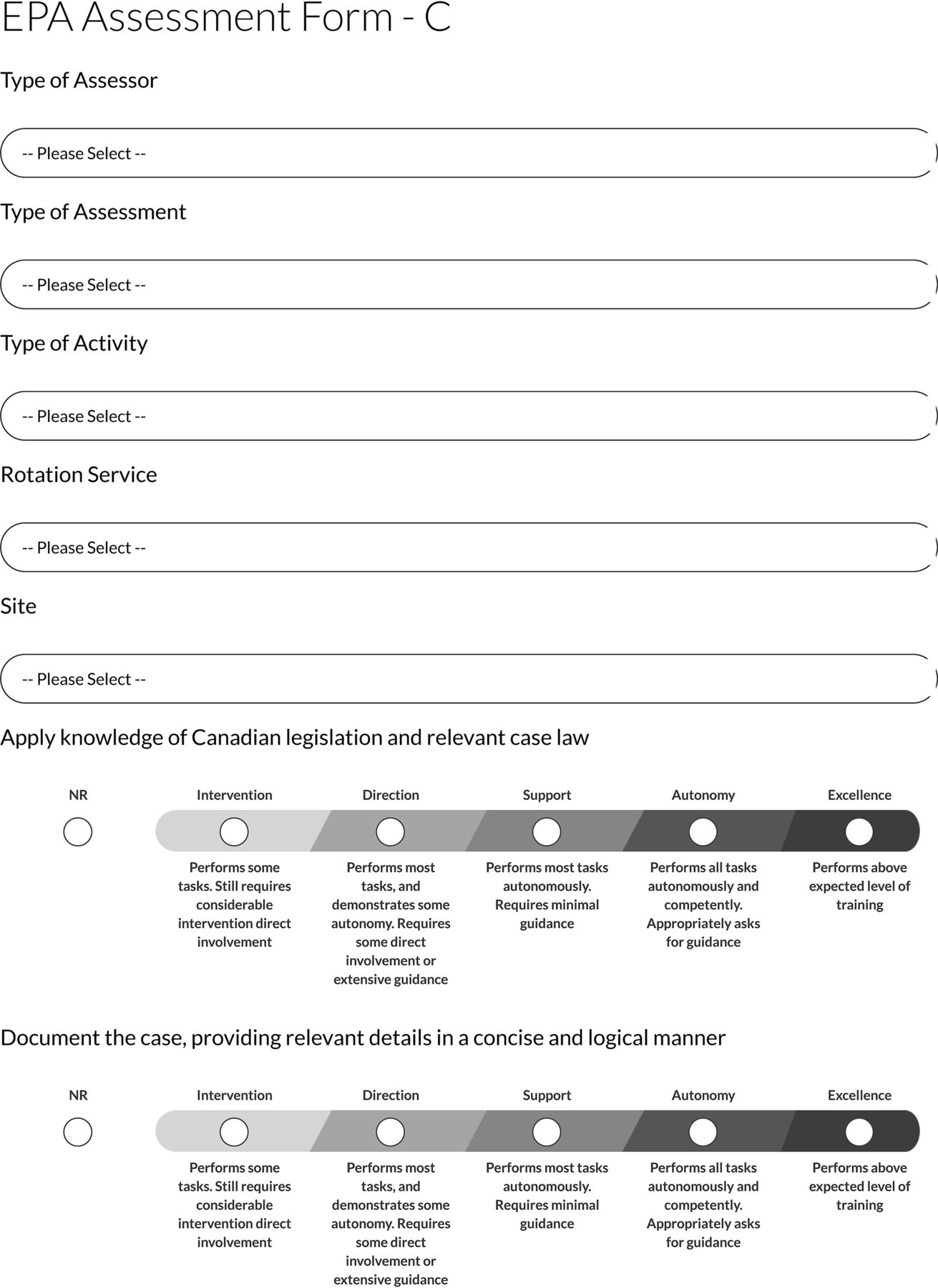
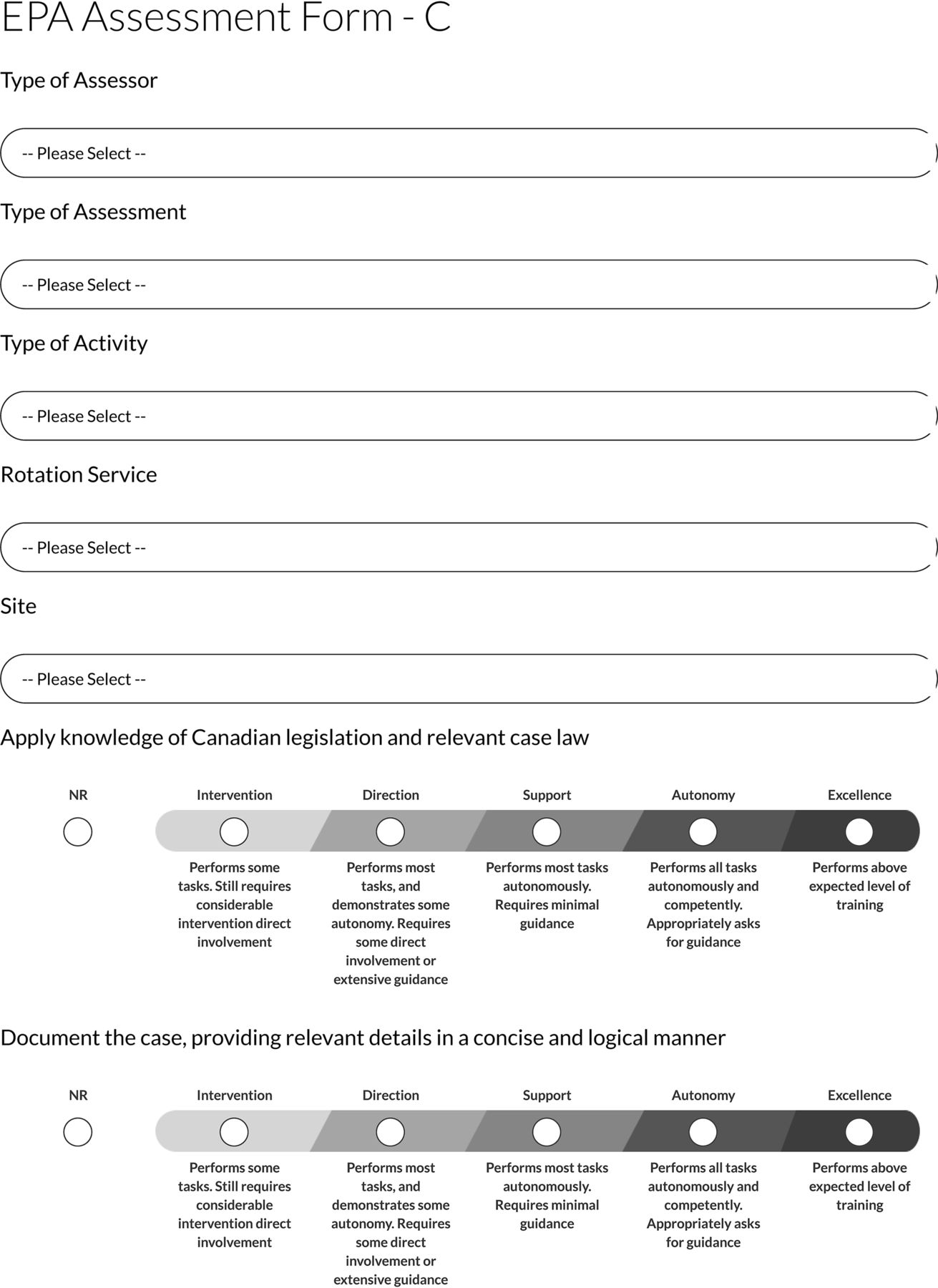
In keeping with the CBD philosophy of frequent assessment and monitoring of competency, residents will be expected to take on a proactive role in their learning by prompting their supervisors to assess them regularly using online platforms. A resident will seek out as many direct observations as needed to reach the required number of “achievements” for any given EPA in the context specified. To facilitate ease of documentation, online platforms, such as Elentra,35 have been developed and will be available on tablets and smartphones. An illustration of an EPA that has been uploaded using this system is provided in the Appendix. Some universities may elect to assign academic coaches to residents, separate from their primary supervisors, to help them identify when they should be referred to the competency committee for a decision as to whether they are ready to progress to the next stage of training.
EPAs in Forensic Psychiatry
Forensic psychiatry lends itself easily to being broken down into specific tasks. Multiple EPAs have been developed for each of the stages of the PGY-6 year in forensic psychiatry, and, within each EPA, multiple detailed milestones are referenced as a guide to assessing the competencies sought. Residents will be expected to perform a certain number of tasks to move on to the next stage. In this article, we present an overview of the program to illustrate the different tasks in which a resident will be expected to show competency. A description of the specific knowledge and skills included in the milestones of each EPA goes beyond the scope of this article. Table 1 summarizes the EPAs associated with each training stage.
Entrusted Professional Acts for Canadian Forensic Psychiatry
In the Transition to Discipline stage, residents will be expected to achieve EPAs focused on providing risk assessments and management plans in general psychiatry evaluations, discussing and documenting consent in forensic assessments, documenting clinical encounters, and working effectively in a team setting. In the Foundations of Discipline stage, EPAs will include conducting uncomplicated assessments of fitness to stand trial and criminal responsibility and providing treatment and management of risk for individuals under the jurisdiction of the Criminal Code Review Board.
During the Core Stage, EPAs will be more detailed, separating the tasks of conducting forensic psychiatry evaluations, writing reports, and providing expert testimony. In addition, they will include tasks across the breadth of forensic psychiatry, including sexual behaviors, correctional psychiatry, child and adolescent forensic psychiatry, and civil forensic psychiatry. There will be an assessment of residents' management of patients with complex presentations, as well as working with interdisciplinary teams. Residents will need to show competency in using risk assessment tools for violence and sexual risk assessments.
During the Transition to Practice stage, EPAs will focus on showing a resident can manage the caseload of a forensic psychiatrist, maintain a professional curriculum vitae, and develop a continuing professional development plan for the first three to five years of practice.
International Comparison
A comprehensive comparison of training in different countries is outside the scope of this article. With the goal of contextualizing the Canadian experience, we will briefly mention some other interesting initiatives in this area. In the United States, there has been movement toward establishing milestones in forensic psychiatry relevant to fellowship training.1 These are designed for use in semiannual reviews of fellowship program performance. The information reported is used as one element in the accreditation system. The introduction to their document notes that, up to the present time, it is not known whether the data are of sufficient quality to be used in high-stakes decisions.
Each milestone has a scoring system that can be scored on five levels. Several specific forensic competencies are detailed. These milestones roughly translate into what the Canadian system terms competencies, which are then broken down into EPAs. In the Canadian system, these EPAs are further broken down into milestones that are assessed by the clinical supervisor and entered into an electronic system. Despite the differences in nomenclature, the goals of the U.S. system are similar to those of the Canadian system. Although these competencies were devised some years ago, their utility has been confined to accreditation purposes. There are as yet no mechanisms for supervisor training or any type of uniform evaluation, which has delayed national implementation.
A similar system was designed in the United Kingdom in 201437; it has been updated twice more since then. To satisfy the requirements of specialist training in forensic psychiatry, a trainee must follow an eight-year pathway. The first five years include two years in the foundation training program, followed by two years in the core psychiatric training program. This scheme is familiar to a North American readership as it is approximately equivalent to the five years of general psychiatric training with which we are familiar. This period would include training in emergency psychiatry, general psychiatry, and subspecialties. It may or may not include a six-month rotation in forensic psychiatry.
There is an extensive list of learning outcomes. The learner is expected to gradually progress to mastering all of these by the end of three years. They range from the basic skills of history taking in the initial stages to designing, writing, publishing, and presenting a research project. Governance (i.e., administration) and leadership skills are also expected.
The trainee is reviewed annually by a constituted committee. At the end of two years of foundation training, the trainee must undergo a national selection process before being appointed to a post that entails core psychiatry training. At the end of core psychiatry training, again with annual reviews and a final review, there is a three-part examination to become a specialist in psychiatry. The trainee then applies for selection by open national competition for advanced training in forensic psychiatry, which entails a full three years.
Also notable are the various roles of the educators and supervisors. These roles are clearly defined in the curriculum and include training program director, clinical supervisor, educational supervisor or tutor, medical psychotherapy tutor (who is generally a psychotherapist), psychiatric supervisor, as well as a number of assessors who can be multidisciplinary. The supervisors are mandated to attend a two-day training program, which must be refreshed every two years.
The types and number of assessments for each specific learning outcome are clearly tabulated. It is assumed that one of the purposes of the extensive training for supervisors is to learn the meaning of the dizzying array of acronyms tabulated in the types of assessment for each learning outcome (our personal favorites being DONCS and DOPS). This program uses workplace-based assessments (WPBA) and lists 10 types of tools as well as the number of each of these assessments required per year (see Ref. 37, pp 56–57). The reader is referred to the original document for a full explanation of these.
The model used in Australia and New Zealand is based on a two-year certification program, which follows the completion of the general psychiatric training.38 The requirements for training are clearly defined and must be completed in accredited programs. They use the same language as the Canadian system noted above in defining broad competence, which is broken down into a specific number of EPAs. The model also describes mandatory training experiences, including three months treating prisoners, three months in an inpatient unit, three months in rehabilitation, and three months in the community, over the course of the 24-month program. The requirements also include successful completion of a research project, which must include publication in a peer-reviewed journal or a master's or honors thesis in a relevant field. Supervisors are provided with mandatory training.
Conclusions
The type of training involved in the fellowship year of the forensic psychiatry subspecialty is transitioning to a new model: Competence by Design. This model addresses many of the criticisms of previous time-based training. It includes four phases of training: Transition to Discipline, Foundations of Discipline, Core of Discipline, and Transition to Practice. Each stage is characterized by specific EPAs that are regularly assessed by a supervisor in a manner that is both specific and corrective. Assessment is regular and repeated, and feedback is given in a manner that facilitates change. Electronic recordings of EPAs are presented, not to an individual supervisor, but to a competency committee that reviews each resident's progress in detail and decides either to move the resident to the next phase or to design a plan for remediation.
It is anticipated that the documents defining the competencies and EPAs will be reviewed annually by the Subspecialty Committee. The authors of this article are all members of the Subspecialty Committee, which is under the auspices of the College, and we anticipate that, after the first two years of the program, we will meet again for a complete and thorough review. We hope that, after some experience with the model, we can collectively develop and improve the requisite areas. By the simple process of having to document the plan for this article and receiving helpful feedback from the reviewers, we can already see some areas upon which we might improve. We are considering methods to collect data to delineate whether the trainees benefit from the program and whether they graduate from the program with improved skills as a result of the changes. The final common goal of increasing the competence of the body of forensic psychiatrists will be difficult to enumerate, but doing so remains an aspirational target.
Only time and feedback will tell how the execution of the CBD model will improve the learning and assessment of residents and postgraduate education. It is unclear if it will merely lead to a sense of confusion, with resulting frustration. It is possible that, despite the best efforts of the College and its proxy, the Subspecialty Committee, programs will continue in approximately the same manner as before, and it will be business as usual. It is hoped that the use of this model will lead to sensible innovation and an improvement in teaching and learning, which will result in the increased competency of residents as they transition into independent practice.
Acknowledgments
The authors thank the members of the Forensic Psychiatry Competency by Design working group for their expertise: Yuri Alatishe (McMaster University), Azaad Baziany (University of Saskatchewan), Brad Booth (University of Ottawa), Jocelyne Brault (Université de Montréal), Aileen Brunet (Dalhousie University), Sumeeta Chatterjee (University of Toronto), Fabien Gagnon (Université Laval), Graham Glancy (University of Toronto), Michelle Mathias (University of Ottawa), Gabrielle Provost (Université de Montréal), Lisa Ramshaw (University of Toronto), Victoria Roth (University of British Columbia), Kimberly St. John (Memorial University), Scott Theriault (Dalhousie University), Todd Tomita (University of British Columbia), Jeffrey Waldman (University of Manitoba), Joel Watts (University of Ottawa), Lenka Zedkova (University of Alberta), Jolanta Karpinski (RCPSC/University of Ottawa), and Virginia Frans (RCPSC).
APPENDIX
Example of an Entrusted Professional Acts (EPA) assessment form in Elentra.35

Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2021 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}