


Abstract
Unlawful behaviors have been reported in association with Huntington's disease (HD), although their overall prevalence and clinical significance remain unknown. Recognition of problematic behavior is limited by stigma and lack of routine clinical assessment, as well as the absence of validated screening measures. We performed a retrospective chart review of 289 patients treated for HD at Vanderbilt University Medical Center from 2006 to 2020 to assess the frequency of illegal activity in our HD population. We identified 31 patients with HD who have a documented history of unlawful behavior, comprising 11 percent of the charts reviewed. Physical violence was the most common behavior reported, followed by reckless driving, substance abuse, illegal financial activity, and inappropriate sexual behavior. Mean age at the time of the first offense was 37 years. Patients with criminal offenses were more likely to be male and in the early stages of disease with associated psychiatric symptoms. Our results emphasize that illegal activities are a significant clinical problem in individuals with HD, particularly young adult males with comorbid psychiatric symptoms. These findings highlight the need for improved screening measures to detect high-risk behaviors in individuals with HD, as well as evidence-based protocols to guide triage and management of patients engaging in potentially detrimental activities.
Huntington disease (HD) is an autosomal dominant neurodegenerative disease caused by an inherited cytosine-adenine-guanine (CAG) trinucleotide expansion in the huntingtin (HTT) gene. Most often, HD manifests mid-life, between 30 and 40 years of age, and it traditionally is diagnosed upon the appearance of abnormal movements such as chorea.1,2 Cognitive and behavioral symptoms can emerge 10 to 15 years before the onset of motor symptoms3 and are often the most disabling aspect of this disease.4 A wide range of behavioral changes have been described in HD, including irritability,5 impulsivity,6 frontal dysfunction,7 and risk-taking behaviors.8,9 Criminal behavior has also been reported in HD, including some particularly prominent cases that have garnered media attention in recent years.10,11 Despite popular interest in this phenomenon and the potentially detrimental personal and societal impacts of these behaviors, there is relatively little literature regarding the prevalence, predictors, and clinical relevance of illegal activities in HD.
Much of our current understanding of criminality in HD relies on retrospective reviews of police records and criminal conviction databases conducted in the 1950s through the 1970s in various locations around the world.12,–,14 These studies have indicated variable rates of illegal behavior ranging from 5 percent to 18 percent in the specific HD populations studied. A more recent review from Denmark that compared registered criminal convictions in people with HD, nonaffected first-degree relatives, and community controls reported an increased rate of crimes in male patients with HD (27.3%) compared with both nonaffected relatives (9.7%) and non-HD controls (12.7%).15 Rates of unlawful behavior in female patients were much lower (4.6%) and were not significantly different from nonaffected relatives or controls. Most of the crimes reported were of relatively low severity (i.e., traffic offenses, drunken driving, assault, theft, vandalism, fraud), and no cases of more serious offenses such as murder, rape, or arson were identified.
Another recent retrospective review examined criminal behavior in a heterogeneous population of 2,397 patients with dementia, including 30 patients with HD.16 Overall, 8.5 percent of the patients reviewed had a documented history of criminal behavior in their medical record, ranging from 7.7 percent of patients with Alzheimer's disease to 37.4 percent of patients with behavioral variant frontotemporal dementia. Six of the 30 patients with HD (20%) had a history of criminal activity, which was noted to be the presenting symptom in five of these patients.
To date there have been no systematic investigations of criminal behavior in a large clinical population of patients with HD, and there is currently limited evidence regarding the clinical correlations and impact of these behaviors. We present the results of a retrospective chart review performed at a large HD Center of Excellence to assess the frequency and clinical significance of illegal activity in our HD population.
Methods
We reviewed the charts of 289 patients treated for HD at Vanderbilt University Medical Center from 2006 to 2020. Patients were identified on the basis of International Classification of Diseases, Ninth Revision (ICD-9) code 333.4 or ICD-10 code G10. All persons with a confirmed clinical or genetic diagnosis of HD based on currently accepted diagnostic criteria were included.17 Persons for whom a diagnosis of HD could not be confirmed were excluded. A clinical diagnosis was defined as the presence of unequivocal motor signs consistent with HD on an exam performed by a neurologist. A genetic diagnosis was defined as CAG repeat length ≥ 36. CAG repeat length refers to the number of CAG trinucleotide sequences contained within the huntingtin (HTT) gene on chromosome 4. The wild-type gene contains CAG repeat lengths between 6 and 26. CAG repeat lengths between 27 and 35 are considered intermediate alleles, which typically do not cause clinical symptoms in the carrier but are unstable and may expand during reproduction and thus affect future generations. CAG repeat lengths between 36 and 39 can be associated with incomplete penetrance and symptom onset at a later age but are considered to be the diagnostic threshold of HD.17,18 CAG repeat lengths of 40 and above will cause clinical manifestations of HD within a normal lifespan with complete penetrance. In general, a higher number of CAG repeats is associated with an earlier age of onset and greater disease severity.18,19
Patient charts were subsequently screened for documentation of criminal behavior, including illegal or criminal activities, police interaction, arrests, or incarceration. A list of search terms was generated on the basis of criminal activities documented in previous publications15,16 as well as input from HD clinicians. These keywords included arrest, court, police, driving under the influence (DUI), jail, prison, violence, theft, speeding, criminal, legal, sexual, ticket, abuse, and substance. Charts identified through this search were then reviewed in detail, and patients were classified as offenders or nonoffenders on the basis of the presence or absence of illegal activities. Criminal behaviors were subdivided by category, and any consequences of these behaviors were also noted. Clinical and demographic information were recorded for all patients with and without criminal behavior, including age, gender, and CAG repeat length. CAG-Age Product (CAP) scores (i.e., age × CAG repeat length of mutant allele – 33.66) were calculated for each patient at the time of the legal event noted to provide an estimation of disease stage.20,21 The CAP score serves as a marker of disease burden and has been used as an estimate to predict time to motor symptom onset, which generally occurs at a CAP score > 400.3 Comorbid psychiatric symptoms were obtained from clinical notes and Problem Behaviors Assessment-short form22 scores when available. This study was exempted from review by the Vanderbilt Institutional Review Board. A waiver of consent was granted as this was a retrospective review of existing data that was deemed to pose minimal risk to participants.
Statistical Analysis
Statistical analyses were performed with SPSS 26 (IBM Corp., Armonk, NY). Patients were grouped according to presence or absence of documented criminal behavior. Clinical variables were reported for each group as mean ± SD. The Student t test was used to compare means between groups for continuous variables (e.g., age, CAG repeat length). The chi-square statistic was calculated for categorical variables (e.g., gender, prevalence of psychiatric symptoms).
Results
Of 289 patient charts initially screened, 282 had a confirmed clinical or genetic diagnosis of HD. Thirty-one of these patients (11%) had a documented history of criminal behavior in their medical record; 251 patients (89%) had no documented criminal behavior. A flow chart is shown in Fig. 1. Demographic data for patients with and without unlawful behavior are shown in Table 1. Sixty-five percent of patients with a history of criminal offenses were male, versus 43 percent of nonoffenders [chi-square (1, n = 282) = 5.34, P = .02]. Mean CAG repeat length was 48 ± 4.8 for patients with criminal offenses and 44 ± 4.3 for patients without offenses [t(190) = 4.34, P < .0001]. While the majority of patients without criminal offenses had CAG repeat lengths between 40 and 44, a significantly higher proportion of patients with criminal offenses had a CAG repeat length between 45 and 49 than patients without criminal offenses [42% versus 25%; chi-square (1, n = 192) = 3.53, P = .060]. The same was true for repeat lengths > 50 [31% versus 12%; chi-square (1, n = 192) = 6.33, P = .012].
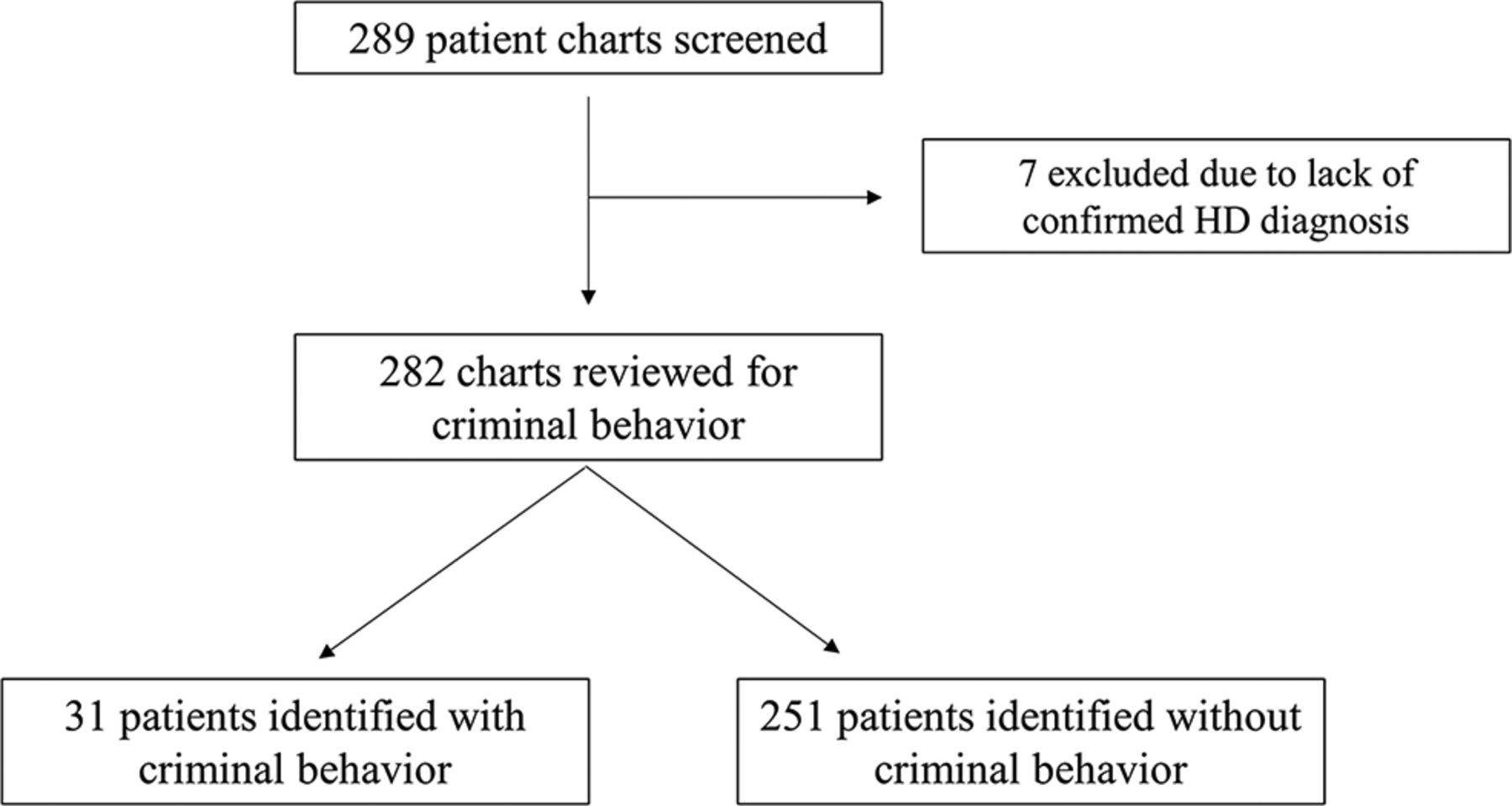
Flow chart depicting chart review process. HD = Huntington's disease.
Demographics
For individuals with a history of criminal behavior, mean age at the time of the first offense was 37 ± 13 years, ranging from 17 to 72. CAP scores at the time of first offense ranged from 200.1 to 661.5, with a mean of 464.7 ± 122.7. Twenty-seven percent of patients had a CAP score of < 400 at the time of first offense, whereas 73 percent had a CAP score > 400. The majority of the patients were in the early manifest stage at the time the first illegal activity was documented. Age and CAP score at time of first offense did not differ significantly by gender. Males first engaged in illegal activities at a mean age of 34.5 ± 12 years, whereas females averaged 41.6 ± 14 years of age [t(29) = 1.505, P = .14]. Mean CAP score at time of first offense was 459.2 ± 126.3 for males and 475.1 ± 122.4 for females [t(24) = 0.308, P = .76].
Comorbid psychiatric symptoms were reported in 100 percent of patients with a history of criminal behavior and in 80 percent of patients without a criminal history [chi-square (1, n = 282) = 7.51, P = .006]. Rates of depression, irritability, aggression, apathy, perseveration, and delusions were significantly higher in offenders compared with nonoffenders. These data are shown in Table 2.
Percent of Patients Endorsing Each Psychiatric Symptom
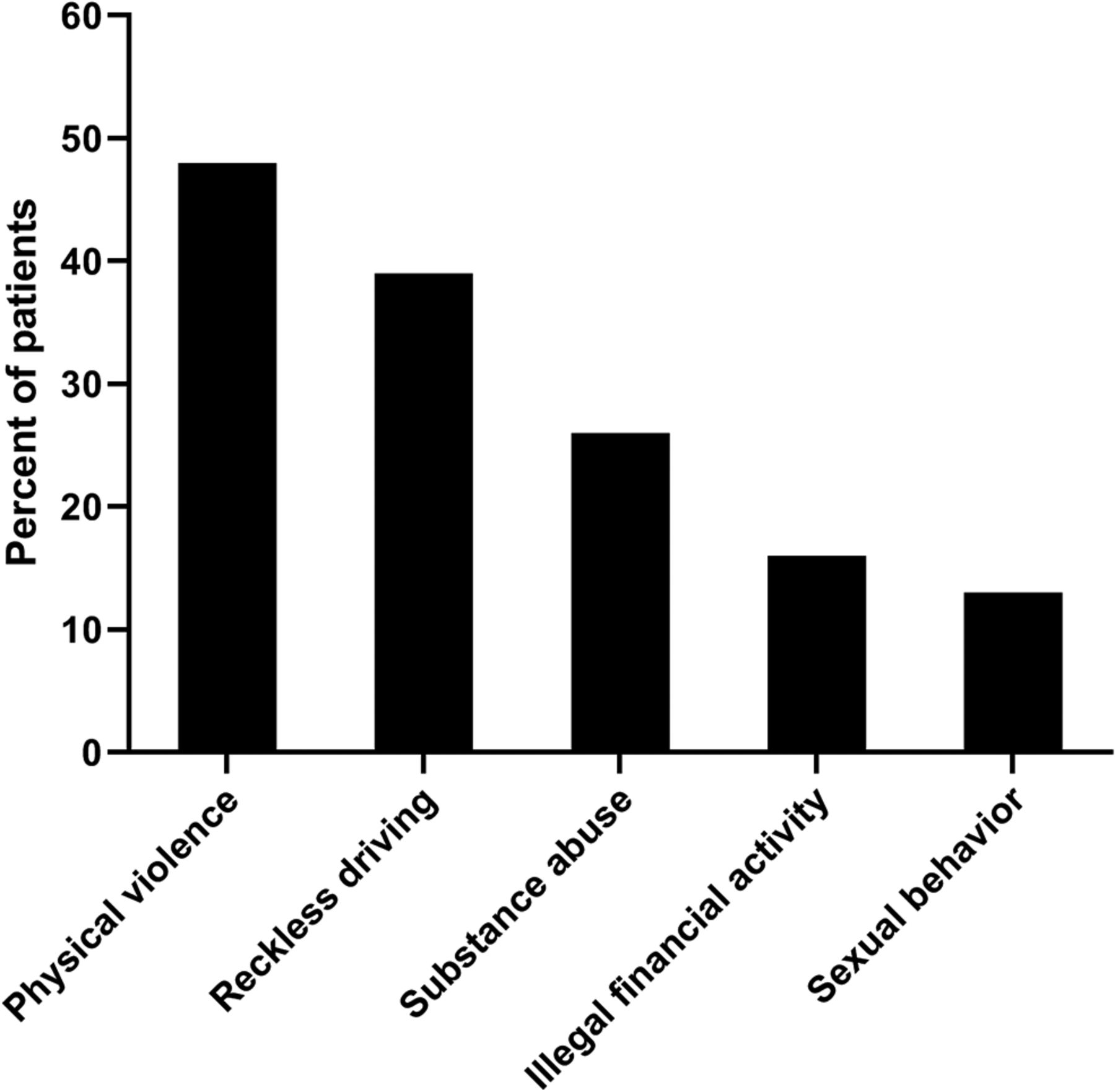
Types of illegal activities reported are shown in Fig. 2. The most prevalent behavior was physical violence, reported in 15 of 31 patients (48%). Examples of physical violence included assaulting a police officer, domestic violence toward spouses and other relatives, physical altercations with teachers or co-workers, and aggressive behavior toward clinicians. Reckless driving (i.e., speeding, driving erratically or recklessly, driving under the influence, or being involved in at-fault crashes) was the second most common behavior reported, affecting 39 percent of patients. Twenty-six percent of patients faced legal consequences due to substance abuse, including public intoxication, other alcohol-related charges, and use of illicit substances including methamphetamines and opiates. Inappropriate sexual behavior was noted in 13 percent of patients, including indecent exposure, pornography use in school, and exploitation of a minor. Sixteen percent of patients engaged in theft or other illegal financial activity, such as shoplifting, auto theft, and unpaid child support. Sixteen patients (52%) were repeat offenders, with two to five instances of criminal behavior reported.
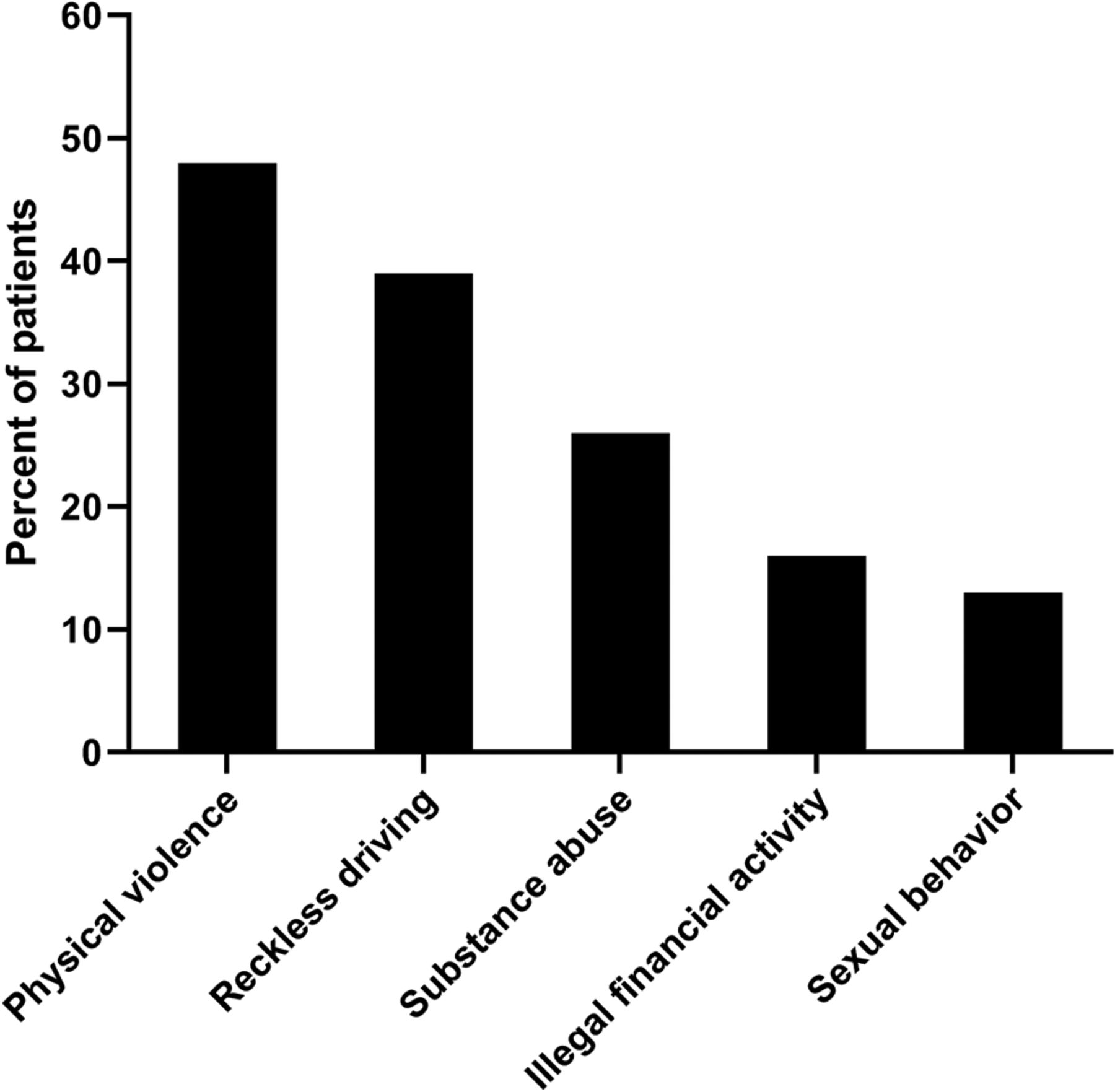
Frequency of criminal behaviors reported by category.
Consequences varied, with arrest being most common. Of the 31 patients, 18 (58%) had been arrested, with seven (23%) having been arrested more than once. Additional consequences included DUI citations (13%), probation (16%), court-ordered rehab (3%), termination from job (3%), driver's licenses revoked or suspended (10%), other citations (13%), speeding tickets (10%), and registration as a sex offender (3%).
Discussion
To our knowledge, this clinical cohort is the largest HD population in which criminal behavior has been studied to date. Eleven percent of the 282 patients included in this study had a documented history of unlawful behavior, in line with previous studies indicating a prevalence of criminal activity between 5 percent and 20 percent in HD.12,–,16 Physical violence was more commonly encountered, followed by reckless driving and substance abuse. These behaviors resulted in significant consequences, including arrests, license revocation, job loss, and registration as a sex offender. Our results indicate that criminal behavior is a significant but understudied clinical problem in HD that can have substantial impacts on patients and families.
Our findings also suggest that certain clinical and demographic factors may influence a patient's risk of engaging in illegal activity. Sixty-five percent of the patients in our cohort with a history of criminal behavior were male, which aligns with previous literature15 and crime statistics in the general population.23 We noted a higher rate of illegal behaviors in our female cohort than has been reported previously (7.1% versus 4.6%).15 Comparison with a community control group in future studies may further elucidate these gender differences. Patients with criminal offenses also tended to have a higher CAG repeat length than those without criminal offenses, suggesting a potential association with earlier disease onset and increased severity. The majority of the patients had a CAP score > 400 at the time of the first documented criminal offense and were most commonly in the early manifest stage of disease when these behaviors were reported. We must note, however, that earlier offenses during the premanifest period may have been missed in this retrospective analysis, as HD patients often do not receive consistent medical care until they develop motor symptoms.
All of the patients who had committed criminal offenses had comorbid psychiatric symptoms, with significantly higher rates of depression, irritability, aggression, apathy, perseveration, and delusions compared with nonoffenders. Psychiatric symptoms have been associated with criminal offenses in other conditions, including bipolar disorder,24 schizophrenia,25 and posttraumatic stress disorder.26 Anger and irritability have been shown to be particularly strong predictors of violent and antisocial behavior, especially in those who have been exposed to trauma.26,27 The high prevalence of irritability and aggression in HD in combination with significant psychosocial stressors28,29 may create a unique vulnerability to the development of criminal behavior in this population. The fact that nearly a quarter of our patients with criminal offenses reported delusions was somewhat surprising. Delusions are relatively rare in HD,30 although they have been associated with violent behavior in patients with psychosis.31 This relationship appears to be mediated by anger resulting from delusions rather than the delusions themselves,32,33 which suggests that irritability may play a mediating role in this observation. The higher frequency of apathy in offenders compared with nonoffenders is also interesting. This association may seem counterintuitive initially, as apathy might sometimes be interpreted as inaction or indifference, but it may also translate to a lack of regard for the consequences of adverse behaviors. Depression is typically associated with a lower rate of criminality than other psychiatric disorders,34 but the combination of depression with other affective symptoms in HD may outweigh the effects of depression alone.
The cognitive and behavioral symptoms associated with HD may also lead to a heightened susceptibility to engaging in illegal activities. Behaviors related to the frontal lobe, including disinhibition, apathy, executive dysfunction, and loss of insight, are widely prevalent in HD, even during the premanifest period.7 Early frontal dysfunction may play a role in predisposing people with HD toward unlawful activities, particularly as criminal and antisocial behavior have been well documented in frontotemporal dementia16,35 and focal frontal lobe injuries.36,37 Impulsivity is another factor that has been associated with involvement in illegal activities.38,39 In HD, higher levels of impulsivity have been linked to aggressive behavior40 as well as executive dysfunction and decreased sensitivity to punishment,6 all of which may increase the risk of engaging in criminal behavior. Alterations in risk and reward appraisal have been implicated in a tendency toward risk-taking in the HD population9,41 and may also lead to involvement in criminal activities. Finally, HD is associated with impairments in emotional processing42 and social cognition43,44 that may play an important role in the development of criminal behavior. Individuals with HD have difficulty recognizing and interpreting emotions, particularly negative emotions such as fear, anger, disgust, and sadness.42 Deficits in theory of mind, or the ability to understand another person's mental and emotional state, have also been demonstrated by individuals with HD43 and have been linked to criminal offenses by individuals with other conditions such as schizophrenia and antisocial personality disorder.45 In summary, HD presents a complex constellation of cognitive and behavioral challenges that together give rise to a unique and multifaceted susceptibility to criminal behavior.
This study emphasizes the complexity of caring for patients with HD from both a medical and a legal standpoint. The spectrum of clinical manifestations seen in individuals with HD highlight the nature of this illness as a quintessential neuropsychiatric condition, blurring the lines between neurological and psychiatric disorders and exposing the limitations of our traditional definitions of these domains. Appropriate management of these patients in both the medical and legal systems requires a true interdisciplinary approach that is based on a careful understanding of the unique vulnerabilities of this population. When considering the emergence of criminal behavior in the context of a neuropsychiatric condition that affects judgment and decision-making, difficult questions regarding free will, intent, and criminal responsibility inevitably arise. The complex intersection between neuroscience and the law has been explored in depth in a number of publications46,–,49 and will not be reviewed here, but we will note that these questions have had direct implications in some prominent cases involving individuals with HD, including a woman who was acquitted of murder after receiving a diagnosis of HD11 and a former physician who, after being convicted of killing his father, is petitioning to be transferred from prison to a psychiatric facility due to HD.10 Another important point to consider is that neurological impairment can at times be misunderstood by law enforcement or mistaken for intoxication or uncooperativeness. This misunderstanding can lead to difficult interactions between individuals with HD and police and may result in inappropriate legal action or incarceration. The Huntington Disease Society of America publishes a Law Enforcement Training Guide to provide education regarding the symptoms of HD and guidance regarding the appropriate management of individuals with HD.50 Over the course of this review, we encountered several instances of DUI citations that had been issued to patients who were assumed to be intoxicated but were subsequently exonerated when this was determined not to be the case. These cases were excluded from our analysis.
This study has several limitations that should be acknowledged. First, our analysis was retrospective and limited to information documented in the medical record. Involvement in illegal activities is a difficult and uncomfortable topic for patients and caregivers to discuss during office visits, and clinicians do not ask about these matters routinely. Furthermore, high-risk behaviors and lawbreaking are not addressed in any of the currently available screening measures utilized for individuals with HD, and these behaviors often go undetected. Therefore, our findings likely represent a significant underestimate of the true prevalence of these behaviors in our clinic population. The keywords selected may have failed to capture the full spectrum of legal involvement experienced in this clinical population, and some patients may have been missed. Some of the patients categorized as nonoffenders may have engaged in illegal activities that were not reported, potentially introducing misclassification bias. Data for this study were collected from an HD Center of Excellence in Nashville, TN, which serves a geographically diverse population of patients with HD from 16 states. Our patients primarily come from the Southeast, Midwest, and Mid-Atlantic regions of the United States, and this sample may not be representative of other regions of the United States. The ethnic diversity of our sample is also limited, as the majority of our HD population is Caucasian. Finally, we did not assess treatment or management of criminal behavior in the scope of this study. Further research is needed to develop improved clinical screening methods for high-risk activities in the HD population and to identify targeted interventions that may reduce the burden of these challenging problems for individuals with HD and their families.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2021 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}