


Abstract
Transporting forensic psychiatric patients outside of forensic hospitals has significant risks that pose competing safety and patients’ rights interests. Psychiatrists and hospital administrators have a duty to keep their staff and the community safe, but this must be carefully balanced with their obligation to uphold the civil rights and liberty interests of their patients. A critical decision in this balancing is whether to utilize security restraints during patient transportation. Addressing these competing interests while striving to safely transport forensic hospital patients to the community can be challenging as hospital staff and patient advocates may voice strong, and sometimes opposing, opinions about this debate. Very little research has been conducted about these high risk and often contentious actions. Here, we describe the process for assessing risk for violence, self-harm, and elopement prior to transportation at one state forensic hospital using a pretransport risk-assessment tool created specifically for that purpose. We then present the results of research identifying which clinical and legal factors identified by our risk-assessment tool correlate with patients being transported with restraints. We also evaluated the potential for racial/ethnic and gender biases in this transportation risk-assessment process.
Forensic psychiatric units or hospitals typically care for individuals with severe mental illness and significant criminal justice involvement who may pose an increased risk of aggression toward others, self-harm, or elopement. The legal status of hospitalized forensic patients usually falls into one of the following categories: not guilty by reason of insanity (NGRI), not competent to stand trial (NCST), incarcerated individuals requiring hospital-level psychiatric treatment (either while incarcerated or at the end of their sentence), and civil patients at significantly heightened risk of violence.1 As a result of these varied reasons for hospitalization, and the varying level of risks for aggression, self-harm, and elopement associated with each,2,–,4 the evaluation of risk and the assigning of appropriate safety measures on the basis of those risk assessments is a part of the everyday work in forensic settings.1
The dual mandate to treat patients in the least restrictive setting and to keep the community safe is an integral component of clinical work in forensic mental health. One of the most notable challenges posed by this dual mandate occurs when transporting hospital patients from forensic units to the community for events such as court hearings or medical treatment. The transportation of prisoners has been identified as one of the highest-risk situations encountered by correctional and law enforcement officers.5 Similarly, transportation of forensic hospital patients, many of whom have been transferred to the hospital from correctional environments, are high-risk events that remove patients from the highly structured and secure inpatient environment and exposes them to a variety of uncontrollable external factors in the community. Unlike correctional environments, where decisions to restrain during transport are typically made by corrections staff (with clinical consultation in some jurisdictions), in the forensic hospital environment these decisions are typically made by clinical staff. Though rare, a psychiatric patient’s escape from an inpatient facility is a serious adverse event that, when it ends in tragedy, can also garner significant public attention.6,–,9
If the hospital’s sole duty were preserving public safety, the simplest and least risky solution would be for the police or other security agency to restrain all patients mechanically during transportation, thus maximally reducing the risk of elopement or aggression. Such practices are typically employed in correctional environments at the discretion of correctional officers. In a hospital setting, this duty to preserve public safety must be balanced, however, against the hospital’s obligation to preserve patients’ liberty interests in not using undue physical restraint. There are multiple regulatory agencies, professional organizations, and legal precedents that establish the right of patients to be treated in the least restrictive manner possible and the mandate that restraint should only be used when necessary because of a significant risk of harm to self or others.10,–,18 These guidelines do not substantively address restraint during transportation, but, recovery-oriented principles suggest that all efforts should be made to treat patients in a person-centered manner that respects their dignity and right to be free from restraint.19 In the hospital, where such decisions are being made by clinical and not security staff, it is important to have an objective way of making determinations about restraint use during transport. Additional operational factors (e.g., the number of staff required for one type of transport versus another) may influence clinical decision-making, but these factors cannot be weighed more heavily than the clinical, legal, and risk-based needs of the patient.
In 2015, Dike et al.20 published the first article to describe a rigorous transportation risk assessment implemented at a forensic psychiatric hospital. Ideally, risk-assessment processes allow for an objective assessment of risk and, through this assessment, permit the balancing of these competing interests by weighing behavioral, historical, and legal risk factors against protective factors (i.e., factors that mitigate risk such as advanced age, medical comorbidities, or a history of treatment compliance) to reach a composite assessment of the individual’s risk. Dike and colleagues extolled the potential benefits of analyzing accumulated results of this risk-assessment process for enhancing our field’s understanding of transportation risk assessment and forensic hospital transport management.20
The intent of this article is to build on this prior work by reporting the analysis of one year of forensic hospital transportation risk-assessment data utilizing an updated version of the risk-assessment tool described in 2015. In this analysis, we examined the impact of various demographic, clinical, and risk factors on restraint utilization during transportation.
Methods
Population
Whiting Forensic Hospital is the state forensic hospital in Connecticut. It is a 229-bed facility consisting of a 91-bed maximum security service and a 138-bed enhanced (medium) security service located in two separate buildings. The hospital treats patients of all four legal statuses described above. The maximum-security service has three competency restoration units, one of which is co-ed, and two all-male long-term treatment units. The enhanced security service consists of five long-term community transition units, one of which is co-ed, and one co-ed competency restoration unit for individuals with low-level, nonviolent charges. Prior to admission, patients are assigned to either the maximum-security service or the enhanced-security service on the basis of several factors, including the severity of their crime, the amount of a court-ordered bond under which they are held, a history of aggressive behaviors, and other relevant medical or clinical history.
Risk-Assessment Procedures
Patients are transported to and from the hospital for a variety of reasons, including court hearings, medical appointments, and therapeutic trips to the community. Prior to these trips, the patient’s risk for dangerousness and elopement is evaluated using a standardized assessment process. Figure 1 presents the hospital’s internally developed risk-assessment form. This form was first developed in 2015 utilizing well-established violence, self-harm, and elopement risk and protective factors, and it was updated in 2019 to include additional evidence-based risk and protective factors. The tool itself, however, is not a validated instrument, and no correlation data were obtained with established risk assessments utilizing validated instruments (e.g., HCR-20), given the time-limited nature of these assessments and the frequency with which they must be conducted. The risk-assessment form typically is completed by the patient’s attending psychiatrist within 48 hours of scheduled transports. Psychiatrists are instructed to complete the risk-assessment tool on the basis of the patient’s history and their clinical assessment of the patient (using input from other clinical team members); no formal training in its completion is provided. Transport levels can be as restrictive as four-point mechanical restraint with leg irons, waist belt, and handcuffs in the presence of two hospital police officers and one clinical staff member, or as permissive as unrestrained transport in the presence of one clinical staff member. In the enhanced-security service, for those patients with a privilege level that allows them to leave the building or hospital grounds with staff, risk-assessment forms are not completed for each transport occasion off grounds but rather on a regular schedule, usually at the monthly treatment plan meetings or following a sudden change in their clinical or legal status. Such patients typically have demonstrated progressive reduction in risk over time and, thus, have sufficient sustained clinical stability to not require such an in-depth assessment prior to each transport out of the enhanced-security building.
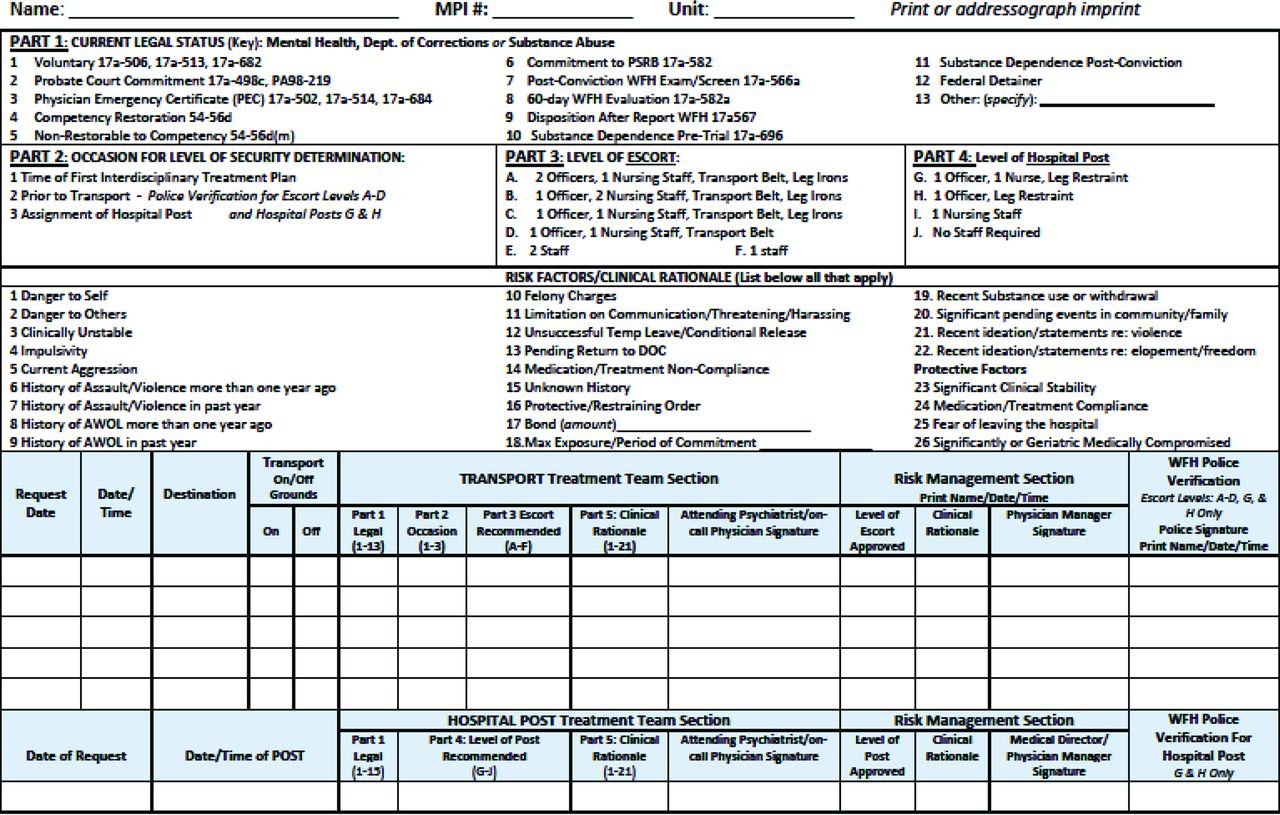
The risk assessment for transportation form.
The transport level recommended by the treating psychiatrist is reviewed and approved by the hospital medical director or assistant medical director in the daily hospital-wide risk management meeting. If either of these individuals does not agree with the level of transport recommended by the attending psychiatrist, they will engage in a discussion with the psychiatrist to understand the differences and attempt to reach consensus on the transport level. If consensus cannot be achieved, the medical director will review the information. If the medical director recommends a transport level that differs from that recommended by the clinical team, the medical director will communicate this to the clinical team, including an explanation for the change.
Data Collection and Analyses
This project is a retrospective review of transportation risk-assessment data collected as part of the hospital’s quality assurance and clinical operations. While the transportation risk-assessment process had been in place since 2015, prior to 2019 there was no systematized mechanism for collecting and storing this data. In 2019, a database was developed to understand this process better. The dataset included information about every transport event for Whiting Forensic Hospital for 2019. The variables in the database were all those on the risk-assessment form (Fig. 1), including the patient’s legal status, occasion for level of security determination, level of escort recommended and approved, clinical rationale (i.e., risk and protective factors) for the level of transport, date and time of the transport, location of the transport, recommending psychiatrist, and approving medical director. For the purposes of this manuscript, the primary endpoint was whether restraint was used during patient transport. Thus, in our data analyses, all degrees of restraint transport (levels A through D in Fig. 1) were combined into one “Restraint Use” group, and all transports occurring only with one or two clinical staff (levels E and F) were combined into a “No Restraint Use” group.
Patients’ primary diagnoses were also included in the database. Although rates of comorbidity among this patient population are high, additional diagnoses were not added because of the complexity of drawing meaningful conclusions from such analyses when patients routinely have three to five diagnoses listed in the medical record.
Protected health information that was collected originally as part of the database was removed prior to the start of analyses for this project. As there was no protected health information included in the analyzed dataset, the project was exempted from review by the institutional review boards of Yale University and the Connecticut Department of Mental Health and Addiction Services.
Data regarding race/ethnicity were not included in the database originally because this information is not collected during the risk-assessment and transportation process. To better understand the potential impact of racial/ethnic bias on the use of restraints during patient transportation, the authors received institutional review board approval to collect this data retrospectively, add it into the database, and then de-identify the revised database. The race/ethnicity data available for inclusion in the database were collected at the time of the patient’s admission to Whiting Forensic Hospital. This information is coded into a limited set of categories: Alaska Native, American Indian, Asian or Pacific Islander, Black or African American, Hispanic, Native Hawaiian, Two or More Races, White or Caucasian, Not Collected, Other, Refused, or Unknown.
As some patients were transported multiple times, there were 821 transport events for 260 distinct patients. Of the 821 transportation risk-assessment records collected, 19 records were not included in the analysis as they were incomplete; the remaining 802 records were analyzed. Descriptive statistics were calculated for all variables of interest. Given the lack of independence between observations, no inferential analyses could be conducted. The data were analyzed using Microsoft Excel (Redmond, Washington).
Results
There was an average of 3.2 transports per patient, with a range of 1 to 31 transports and a median of 2 transports per patient. As detailed in Table 1, 443 (55.2%) transport events used some form of mechanical restraint. To assess if there was a trend toward increasing or decreasing use of restraints, the calendar year was divided into three-month sections and the results were compared. There was no apparent trend (data not shown), although the timeframes selected may be too short to demonstrate such a trend. As the vast majority of transport destinations were medical appointments in the community, this variable was not further analyzed as meaningful differences between transports could not be discerned.
Demographic and Legal Status Factors Related to Use of Restraint during Transport
A total of 683 transports were for male patients; of those transports, 55.2 percent required restraints. Similarly, 55.5 percent of the 119 transports of female patients required restraints. Most transports (n = 568) were for patients less than 60 years old; of those transports, 62.9 percent used restraints. In contrast, only 36.8 percent of the 234 transport events for patients more than 60 years old used restraints.
The racial breakdown of transport events was as follows: 44.8 percent White or Caucasian (hereafter White), 34.5 percent Black or African American (hereafter Black), and 19.7 percent Hispanic; Alaska Native and Asian or Pacific Islander each represented less than one percent of all transport events. This approximates the average racial breakdown in the hospital during that calendar year: 50 to 51 percent White, 33 to 35 percent Black, 13 to 16 percent Hispanic, and 1 percent all other races/ethnicities.
As there were only seven Asian/Pacific Islander–identified patient transport events and one Alaskan Native–identified patient transport event, the sample size of those groups was too small to compare them meaningfully with the larger groups. For the remaining groups, the total transports of the Black group had the highest proportion of restraint use, with 61.0 percent requiring the use of restraints. In the Hispanic group, 57.0 percent of transports required restraints; the White group had the lowest proportion, with 49.3 percent of transports requiring the use of restraints.
The legal status of the patients who were transported was sorted into five categories: voluntary civil patients (from community hospitals or end of sentence transfers from the Department of Correction, n = 49 transports); competency restoration patients (n = 397 transports); civilly committed, which included those civilly committed to the hospital from the Department of Correction who required a hospital-level of care (n = 146 transports); NGRI acquittee (n = 205 transports), and Other, which included individuals hospitalized for other court-ordered evaluations, such as postadjudication presentencing evaluation (n = 5 transports). Restraint use was lowest among the voluntary group (20.4%), followed by civil (38.4%), NGRI (47.3%), competency (69.3%), and Other (100%).
For patients receiving competency restoration services, 69.3 percent of the transport events required the use of restraints, compared with only 41.0 percent of all other patients. Among competency patients, 92.9 percent of patients transported from the maximum-security service were transported in restraints, while only 56.3 percent of competency patients from the enhanced-security service were restrained during transport. For noncompetency patients, 60.6 percent of transports from the maximum-security service required restraints, while only 5.7 percent of transports from the enhanced-security service required the use of restraints. This trend reflects the use of the maximum-security service for patients who are known to the hospital to have higher risk profiles (i.e., typically reserved for competency restoration patients with more violent charges or an increased clinical risk for violence).
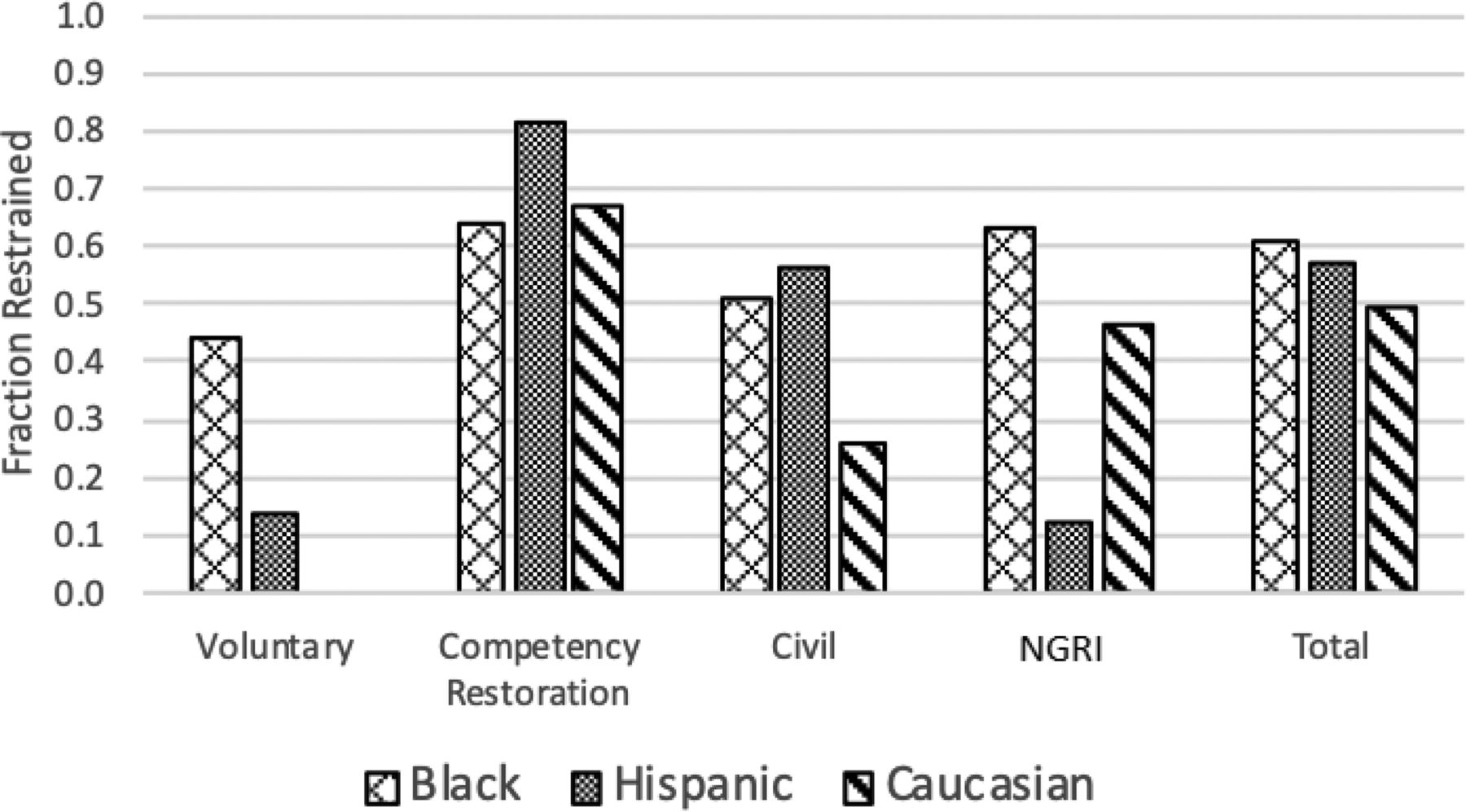
Figure 2 shows the fraction of transport events requiring restraint sorted by race and by legal status. The racial breakdown of each legal status was as follows: voluntary (33% White, 37% Black, 30% Hispanic), civil (56% White, 27% Black, 17% Hispanic), competency (41% White, 37% Black, 22% Hispanic), NGRI (49% White, 35% Black, 16% Hispanic), Other (50% White, 50% Black). Overall, restraints were utilized more often among Black and Hispanic patients than among White patients. These differences are most notable among voluntary civil patients (the smallest legal status sample), where Black patients were restrained in 44.4 percent of the transport events and Hispanic patients were restrained in 13.3 percent of the transport events; none of the transport events involving White voluntary civil patients used restraints. Racial disparities in restraint use also were noted among civilly committed patients (51.3% Black, 56.0% Hispanic, and 25.9% White) and NGRI patients (63.4% Black, 12.5% Hispanic, and 46.5% White). This trend was not observed among competency restoration patients, where restraints were utilized most in Hispanic patient transports (81.4%), followed by White patient transports (67.1%) and then Black patient transports (63.9%).

Fraction of transports that required restraints by race and legal status.
Dividing the sample by both race/ethnicity and legal status left smaller sample sizes, increasing the potential that a small number of patients who were transported many times could bias these results. To evaluate this possibility, we removed the individual patient with the greatest number of transports from each group and recalculated the fraction of transport events that used restraints for each group. Removing the most frequently transported patient from each group did not substantively change any of the results (data not shown).
Table 2 presents the primary diagnostic categories of the patients in each of the transport events. The majority of the patient diagnoses were in the schizophrenia spectrum disorders category, which totaled 56.6 percent of all those transported. The neurocognitive disorders category totaled 12.7 percent of all those transported. When comparing these two populations, it appears there was a trend toward less restraint use in the neurocognitive disorders group (36.3% restraint use) than in the schizophrenia spectrum group (55.9%). The diagnostic categories with the highest percent of restraint use were depressive disorders (84.6%), trauma and stress-related diagnoses (80.0%), and no diagnosis (83.3%). The no diagnosis category simply indicates that no diagnosis had been recorded in the electronic database at the time of transport, not that an individual was not eventually assigned a diagnosis.
Diagnostic Categories Related to Use of Restraint during Transport
Table 3 presents the risk and protective factors that were included in transportation risk assessments. The assessment factors were categorized into behavioral risk, historical risk, legal/social risk, and protective factors. Not surprisingly, assessments that indicated the use of restraints included more behavioral, historical, and legal/social risk indicators, whereas those that did not indicate the use of restraints included more protective factors.
Risk Factor Categories Related to Use of Restraint during Transport
Of the 802 transport events studied, a medical director changed the recommended level of transport in only six cases (0.7%). In two cases, there was no change in rationale, but the level of transport was lowered from one involving restraints to one not involving restraints. In one case, an additional risk factor was added, and the transport level was increased to involve restraints. In two cases, the recommended rationale was substituted with a different rationale, in one case lowering the transport level to not include restraints, and raising it to include restraints in the other case. In the final case, it was unclear from the data why the rationale was changed, and the change had no impact on restraint use.
Hospital adverse event data were queried for any adverse events that had occurred during patient transportation (e.g., patient elopement, aggression, self-harm, patient falls, or physical injuries due to use of security restraints, etc.) for the year studied. Notably, there were no adverse events reported during this timeframe related to patient transport to or from the hospital. The lack of negative occurrences precluded any analysis of factors that contributed to, exacerbated, or protected against such events.
Discussion
This paper, expanding on the work by Dike et al.,20 represents the first published manuscript to describe the systematic analysis of the use of a risk-assessment tool and associated restraint utilization in the transportation of hospitalized forensic psychiatric patients. Much of what the data revealed was consistent with the authors’ expectations. Greater numbers of behavioral, historical, and legal risk factors were identified on the risk-assessment tool as the rationale for restraint utilization, and more protective factors were identified when restraints were not used. Restraints were utilized more often among patients who were younger, residing in the maximum-security service, and hospitalized for competency restoration. This latter finding is not surprising given that competency restoration patients are generally newer to the hospital; thus, their acuity may be higher, and their risks not as well understood. The higher use of restraints in maximum security is also not surprising given the use of the maximum-security service for patients who are known to have higher risk profiles. Only 5.7 percent of noncompetency patients outside of the maximum-security service required the use of restraints. When comparing the two largest diagnostic groups, it appears there was a trend toward greater restraint use in those with schizophrenia spectrum disorders compared with those with neurocognitive disorders (the second largest diagnostic group), which is not surprising, especially as geriatric status is a protective factor identified on the risk-assessment tool. It is, however, difficult to draw meaningful conclusions from differential findings in restraint use by diagnosis, given that the schizophrenia spectrum disorder category accounted for more than half of the transport events, with most other diagnostic groups representing a small fraction of overall total transport events.
Prior to conducting the study, there was a perception among some hospital staff that the hospital leadership frequently overturned the recommendation of the clinical teams in a manner that was potentially unsafe. These findings demonstrate that this was not the case, as the recommended level of transport was changed in less than 1 percent of cases. This finding supports an assertion that there is a high degree of consistency in the threshold employed for restraint use during transport by both clinical staff and hospital leadership. Also, in the few instances where the mode of transport was changed, the rationale for doing so was clear in all but one case. Further, of 802 transport events, there were zero adverse events, suggesting that the thresholds that were used adequately protected the safety of patients, hospital staff, and the community. This suggests that such a clinically driven risk-assessment process may be a safe and effective tool for forensic units to use to determine appropriate restraint application during patient transportation. It must also be considered, however, that this process may be overly restrictive in favor of safety and that less stringent risk-assessment processes could result in lower restraint utilization yet still achieve similar safety outcomes. To test this hypothesis, the system would have to be willing to tolerate the potential for increased risk to these same stakeholders, which is a challenging proposition to consider.
This study explored disparate restraint use and bias across multiple parameters. As the percentages of transports that required restraints were similar for male and female identified patients, we did not identify a gender bias in the use of restraints. The data did, however, demonstrate a potential racial/ethnic bias in the use of transportation restraints, as Black and Hispanic patients were restrained more than White patients overall and among all but one legal status group. This finding is concerning and warrants additional inquiry to better understand its meaning and to identify other factors (e.g., legal or clinical) that may contribute to these disparate practices. For example, a difference was not seen as readily among competency restoration patients (making up just under half of the total transportation events), where Hispanic patients were restrained the most, but there was no difference in restraint use between Black and White patients. Unfortunately, because the unit of measure studied was transport events as opposed to individual patients, more detailed inferential analyses correlating the relationships between race, legal status, and risk factors could not be conducted because of concerns that duplicated patients (i.e., patients who were transported multiple times) could unduly influence the results. Thus, it is unclear from these data if the biases we identified were due to factors intrinsic to the hospital’s risk-assessment process, upstream effects originating in the legal system, or even further upstream effects from the social determinants of health, socioeconomic biases, and criminogenic risks in the communities served.21,–,23 Whatever the causes, better understanding this bias and taking proactive steps to strive for unbiased evaluation and restraint practices are important quality improvement measures that must result from this work, both for the hospital and for the field as a whole, and requires further study.
This study has notable limitations. First, analyzing the total number of transport events, as opposed to the total number of patients transported, introduces the potential for bias as some patients were transported more than others. The purpose of this study, however, was to show the full population of transport events, not the population of individuals transported, as a variety of clinical and other factors may influence a patient’s risk level over time. For example, a patient’s risk level may fluctuate such that transportation restraint is required at one point during the hospitalization, but not at another. Second, as data of transport events were collected from only one institution implementing only one risk-assessment method, the authors are limited in their ability to generalize these findings to other similar settings. The authors hope to conduct additional studies that allow for greater inferential analyses so we can better understand the significance of these findings. Third, the lack of adverse events during the study period precluded any analysis of factors that may have contributed to, exacerbated, or protected against such events. The absence of any such events raises questions about the threshold for security restraint utilization and warrants further investigation, recognizing that the potential risks to patients’ autonomy must be weighed against risks to others and considered within the historical context of similar past events in the local community. In addition, this study only included one year of data, and it was the first year that such risk-assessment data were collected systematically at the hospital. Data collection and analysis over a longer duration may prove beneficial, particularly when assessing for the frequency of less common adverse events and their corollaries.
Conclusion
This study of one year of security restraint utilization during the transportation of forensic hospital patients identified several important findings. Clinical, historical, and legal factors were closely linked to restraint use, where a greater number of protective factors mitigated the need for its use. These findings also reinforce commonly understood clinical axioms that greater familiarity and time to work with patients (e.g., as observed with NGRI patients who have much greater lengths of stay in the hospital compared with competency patients) may allow for enhanced symptom management and more refined clinical risk assessment, both of which may have contributed to the reduced need for restraint use seen in this NGRI population. Racial or ethnic bias was identified, though its underpinnings remain unclear and require additional study. This study further supports the assertion that forensic units or hospitals that employ similarly rigorous, clinically informed, and systematic yet individualized transportation risk-assessment processes can fulfill their obligation to balance patients’ liberty interests with public safety.
Footnotes
All authors receive salary support from the Connecticut Department of Mental Health and Addiction Services, but this publication does not represent the views of the Department of Mental Health and Addiction Services or the State of Connecticut. The views and opinions expressed are those of the authors. Dr. Wasser is involved in the editorial leadership of The Journal; however, he did not participate in any aspect of this article’s review and acceptance.
Disclosures of financial or other potential conflicts of interest: None.
- © 2022 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}