


Abstract
Inmates have high rates of opioid use disorder and are at risk for morbidity and mortality both during incarceration and after release. We conducted a retrospective chart review to assess prescribers’ fidelity to the New Jersey Department of Corrections practice guideline for prescribing maintenance or prerelease buprenorphine. We compared the entire group of inmates prescribed buprenorphine at the conclusion of 2019 (n = 875) with a sample of inmates diagnosed with opioid use disorder (OUD) but not prescribed buprenorphine (n = 396) and a sample of inmates not diagnosed with OUD (n = 367). Inmates on buprenorphine were more likely to be male, White, in treatment for a mental illness, have higher scores on the Texas Christian University Drug Screen, be closer to release, have multiple substance use disorder comorbidities, and have more substance-related disciplinary charges. They were most often prescribed buprenorphine-naloxone strips, with doses ranging from 2 mg to 12 mg, and a median dose of 8 mg. Racial disparities in prescribing were observed, though the reasons for this are likely multifactorial, and research from the community has shown similar findings. We propose strategies to reduce these differences, including staff education, patient education, and quality improvement initiatives.
The opioid epidemic is widespread and deadly throughout the United States.1,2 Substance Use Disorders (SUDs) are highly prevalent in incarcerated individuals, with rates even higher in those with mental illness. The Bureau of Justice reported that 74 percent of inmates with current or historical mood or psychotic symptoms had any SUD, compared with 56 percent of inmates who did not have these symptoms.3 Approximately 17 percent of state prisoners report a history of regular use of opioids.4
Opioid use disorders (OUDs) in prisoners have effects that reach out into our communities. Along with causing legal entanglements, OUD exposes these individuals to many adverse health and social consequences, including human immunodeficiency virus (HIV), Hepatitis C infection, unemployment, and family problems. Former inmates with OUD often resume using opioids upon release, with a substantial risk of overdose death, especially in the early weeks after release.5,–,7
Medications for Opioid Use Disorder (MOUD), including buprenorphine, are widely regarded as effective treatments, with evidence supporting reducing drug use, criminal activity, and mortality.8 Research supports a reduction in overdose mortality for recently released inmates prescribed MOUD.9 Two recent and large systemic analyses support providing buprenorphine for inmates during incarceration to reduce recidivism, as well as to reduce the risk of mortality both during and after incarceration.10,11
Nevertheless, the criminal justice system has been slow to adopt buprenorphine as an in-house treatment for inmates with OUD.12,13 Prescribed buprenorphine is a commonly misused substance in prison settings.14 Buprenorphine is a controlled substance that is frequently smuggled into correctional settings, so abuse and diversion are concerns for custody and administrative staff.13 Though state departments of corrections are increasingly offering buprenorphine, the vast majority do not.15 In the meantime, opioid overdose is the third leading cause of death for inmates during incarceration, and simply referring an inmate for OUD treatment upon release is unlikely to result in the former inmate accessing MOUD.16,17
Rutgers University Correctional Health Care (UCHC), the New Jersey Department of Correction’s (NJDOC) health care vendor, has an evolving guideline for the treatment of SUDs that includes medication management for OUD. All UCHC prescribers were mandated to obtain a DATA 2000 X-waiver in 2014.18 With the approval and support of the NJDOC, the guideline has developed to allow the prescription of a full range of MOUD options, including oral naltrexone (2012), long-acting injectable naltrexone (2016), buprenorphine (2017), and methadone (2019), though regulatory requirements limit UCHC’s use of methadone.
When buprenorphine was made available to inmates with OUD in the NJDOC, it was initially intended for preparing individuals with opioid use disorder to more safely return to the community. By 2018, inmates with longer time remaining in their sentence were also considered eligible for MOUD should it be clinically determined that they may benefit from the treatment. Examples include inmates who have experienced health risks or repeated disciplinary problems related to ongoing opioid use during their incarceration. While instructions for providers about buprenorphine prescription were informed by SAMHSA guidelines, until recently, they did not include specific direction for prescribing to persons in prison, the majority of whom are not currently dependent on opioids.19 Thus, the guideline required adaptation for prison work.
The UCHC guideline for the treatment of substance use disorders calls for an assessment on intake using the Texas Christian University Drug Screen V (TCU-DS), entering specific substance use disorder diagnoses into the inmate’s electronic medical record (EMR) problem list and limiting the prescription of buprenorphine to those diagnosed with an OUD. It recommends lower induction doses than would typically be used in the community for those presenting in withdrawal and the use of buprenorphine-naloxone strips. While available and on formulary, buprenorphine tabs (without a naloxone component) are not preferred because of a higher risk for diversion.20,21 In the NJDOC, MOUD is prescribed by a psychiatrist or a psychiatric advanced practice nurse if the patient is on the Mental Health Special Needs Roster (MHSNR) and otherwise by a general medical provider or medical advanced practice nurse. Inmates on the MHSNR have a mental health disorder that impairs their functioning in prison and requires treatment. A diagnosis of SUD by itself is insufficient to require treatment on the MHSNR.
The guideline’s recommended dose of buprenorphine for most inmate patients is between 4 and 8 mg per day. The rationale for this recommendation is research suggesting that doses of buprenorphine less than 4 mg per day are unlikely to suppress withdrawal symptoms.22 While doses much higher than 8 mg are typical in the community, that upper limit was chosen based on research suggesting that lower induction doses for nontolerant prisoners were appropriate, and experience to that point suggesting that it was adequate to suppress cravings for most individuals with relatively limited access to illegal opioids.23,24 Long-acting injectable (LAI) buprenorphine is also available, though its use is restricted because of cost. While accessible through the nonformulary process, approval of LAI buprenorphine is limited to those patients anticipated to transfer to a halfway house setting. Halfway houses in New Jersey are not equipped or staffed to store, administer, and monitor controlled substances, so residents of these settings must return to a parent prison site to have each dose administered. Thus, a monthly buprenorphine injection is more operationally practicable than a daily dose of buprenorphine.
By the end of 2019, there were 875 inmate patients prescribed a buprenorphine product in the NJDOC. According to publicly available data, the NJDOC census on January 1, 2020 was 18,477 inmates, so 4.7 percent of the inmate population was prescribed buprenorphine at that time.25 To our knowledge, the NJDOC had the largest number of inmates receiving buprenorphine in the United States in 2019, even more than in the Rhode Island Department of Corrections, which is regarded as the model U.S. prison system for providing MOUD.26
Methods
We began this work as a performance improvement project with an objective to evaluate fidelity of buprenorphine prescribing to our internal UCHC Practice Guideline for the Treatment of Substance Use Disorders. We intended to describe demographic, clinical, and institutional features of inmates receiving buprenorphine and to compare them with those of individuals with OUD who were not prescribed buprenorphine and also with inmates who are not diagnosed with OUD. Given the large number of persons treated for OUD within the NJDOC, we determined that the initial results of our performance improvement project had wider interest. Our project was approved as research by the Rutgers Robert Wood Johnson Institutional Review Board and the NJDOC Departmental Research Review Board. Immediately after approval, our data set was de-identified by removing all protected health information.
We completed a retrospective chart review of the practice of prescribing buprenorphine in the NJDOC in the year 2019. The principal study group consisted of individuals on a report generated by the (AthenaHealth GE Centricity) EMR of all NJDOC inmates prescribed a buprenorphine product as of December 31, 2019. The reason we included this group in its entirety was for the descriptive value. We selected two comparison groups of a combined approximately equal size to the study group. The first was a random sampling of NJDOC inmates who have a current diagnosis of opioid use disorder yet were not prescribed buprenorphine on December 31, 2019. The second comparison group was a random sampling of NJDOC inmates who did not have a diagnosis of OUD. (We did not calculate the point prevalence of OUD in the NJDOC at the time of the project, but internal UCHC continuous quality improvement data suggest that approximately 20% of NJDOC inmates have a diagnosis of OUD, which is similar to other published estimates.)4
From the EMR, investigators collected the following data for inmate patients with OUD who were prescribed buprenorphine: name, identification number, age, gender, mental health treatment (MHSNR) status, anticipated date of release, the date of initiation of buprenorphine, the form and dose of buprenorphine, and current substance-related diagnoses. For both comparison groups, investigators collected from the EMR name, identification number, age, gender, MHSNR status, anticipated date of release, and current substance-related diagnoses. For those not prescribed buprenorphine at the end of 2019, investigators checked if it had been prescribed (and stopped) during the year and recorded the reason for discontinuation, if known. If subjects were prescribed nonpreferred forms of buprenorphine, the reason for this choice was also collected from the EMR, if known.
For each case reviewed, we also checked the NJDOC’s offender management system database iTAG (institutional TAG; TAG is not an acronym), which more reliably stores information on race, the most recent TCU-DS score, and the disciplinary charges related to substance use that occurred in 2019, including the date(s) of the infraction(s).27 Information on race in iTAG was collected from various sources, usually entered at booking in the county jail, and is typically recorded to reflect inmate self-report. iTAG collects TCU-DS information both from clinical and nonclinical sources. Drug-related charges include the following designation codes in New Jersey regulations: 203: Possession of Prohibited Substances; 204: Use of Prohibited Substances; 205: Misuse of Authorized Medication; 215: Distribution of Prohibited Substances; 258 through 261 (refusal of testing related to suspected drug use); 551: Making Intoxicants; and 552: Being Intoxicated.28 Misuse of authorized medication is used when an inmate is observed not taking a prescribed medication as directed (e.g., not swallowing it if prescribed orally, or not applying it under the tongue if prescribed sublingually). Prohibited substance charges refer to misconduct related to illegal drugs like heroin. If the disposition of the charge was “Not Guilty,” these data were excluded. If the inmate was in the main study group prescribed buprenorphine, we noted if the institutional charge happened before medication initiation, happened concurrently while it was being prescribed, or if there were multiple charges, if they were incurred both before and after buprenorphine was started.
Statistical Analysis
Analysis of differences of categorical variables (such as race) was made using a chi-square test, with post hoc residuals to identify significance of contributions from contingency table blocks. Significant positive residuals are reported. Continuous variables (such as TCU-DS scores) were analyzed using one-way ANOVAs with post hoc Tukey HSD tests. Pairwise comparisons (such as getting a disciplinary charge before or after starting buprenorphine) were done using the Fisher’s Exact Test. Groups present in 1 percent of the sample or less were excluded from statistical analyses. Life sentences were not included in calculating the average time remaining in an inmate’s sentence. Statistical significance was set a priori at p < .05.
Results
Demographic variables are shown in Table 1. For the buprenorphine group (n = 875), the average age was 37.1 years, 97.7 percent were male, and 67.3 percent were White, 17.0 percent Black, 13.9 percent Hispanic, 1.0 percent Asian, and 0.2 percent another race. In the OUD comparison group (n = 396), the average age was 36.4 years, 93.2 percent were male, and 57.1 percent were Black, 29.5 percent White, 12.1 percent Hispanic, 0 percent Asian, and 0.5 percent another race. In the control group without an OUD diagnosis (n = 367), the average age was 38.1 years, 95.6 percent were male, 64.0 percent Black, 19.1 percent Hispanic, 15.3 percent White, 1.4 percent Asian, and 0 percent another race.
Demographic Variables
While age was similar between comparison groups (ANOVA p = .07), significant differences were found by gender and race. Significant racial differences included greater numbers of White inmates on buprenorphine (df = 4, χ2 = 398.1, p < .001, z = 9.0), Black inmates with OUD but not prescribed buprenorphine (z = 6.4), and Black and Hispanic inmates not diagnosed with OUD (z = 8.5, z = 2.1 respectively). In terms of gender, differences were driven by a greater proportion of women in the group diagnosed with OUD but not prescribed buprenorphine (2.3% of group prescribed buprenorphine were women versus 6.8% of the group with OUD but not prescribed buprenorphine; df = 2, χ2 = 15.4, p < .001, z = 3.0).
Comparison of clinical variables between those prescribed buprenorphine and those not prescribed buprenorphine or those without a diagnosis of OUD are shown in Table 2, Figure 1, and Figure 2. Those prescribed buprenorphine were more likely to be on the MHSNR (48.4%) compared with OUD diagnosis (33.6%) and no OUD diagnosis (16.1%) (df = 2, χ2 = 125.6, p < .001, z = 5.42) and were more likely to have a higher TCU drug score (8.2) compared with 6.1 and 1.5 for the other groups (ANOVA p < .001, post hoc Tukey HSD P < .01 all comparisons). Whether prescribed buprenorphine or not, those with OUD were more likely to have use disorders for three or more substances (49.4%) compared with 53.5 percent and 6.5 percent for the other groups (df = 2, χ2 = 231.3, p < .001, z = 4.0 for both OUD groups). The most common substance-related comorbidities for those with OUD were stimulants, cannabis, alcohol, and sedatives, each with statistically significant differences.
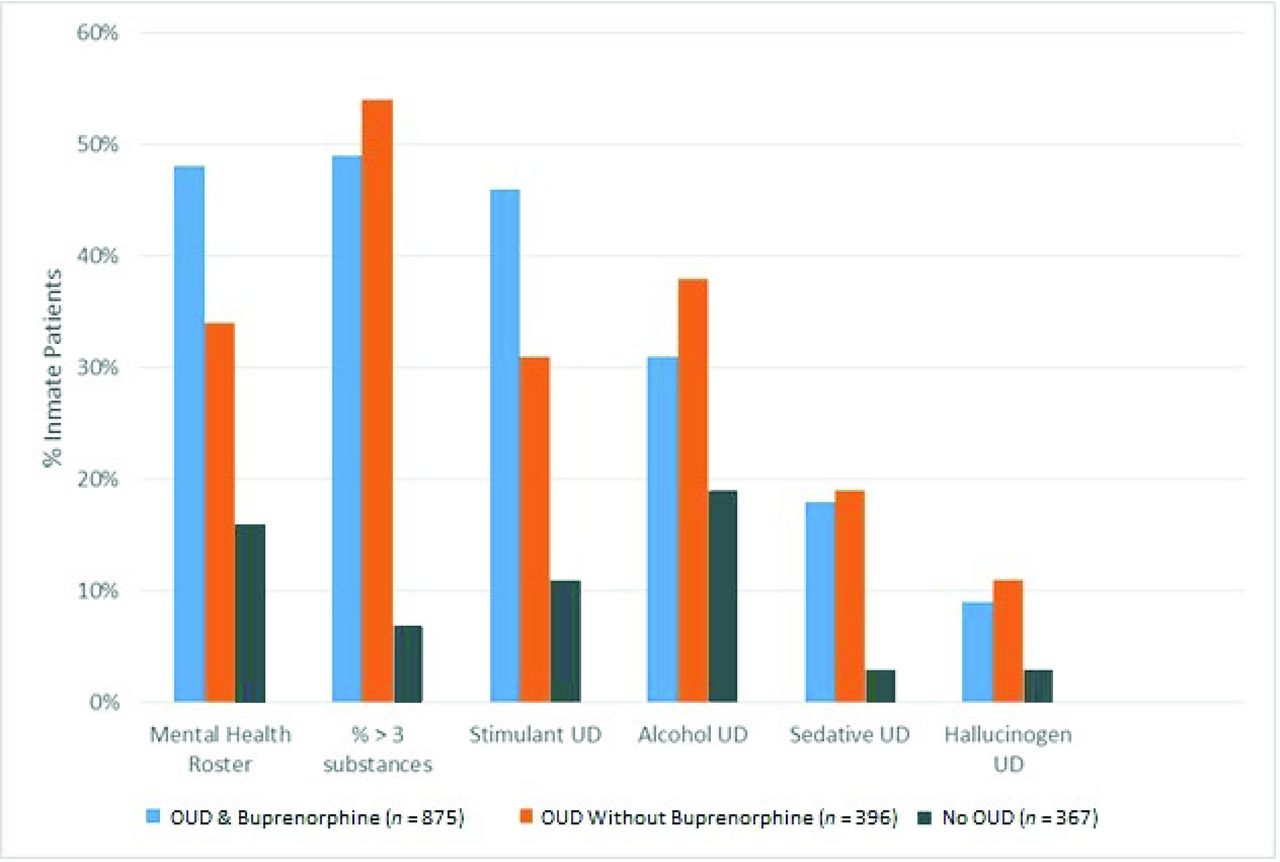
Clinical Variablesa; OUD = Opioid Use Disorder; UD = Use Disorder; aAll categories p < .001.
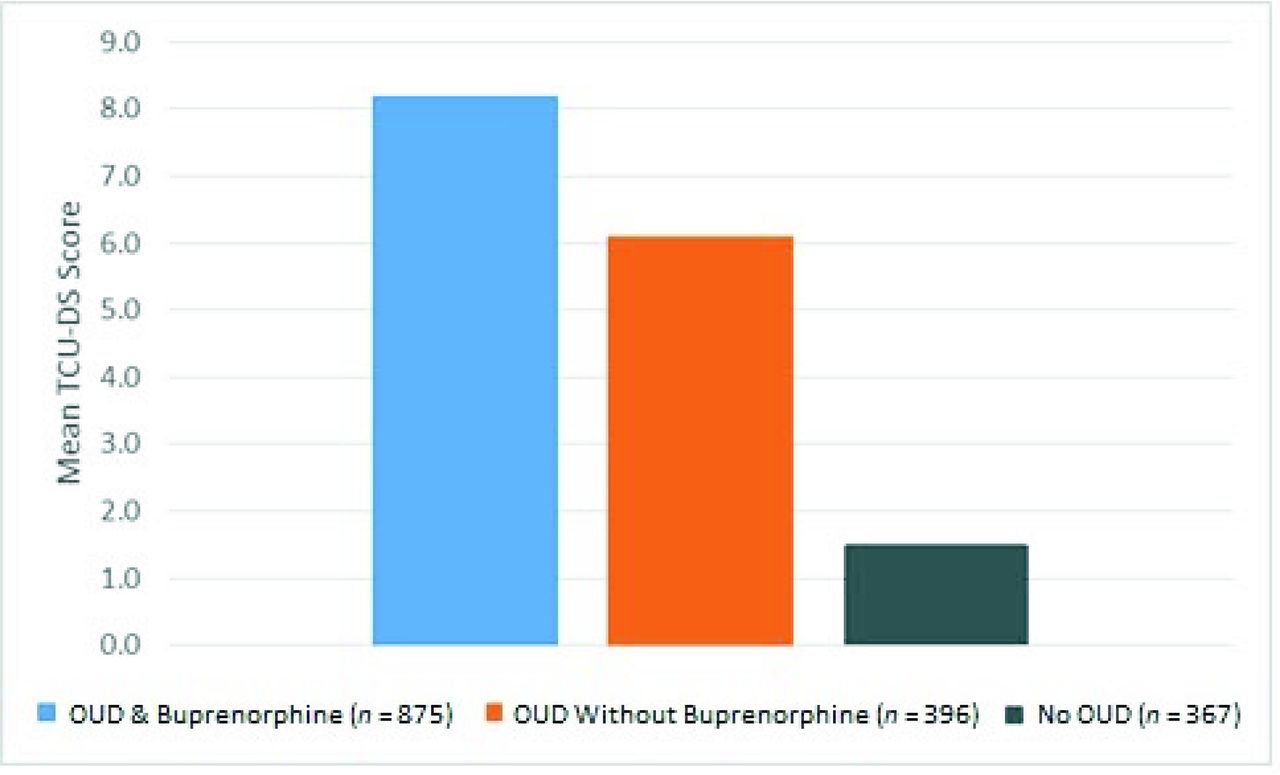
Mean TCU-DSa; TCU-DS = Texas Christian University Drug Screen; OUD = Opioid Use Disorder; UD = Use Disorder; ap < .001.
Clinical Variables
Most inmates prescribed buprenorphine were on buprenorphine-naloxone films (85.9%), while 10.1 percent were on buprenorphine without naloxone, and 4.0 percent were prescribed LAI buprenorphine. Excluding LAIs, the average and median doses of buprenorphine were 7.5 mg and 8 mg respectively, with a range of 1 mg to 14 mg. When prescribed for at least 90 days (as with 64.8% of the main buprenorphine group), the average and median doses of buprenorphine were 8.4 mg and 8 mg respectively, with a range of 2 mg to 12 mg. A graphical representation of the dosing frequency of buprenorphine as of December 31, 2019 is seen in Figure 3 Of those on established doses of buprenorphine (prescribed for at least 90 days), 8 mg was the modal daily dose, but 1.5 percent were on less than 4 mg and 27.2 percent were on higher than 8 mg.
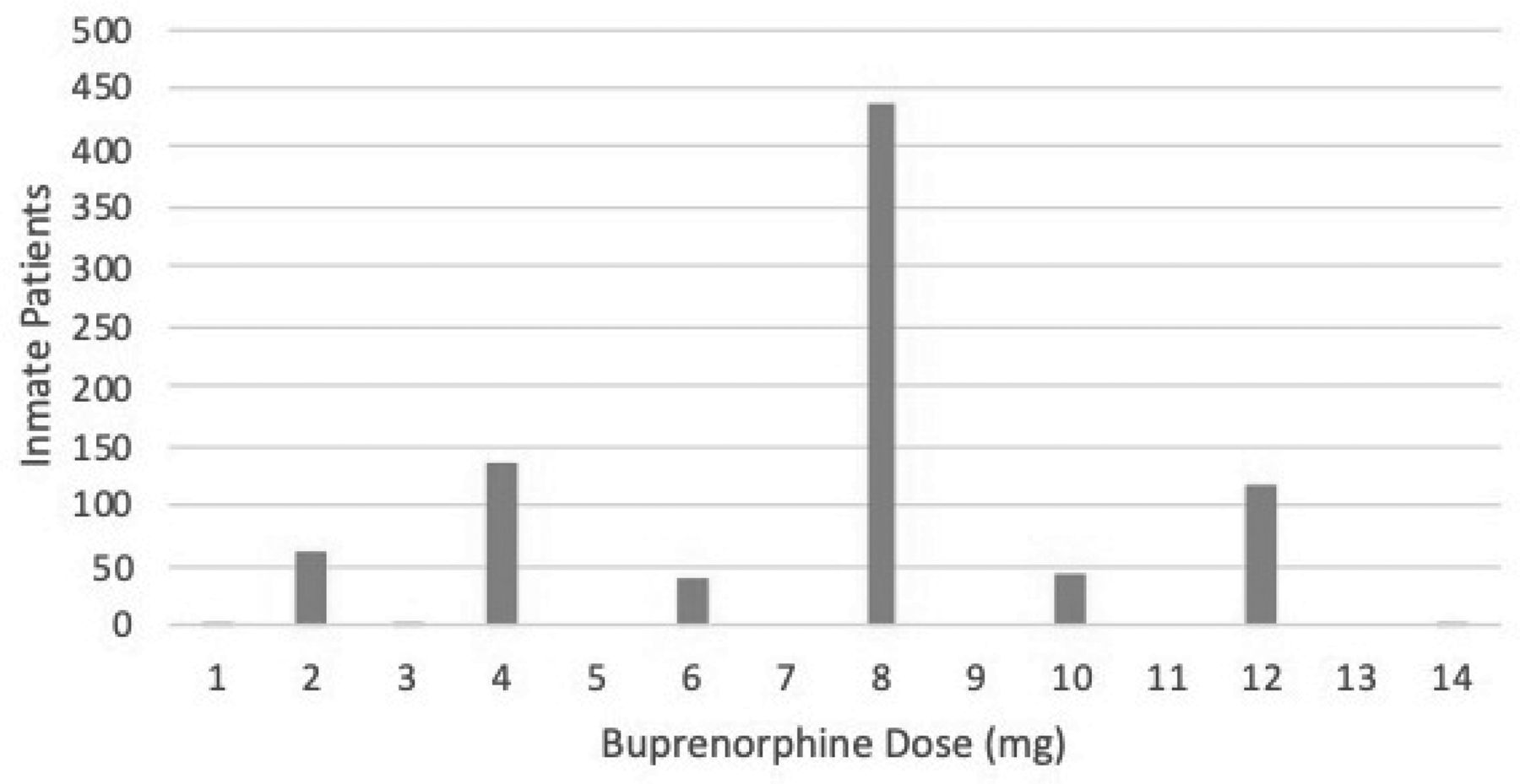
Buprenorphine Dosage Frequencies on December 31, 2019 in the NJDOC.
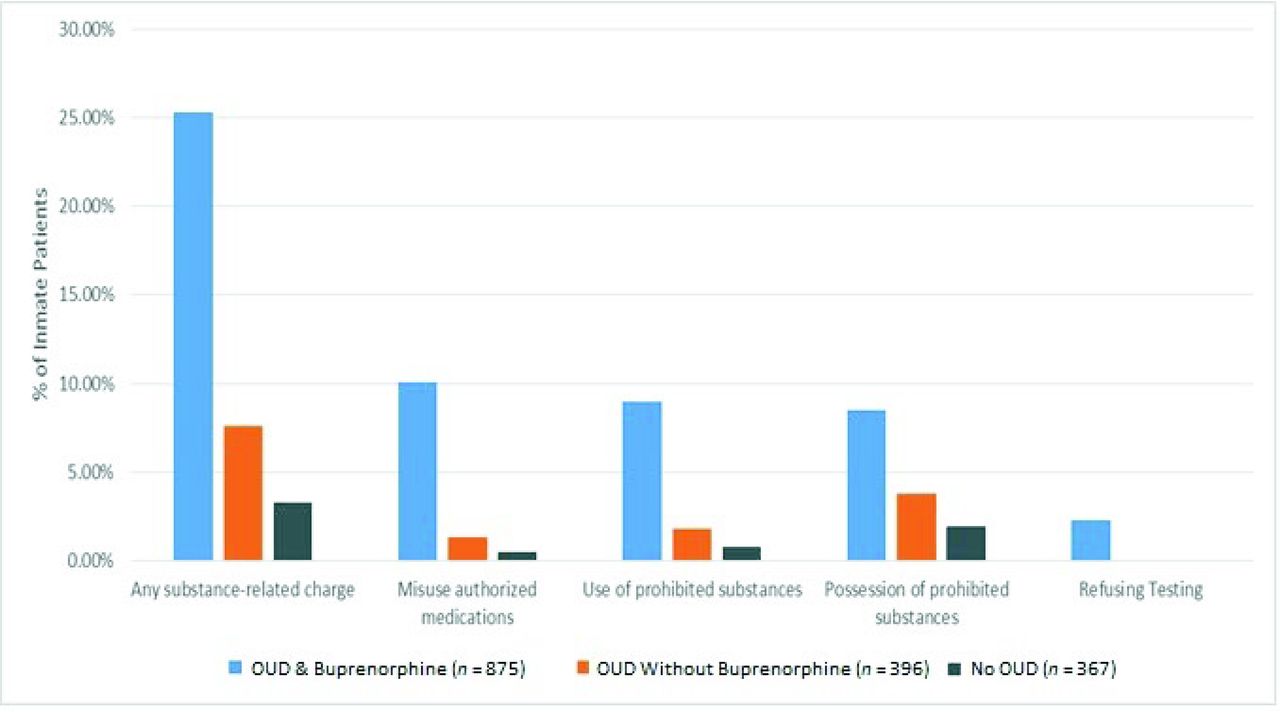
Comparison of institutional (disciplinary) variables between groups is shown in Table 3 and Figure 4. Those on buprenorphine were closer to community release (2.1 years) than those with OUD but not prescribed buprenorphine (3.1 years), who were closer to release than those without a diagnosis of OUD (4.9 years, ANOVA p < .001, post hoc Tukey HSD p < .01 all comparisons). Those prescribed buprenorphine were more likely to have a substance-related institutional charge (25.3% versus 7.6% for those not on buprenorphine and 3.3% for those not diagnosed with OUD) (df = 2, χ2 = 98.4, p < .001, z = 5.9). There was no significant difference in the incidence of these charges before or after buprenorphine was initiated (13.6% versus 13.3%, Fisher’s exact test = .94), and in 1.7 percent of cases, charges happened both before and after buprenorphine began. The most frequently incurred disciplinary charges, with statistically significant differences, for the buprenorphine group were misuse of authorized medication (10.1%, df = 2, χ2 = 61.6, p < .001), use of prohibited substances (9.0%, df = 2, χ2 = 47.6, p < .001), possession of prohibited substances (8.5%, df = 2, χ2 = 24.2, p < .001), and refusing drug testing (2.3%, df = 2, χ2 = 17.7, p < .001). Analyzing these results further, there were more charges for use of prohibited substances before buprenorphine initiation (7.1% versus 1.9%, Fisher’s exact test < .001) and more charges for misuse of authorized medication after buprenorphine initiation (2.4% versus 7.7%, Fisher’s exact test < .001).

Substance-Related Institutional Chargesa, TCU-DS = Texas Christian University Drug Screen, OUD = Opioid Use Disorder; UD = Use Disorder, aAll Categories p < .001
Institutional Variables
For the prescription of a nonpreferred form of buprenorphine (see Table 4), the most common reasons given for buprenorphine (without naloxone) were liver enzyme abnormalities or liver disease, side effects from the buprenorphine-naloxone strips, and no reason cited. When an LAI form of buprenorphine was prescribed, a reason was cited only 51.4 percent of the time. In all but one case, LAI was used in anticipation of release to a halfway house program.
Reasons Stated for Prescribing Buprenorphine without Naloxone Component
Looking in more detail at individuals with OUD but not on buprenorphine, 16 (4.0%) had been prescribed it earlier in 2019. The reasons for discontinuation are shown in Table 5, with the most frequently identified reasons being side effects, a preference to not be on buprenorphine when released, and simple refusal. In only one case was misuse of buprenorphine cited as the reason for discontinuation.
Reasons for Discontinuing Buprenorphine
In a secondary analysis looking at inmates prescribed buprenorphine controlling for MHSNR status, the gender gap closed (2.1% versus 2.5% respectively were women, Fisher’s exact test = .82), but the racial disparity in prescribing buprenorphine persisted and was larger (White 73.1%, Black 14.4%, Hispanic 11.4%, Asian 0.2%, Other 0.7%). TCU-DS severity was identical (8.2) whether or not the inmate prescribed buprenorphine was on the MHSNR. Inmates prescribed buprenorphine and on the MHSNR were more likely to be on buprenorphine long term (i.e., ≥ 90 days, 70.3% versus 59.5%, Fisher’s exact test < .001) and were no more likely to have a substance-related disciplinary charge (27.4% versus 23.2%, Fisher’s exact test = .16).
In a secondary analysis of buprenorphine prescription by race (White n = 589, Black n = 149, Hispanic n = 122), there were no statistically significant differences in TCU-DS (White 8.3, Black 7.7, Hispanic 8.3, ANOVA p = .23), or time to release (White 2.2 years, Black 2.5 years, Hispanic 1.8 years, ANOVA p = .30). White inmates prescribed buprenorphine were more likely to have substance-related disciplinary charges (White 27.7%, Black 22.1%, Hispanic 17.2%, χ2 = 6.8, p < .05) and were more likely to be on the MHSNR (White 53.5%, Black 42.3%, Hispanic 40.2%, χ2 = 11.1, p < .01). There was a significant difference in days on buprenorphine by race (White 186.0 days, Hispanic 157.4 days, Black 159.0 days, ANOVA p = .04), but none of the post hoc comparisons reached statistical significance.
Discussion
The descriptive data for inmates prescribed buprenorphine in the NJDOC largely support fidelity of UCHC providers to our internal practice guideline for buprenorphine prescription. The vast majority (85.9%) of inmates are getting buprenorphine-naloxone strips, which is the preferred form according to our guideline. When prescribed the nonpreferred form of buprenorphine (without naloxone) tabs, half of the time, the reason cited was hepatic toxicity or liver disease, as suggested by the guideline. The remaining reasons given suggest a need for further scrutiny. The naloxone component of buprenorphine-naloxone strips is not absorbed when used as directed, so side effects from this component alone are unlikely.29 It is important to note that hepatitis is not an absolute contraindication for buprenorphine-naloxone, and the prescribing information for buprenorphine without naloxone carries similar warnings about hepatic risks.29,30 Laboratory monitoring for hepatotoxicity is appropriate regardless of the form of buprenorphine chosen. Hepatitis is a very common comorbidity in OUD. For example, the seroprevalence of Hepatitis C at a methadone clinic in New York City between 2013 and 2016 was 48.7 percent.31 It is possible that the UCHC guideline may have oversimplified hepatic risk as a reason for avoiding the buprenorphine-naloxone strips and that some inmate patients have learned this and used it to obtain a form that is more easily diverted.
The most frequently prescribed dose of buprenorphine was 8 mg, and 71.3 percent of inmates on sublingual buprenorphine were prescribed between 4 mg and 8 mg as recommended by the UCHC guideline. Underdosing was rare, though a substantial number of individuals (27.2%) were on higher than recommended doses. In a study of buprenorphine induction of prisoners, Vocci found that around week 8 the mean buprenorphine dose plateaued around 12.5 mg.(24) Unrelated to our project, an update to the UCHC practice guideline in December 2019 changed the recommended top dose to 12 mg per day and described it as a cap, barring exceptional circumstances. The rationale was that this is the maximum dose of buprenorphine-naloxone available in a single strip. Giving multiple strips either increases the risk of diversion (via stacking or hiding the additional strips) or substantially increases nursing administration time. We anticipate that the average daily dose of buprenorphine in our system will have risen since this update to the guideline.
Inmates on buprenorphine were more likely to be closer to release than those with an OUD but not prescribed buprenorphine. This is not surprising. The UCHC guideline suggests a lower threshold for prescribing to those anticipated to return to the community within 90 days, whereas it recommends collection of additional information (such as outside hospital records, collateral from outside informants, and institutional medical and disciplinary history) to support a conclusion that the benefits of long-term maintenance MOUD during incarceration outweigh the risks. The inmate experience of receiving buprenorphine during incarceration can be inconvenient and even risky. It is time-consuming, stigmatizing, may put inmates in danger of extortion or intimidation by peers, and exposes the inmate to closer observation by custody and health care staff.
Inmates on buprenorphine were more likely to receive a substance-related disciplinary charge than inmates with OUD but not prescribed buprenorphine or those without a diagnosis of OUD. Incidence of charges was similar both before and after buprenorphine was prescribed. While the before and after periods vary depending on what point in the year the buprenorphine was initiated, the risks of incurring a disciplinary charge also changed. Inmates on buprenorphine were less likely to be charged for using illicit substances, though they were also under greater observation during medication administration and were more likely to be charged with misuse of medication.
Demographic data indicate that the typical NJDOC inmate on buprenorphine is a White male in his late 30s. Compared with persons diagnosed with OUD but not prescribed buprenorphine, the numbers of women, Black, and Latino inmates are underrepresented. The clinical significance of the observed gender difference will require further research as the number of female inmates in the NJDOC is small. (As of January 1, 2020, 3.0% of the inmate population was female).21 The racial differences, especially for Black inmates, are more pronounced. According to publicly available information, as of January 1, 2020, NJDOC inmates were 62 percent Black, 22 percent White, 16 percent Hispanic, and 1 percent Asian.32 These numbers most closely resemble the demographic breakdown of our sample that were not diagnosed with OUD. For inmates prescribed buprenorphine, there were nearly four times as many White inmates as Black inmates, while nearly twice as many Black inmates as White inmates had a diagnosis of OUD but were not prescribed buprenorphine. This replicates Lagisetty’s observations that Black persons in the community were only 23 percent as likely as White persons to be prescribed buprenorphine.33
There are several possible explanations for the observed racial differences in buprenorphine prescribing. OUD is more common in White persons, especially in those 20 to 40 years of age, which is consistent with the typical age of an incarcerated adult.34 Our methodology controlled for this, however, by looking at prescription of buprenorphine by diagnosis. In 2020, SAMHSA published a document specifically addressing the disparity in OUD treatment for African Americans. Relevant cultural factors may include a historical distrust of health care and the justice system, longstanding stigmatization of Black people with SUD, and a perception in some Black communities that SUDs are weaknesses rather than being diseases.35 White inmates prescribed buprenorphine were more likely to be on the MHSNR and to have disciplinary charges. Both of these factors could have resulted in increased clinical contacts with either buprenorphine prescribers or referral sources. Other considerations include social determinants such as limited options for buprenorphine aftercare in urban settings and fewer Black providers with DATA 2000 waivers, which may have discouraged Black inmates from pursuing MOUD.36
Our secondary analysis controlling for MHSNR status suggested that the disparity in prescribing for Black inmates was larger for those in mental health treatment. We suspect that a greater willingness of psychiatric providers to prescribe buprenorphine, and to prescribe it long term, drove this observation. While there appears to be an even distribution between psychiatric and general medical prescribing of buprenorphine, the usual proportion of inmates on the MHSNR is relatively small. For example, only 16.1 percent of those without a diagnosis of OUD were on the MHSNR, and this is closer to the overall percentage we have typically observed. Though our statistical analysis suggested that other interpretations are possible, White inmates were on buprenorphine for longer periods than Black or Hispanic inmates, despite no significant difference in their anticipated time to release. While it is possible that Black and Hispanic inmates are more inclined to wait until they are prerelease to request MOUD, implicit bias cannot be excluded.
We intend to address the racial differences observed in this study by presenting our performance improvement project and results to all qualified buprenorphine prescribers in both the psychiatric and medical departments of UCHC. Another option is to provide public service-type information to inmates addressing cultural concerns and encouraging those with an appropriate clinical indication to seek help. An unrelated continuous quality improvement method used by UCHC that began in mid-2019 is a centrally generated biweekly report of inmates who have expressed an interest in MOUD at any point during their incarceration and are approaching release to the community within six months. This report does not include data about race. It is sent to all prescribers with encouragement to meet with these individuals and discuss MAT options. Research is needed to evaluate the effect of such interactions.
There are several limitations to this study, including all those inherent to a retrospective chart review (such as missing data, incorrectly documented information, or the risk of incorrect data abstraction). Our results may not generalize to other correctional systems, especially those operating under different policies and procedures, with different medication availabilities, or with differently qualified staff. The diagnoses found in the EMR were made clinically, usually but not always with the assistance of a psychometric instrument (the TCU-DS). Inmates who entered the NJDOC before the TCU-DS was in wide use by UCHC, for example, may have been given a SUD diagnosis without the benefit of a psychometric instrument. TCU-DS scores were missing in 10.6 percent of the inmates prescribed buprenorphine, 18.4 percent of those with OUD but not on buprenorphine, and 34.3 percent of those without a diagnosis of OUD. This is unsurprising as inmates prescribed buprenorphine were actively in treatment for a substance use disorder. Disciplinary charges for misuse of authorized medication do not specify what medication was misused in either the EMR or iTAG. Therefore, it cannot be assumed that the misused medication was buprenorphine. Other factors we did not include in this review, like a substance-related instant offense or prescription monitoring program data, might have influenced prescribing decisions. We did not use a power analysis to determine the sample sizes of our comparison groups, so the study may not have been powered to detect some differences (like younger age in inmates with OUD, which did not reach statistical significance). This was an exploratory study with reasonable sample sizes that could inform more targeted research in the future with specific hypotheses and associated power calculations. An alternative study design using a sampling of inmates by race, and then calculating the rate of OUD diagnosis and treatment with buprenorphine, would more directly have assessed our practice in terms of underdiagnosing or undertreating OUD by race. But this was not the intention of our project; it is an empiric question that may be addressed by other research.
In summary, we found that 875 inmates in the NJDOC were receiving prescribed buprenorphine at the end of 2019. Consistent with UCHC’s internal practice guideline, inmates prescribed buprenorphine were most likely receiving buprenorphine-naloxone strips at doses ranging from 4 mg to 8 mg daily, though we anticipate dosing to trend higher. Inmates on buprenorphine were more likely to be closer to release, and more likely to incur disciplinary charges related to substances even though they were being prescribed buprenorphine. We observed differences in prescribing patterns related to gender and race, especially for Black inmates, who were more likely to have a diagnosis of OUD but not be prescribed buprenorphine. Similar observations of underprescribing MOUD have been made in community samples. The controlled environment of the NJDOC is an opportunity to offer and study interventions to address such disparities.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2022 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}
{kind=link}
{kind=link}