


Abstract
The current pandemic raises substantive ethical and legal challenges for inpatient psychiatric units striving simultaneously to contain COVID-19 and provide safe, high-quality psychiatric care. Among these challenges, psychiatric units need to consider their role in isolating and quarantining COVID-19 positive patients who are psychiatrically cleared for discharge. We examine this complex dilemma by evaluating mental health law, quarantine law, public health ethics, a case from an urban academic medical center’s inpatient unit, and literature focused on treatment and isolation protocols during HIV and tuberculosis epidemics. Although inpatient units are highly restrictive and intended for acute psychiatric treatment, at present there are no obvious isolation, quarantine, or housing options for many patients with mental illness infected with COVID-19.
The far-reaching effects of COVID-19 continue to pose logistical, medical, and ethics questions for the health care system. Psychiatry departments confront a unique set of challenges navigating the ethics tensions related to psychiatric treatment during the pandemic. The guiding moral principles of autonomy, beneficence versus nonmaleficence, utility, privacy, transparency, maintaining trust, and justice (including fair distribution of scarce resources (distributive justice), respect for people's rights (rights-based justice) and respect for morally acceptable laws (legal justice)) provide a framework to grapple with new questions.1 A major concern that inpatient psychiatric units continue to encounter is how best to contain COVID-19 and decrease exposure risk while continuing to provide urgently needed access to expert inpatient care. In response to these challenges, some inpatient psychiatric units have developed designated COVID-19 positive or COVID-19 negative units.2 This designation allows hospitals to safely continue both voluntary and involuntary psychiatric admissions while protecting patients from infection without requiring more restrictive measures, such as strict isolation, seclusion, or physical restraint, to segregate infected from noninfected individuals.2 Another question arising during the pandemic is the role, if any, of the psychiatric inpatient unit in isolating infected individuals with serious mental illness from others in the community. This article explores the ethics and legal responsibilities and limits of psychiatric units in serving as isolation sites for COVID-19 infected patients who may otherwise have been psychiatrically cleared for discharge but require new or continued isolation or quarantine.
Mental Health Law
We begin with some of the original court cases that pertain to inpatient psychiatric admission and discharge. Wyatt v. Stickney3 (1971), initiated by guardians of patients admitted to Alabama State Mental Hospital, established that inpatient psychiatric units are justified in keeping a patient only while they provide treatment.3 The case clearly states that patients cannot be held for custodial care, as hospitals are not a penitentiary to house people indefinitely.3 Another landmark case, O’Connor v. Donaldson4 (1975), adds that hospitals cannot detain patients simply to give them a higher quality of living compared with what is available to them in the community.4 The court ruled that “commitment must be justified on the basis of a legitimate state interest” (Ref. 4, p 580) and established that hospitals cannot restrict patients if they can live safely on their own or with family.4
An additional case during the pandemic is also relevant. In Foster v. Commissioner of Correction5 (2020), the Supreme Judicial Court of Massachusetts ruled that substance use treatment facilities need to provide individuals who are civilly committed for treatment with a new hearing to calculate the risk and benefits of admission during the pandemic.5 Part of the ruling argues that civil commitment for substance abuse treatment during the COVID-19 pandemic does not sufficiently advance treatment goals, thereby violating individual’s substantive due process rights.5 Although this case relates to substance use treatment and not specifically to an inpatient psychiatric unit, it is an example of how states have contemplated the risks and benefits of inpatient treatment. The ruling suggests that infection control measures in inpatient settings, such as no longer offering groups or milieu treatment, may degrade the ability of a program to offer the same level of care that would otherwise be expected.
While establishing important precedents, these rulings do not definitively address the question of how to proceed if a COVID-19 positive or exposed patient no longer experiences psychiatric symptoms warranting inpatient level of care, yet their shelter, family, or residence will not accept them back due to concern about contagion or inability to allow the space or support needed to isolate or quarantine from others. The addition of COVID-19 illness or exposure to our standard equation of evaluating readiness for discharge adds a new element in defining whether a person can live safely on their own or with family. Patients who would otherwise be considered safe for discharge may have ongoing psychiatric symptoms. If these symptoms interfere with their ability to understand or follow isolation or quarantine recommendations, that may shift the decisional balance toward the patient’s no longer being able to live safely in the community. In these cases, treatment is more obviously active and would aim to target these symptoms until the patient can be determined to be safe. In cases where patients’ symptoms do not significantly interfere with their ability to understand or adhere to isolation or quarantine, it becomes more complicated. The patient still may not have a safe place to go in which to isolate or quarantine, and though continued inpatient care involves ongoing active treatment regardless of patient level of symptomatology, one could argue that the level of treatment available while a patient is under strict isolation for COVID-19 is likely less than that offered to other inpatients who are not under isolation. Hence, there is a distinction between those patients who remain psychiatrically symptomatic and are a danger to themselves or others because of their inability to understand isolation rules, but otherwise are safe for discharge under non-COVID-19 circumstances, and those patients who no longer have psychiatric symptoms and remain a danger simply because they have no safe place to isolate.
In New York City (NYC), one solution to the safe disposition problem came from underutilized hotels that were repurposed as COVID-19 hotels to allow homeless individuals with COVID-19 to complete the quarantine period rather than returning to shelters.6 The criteria for this temporary housing were strict and the resource was scarce and often unavailable.6 The NYC Department of Homeless Services issued a COVID-19 hospital referral application for isolation sites, however serious mental illness or history of suicide ideation or attempt were considered criteria for exclusion.6 These limitations essentially meant that people with serious mental illness could not go to shelters as the shelter system did not want to take on additional liability or responsibility in their already burdened system.
Quarantine Law
The court cases cited above relate to mental hygiene laws rather than quarantine laws.3,–,5 In a recent article,7 Eric Broutman, J.D. explained that many of the theories used in public health law are drawn from mental hygiene law. Both restrict individual liberties based on something that may happen in the future to protect the rights and safety of the community.7 Just as with mental hygiene law, in which risk of harm to self or others must be proven for involuntary admission, quarantine law stipulates that the government must prove that the individual poses a danger to others via contagion to invoke involuntary quarantine.7 The standard of proof to quarantine an individual would be the same used to involuntarily commit a psychiatric patient, which is clear and convincing evidence.8,9 Once such danger is proven, federal law permits the government to quarantine individuals in two circumstances: an infected individual can be prevented from entering the country or from crossing state lines.7 Although there are federal laws that allow for the quarantine of individuals, they relate mostly to circumstances involving international, or interstate travel.10,11 The bulk of quarantine law emanates from individual states exercising their police powers and parens patriae powers.12
Police powers of states may be used by public health officials to compel treatment, direct or prohibit certain behaviors, or detain or isolate individuals based on the legal principle of salus publica (preventing or avoiding public harm).12 An early example of state police powers being used to quarantine comes from soon after the end of the Revolutionary War when Philadelphia was isolated to control the spread of yellow fever.12 During the 1950s and 1960s, state police power (and by extension orders of quarantine) became much more heavily scrutinized and restricted by the Supreme Court in favor of preserving individual rights and freedoms.12 Each state has public health laws that provide for the control of communicable diseases. In New York State, Article 21 of the Public Health Law lays out the powers and duties of local boards of health and health officers in controlling communicable diseases, which include: medical inspection and regulation of people infected with or exposed to diseases; provision of care and isolation for people with communicable disease in a safe environment to protect the public; and prevention of all interactions with infected places and people, including provision for purification and cleansing if necessary.13
On March 3, 2020, the Westchester County Health Commissioner used this power when she ordered the closure of Young Israel of New Rochelle synagogue and the self-quarantine until at least March 8 for congregants of the synagogue who attended services or events on February 22 and 23, 2020. The Health Commissioner warned that those who did not self-quarantine would be mandated to do so by the County Department of Health.14 In New York, the state Public Health Law goes further in Section 2120 to provide the option for a physician to notify a health officer when a person afflicted with a communicable disease is unable or unwilling to prevent danger of infection to family or other contacts.15 The health officer then investigates the situation and can refer the situation to a magistrate who may then commit the individual to any hospital or institution established for the care of people suffering from such a communicable disease on the basis of danger to others.15
Interestingly, New York City has its own set of guidelines given the city’s density. An appointed commissioner in New York City is authorized to detain suspected infectious individuals for up to 60 days without a court order in a hospital or their home; however, individuals have a right to a hearing.7 A notable example of a federal quarantine order occurred in 2007 when the Centers for Disease Control (CDC) required an individual, Andrew Speaker, to be quarantined in a New York City hospital based on suspected drug-resistant tuberculosis.16
The distinction between isolation and quarantine is important. Quarantine pertains to containing individuals who have had exposure and are deemed to be potentially contagious, while isolation applies to individuals with known infections.16 Although distinct, both quarantine and isolation procedures are often influenced by religious, political, and economic biases.16
Precedents from Other Epidemics
The literature regarding notable infectious disease epidemics, such as with human immunodeficiency virus (HIV) and tuberculosis (TB), provides a framework for how to grapple with the ethics strains of discharging psychiatric patients during uncertain times. In the 1980s, physicians who discharged HIV positive patients were conscious of the potential harm patients could inflict on others, the discrimination they would experience, as well as the lack of housing options for them.17 At that time, experts concluded that state hospitals should not serve as penitentiaries for competent and stable HIV positive patients, even if they have the potential to spread the virus.17 One could infer from this logic that inpatient psychiatric units should not be used as isolation centers, even during infectious disease outbreaks, and, by extension, difficulty with disposition placement may not be enough to justify an extended stay on a psychiatric unit.
In contrast to guidance provided during the HIV epidemic, however, select literature related to tuberculosis offers a more cautious route with more lenience toward holding patients while implementing safeguards to promote containment in vulnerable populations. Specifically, an emphasis is placed on the necessity of comprehensive discharge planning to maintain tuberculosis treatment compliance during management of outbreaks. Bayer et al. posit that effective discharge planning includes securing a residence with a range of accessible social services and treatment options.18 They argue that governments are ethically responsible to deliver such resources to facilitate treatment, especially when treatment is obligated.18 Of note, in the 1990s a select number of nonadherent tuberculosis patients in a direct observed therapy clinic in Denver, Colorado, were sent to locked units to receive treatment to protect public health.19 Of the 20 patients detained, 18 had alcohol use disorder and two had untreated schizophrenia.19 Despite comprehensive outpatient treatment, Colorado allowed for even more restrictive measures to contain a tuberculosis outbreak.
Although HIV and TB are both devastating illnesses with high morbidity and mortality, the difference between these two approaches is likely rooted in the difference in transmissibility between the two illnesses. The much higher rate of community TB transmission as an airborne pathogen leads to a more restrictive response and is a better analogy for the current SARS-CoV-2 pandemic. The examples from HIV and TB lead us to conclude that it is the responsibility of the provider, as well as the state, to ensure that patients receive comprehensive treatment resources and safe discharge plans, including provisions to protect public health, and that the level of infringement on patient rights warranted is likely proportional to the level of transmissibility, morbidity, and mortality of the infectious illness.
Ethics and Professional Considerations
Ethics concerns about safe discharge planning existed before COVID-19, however the pandemic has highlighted the intensity of these decisions. Hospitals need to calculate the overall benefit and risk of admission for patients during a pandemic. Inpatient psychiatric hospitalization could create a potential exposure for patients as they are in closer contact with others than they may otherwise be in the community, and often in contact with others who may have severe psychiatric symptoms which preclude their ability to comply with social distancing, mask-wearing, or even basic hygiene. In addition, given that much of the therapeutic milieu, such as groups and visiting, have been paused or modified significantly, patients may not receive the accepted level of care that was provided before the pandemic. Sorrentino et al. argue that without the full support of the multidisciplinary team, discharges may be further delayed during COVID-19, as there are fewer personnel evaluating patient progress and fewer therapeutic interventions available.20 The advantage of admission is further weighed against patient autonomy, beneficence, nonmaleficence, and responsibility to the community.20
Ghossoub and Newman explore the responsibility psychiatrists must consider when determining the safety of third parties who may contract the infection from patients.21 Patients with serious mental illness may have poor insight or judgment about their COVID-19 status that may magnify their risk of transmission.20 Psychiatrists need to use clinical judgment and legal consultations to calculate their duties to their patients and communities.21 The American Psychiatric Association (APA) ethics committee has specified that caregiver safety is an important consideration in discharge planning.22 They cite principles including fidelity, nonmaleficence, and proper distribution of scarce resources in their reasoning and posit that discharging infectious patients to the street poses a safety risk both to the patient and the community. The APA ethics committee stated that, in the event of a public health emergency, involuntary patients can be quarantined if the process carefully discerns between seclusion for behavioral reasons and infectious ones. They defend this statement based on protection or preservation of self and the community. In June 2020, the APA Board of Trustees published guidance on admitting and discharging psychiatric patients during communicable disease outbreaks and explicitly warned against premature discharge as it can result in adverse outcomes for patients and the community.23 They emphasized the need to address patients’ mental health needs while also considering the potential risks of the communicable disease at different levels of care and stated that delivery of safe and appropriate treatment at all levels includes adequate protection from infection.23 Although the statement does not specify COVID-19 infection status, the overall tone favors inpatient admission as long as safety measures and potential risks are considered.
In addition to the potential risks outlined above, there is a risk of financial harm to patients by holding them longer in the hospital. With respect to hospital billing, it would be untenable for patients to bear the cost; rather, we anticipate that coverage would be discussed with third payers as usual. As an example, in March 2020, MassHealth issued a statement that acute inpatient hospitals could bill MassHealth for patients no longer requiring an inpatient level of care but who require quarantine in the hospital or who cannot be safely discharged due to COVID-19 status.24 In instances when insurers are unwilling to cover the costs, medical centers may elect to absorb the costs as they do in other circumstances. Another potential financial harm is related to impeding a patient’s return to gainful employment; however, this impact may be negligible compared with the person’s psychiatric illness and COVID-19 infection or exposure.
Case Scenario
To further explore these ethics questions, we present here a common scenario from an inpatient psychiatry unit in New York City during the initial COVID-19 peak in the United States. John Doe is a middle-aged man with a history of schizophrenia who resides with his family, some of whom are elderly. Mr. Doe presented to the hospital with worsening symptoms, including aggression and violence in the context of medication nonadherence. During a prolonged hospitalization, he was eventually transitioned to clozapine for treatment-resistant psychosis with gradual improvement. With reduction in symptoms and greater ability to care for himself, he was determined to be psychiatrically stable and no longer to pose a danger to himself or others.
As his treatment team worked on disposition plans, including helping his family feel safe with him returning home, he tested positive for COVID-19, although he remained asymptomatic. His family were concerned about having him return home to self-isolate given the risk of transmission.
At this point in Spring 2020, COVID-19 rates were surging toward their peak in New York City, fear was overwhelming and, despite guidance from the CDC about self-isolation, housing options and shelters were cautious and did not yet have clear policies on accepting people who had tested positive. In view of Mr. Doe’s new COVID-19 positive status, the New York City centralized shelter system predicted it would take weeks to find him a bed.
Mr. Doe was being held on an inpatient psychiatric unit involuntarily and had been determined to no longer meet criteria for that legal status based on improvement in his psychiatric condition prior to testing positive for COVID-19. He requested to be discharged. The team now had to reconsider his capacity within this new circumstance, and Mr. Doe had a tenuous grasp of his COVID-19 diagnosis and its multiple implications.
As we consider this case in an ethics framework, we consider our obligations to Mr. Doe. We have a duty to honor his autonomy by treating him in the least restrictive setting. There is a fine balance between protecting public health and maintaining individual privacy and liberty. Childress et al. offer five justifications for overriding individual liberty to promote public health policies, which include the anticipated effectiveness of policies that breach moral the guidelines, the proportionality or balance of potential benefits versus risks, the necessity of the policy to achieve public health measures, minimized infringement on moral considerations, and public justification to relevant parties.1
If we were to honor Mr. Doe’s desire to be discharged without a safe disposition, he would likely either return to his family’s home, possibly endangering them by exposing them to COVID-19, or end up on the street where he would be unlikely or unable to self-isolate and thereby potentially spread the virus to others. Based on the precedent from O’Connor v. Donaldson4, he could not be held in the hospital for custodial care if he was in fact no longer receiving acute inpatient level of treatment, and the hospital and state would thus have a responsibility to provide for housing or respite.4 As an alternative to this, quarantine law in NYC would allow the commissioner to detain him in the hospital to serve out his quarantine period.7,16
Mr. Doe’s case highlights the rigid requirements for discharge despite alternatives which are entirely unsatisfactory and potentially dangerous. Arguably, Mr. Doe was still a danger to others given his unknown contagion status. Furthermore, he might even be considered a danger to himself because if he were to infect his own family he could theoretically disable his support system and be left unable to care for himself. Accordingly, an important question to ask in these situations is whether the danger the patient presents is an outgrowth of his mental illness or purely based upon his positive COVID-19 status. Under the former, the patient may remain hospitalized under current mental health laws, the latter would require the utilization of quarantine laws.
Ultimately, Mr. Doe agreed to work with the treatment team to find a safe disposition plan but declined to convert to voluntary legal status. He continued to be treated on the inpatient psychiatric unit, which out of necessity at the time became a designated COVID-19 positive psychiatric unit within a medical hospital system that was overwhelmed with patients with COVID-19.2 His team continued to target his impulsivity, self-care ability, insight, and judgment, which were all felt to be affected directly by his psychiatric symptoms related to his diagnosis of schizophrenia. Shelter housing continued to be unavailable. Regular contact was maintained with Mr. Doe’s family via phone as he completed the recommended COVID-19 isolation period. With much encouragement, support, education and further family therapy interventions, family members were able to feel safer accepting Mr. Doe back, leading to his much anticipated and long-overdue discharge.
Discussion
Inpatient psychiatric units have the capacity to offer life-saving treatment but also have the potential to infringe on patients’ rights in a way that can be traumatizing and detrimental to trust in our medical system and psychiatric care. While patients should not be held on an inpatient psychiatric unit solely for isolation or quarantine of an infectious disease, there may be times when, because of ongoing psychiatric symptoms or disposition challenges, there may be no other option for safe discharge. Inpatient units and inpatient psychiatrists must balance the myriad ethics and legal obligations involved to determine if and when to isolate or quarantine civilly committed psychiatric patients with new or ongoing COVID-19 illness or exposure who would otherwise have been considered safe for discharge.
The available guidance can be summarized in the following points: mental hygiene legal precedents suggest that continued civil commitment requires providing active treatment, and must be based on legitimate state interest in that patients cannot live safely elsewhere under a lower level of care, and that patients have a right to a hearing to reevaluate the risks and benefits of the inpatient level of care to account for both changes in the care provided and potential additional risks during the pandemic;3,–,5 quarantine legal precedents suggest that the level of restriction of patients’ rights and enforcement of isolation or quarantine should be proportional to the likelihood of transmission, morbidity and mortality of infection, and extent of the public health crisis in the community, including that strict enforcement may be warranted in some instances when the risk to the public is severe;7,12,13,15 and as physicians we have a duty to our patients to protect them in an inpatient setting when they pose a danger to themselves or others or are gravely disabled by their symptoms, to provide a collaborative therapeutic treatment environment in the least restrictive setting, while also managing our duty to protect the families, communities, and systems that support our patients.1,20,–,22 Based on these legal and ethics considerations, and accounting for the fact that COVID-19 is a contagious respiratory illness with significant morbidity and mortality, but a relatively short contagion period compared with prior examples of HIV and TB, it may be necessary to enforce the isolation or quarantine period for certain psychiatric patients who would otherwise be considered stable for discharge.25,26 In this situation, one must also consider state licensing and regulatory frameworks that may restrict the treatment, isolation, or quarantine of a patient on a psychiatric unit. For example, in New York, a psychiatric facility or unit of a general hospital may not provide care to a patient where the primary purpose for the admission is not for psychiatric reasons.27 The burden of balancing this complicated risk/benefit analysis and finding the least restrictive treatment setting falls on the inpatient psychiatrist, the inpatient psychiatric unit, and the hospital system working in collaboration.
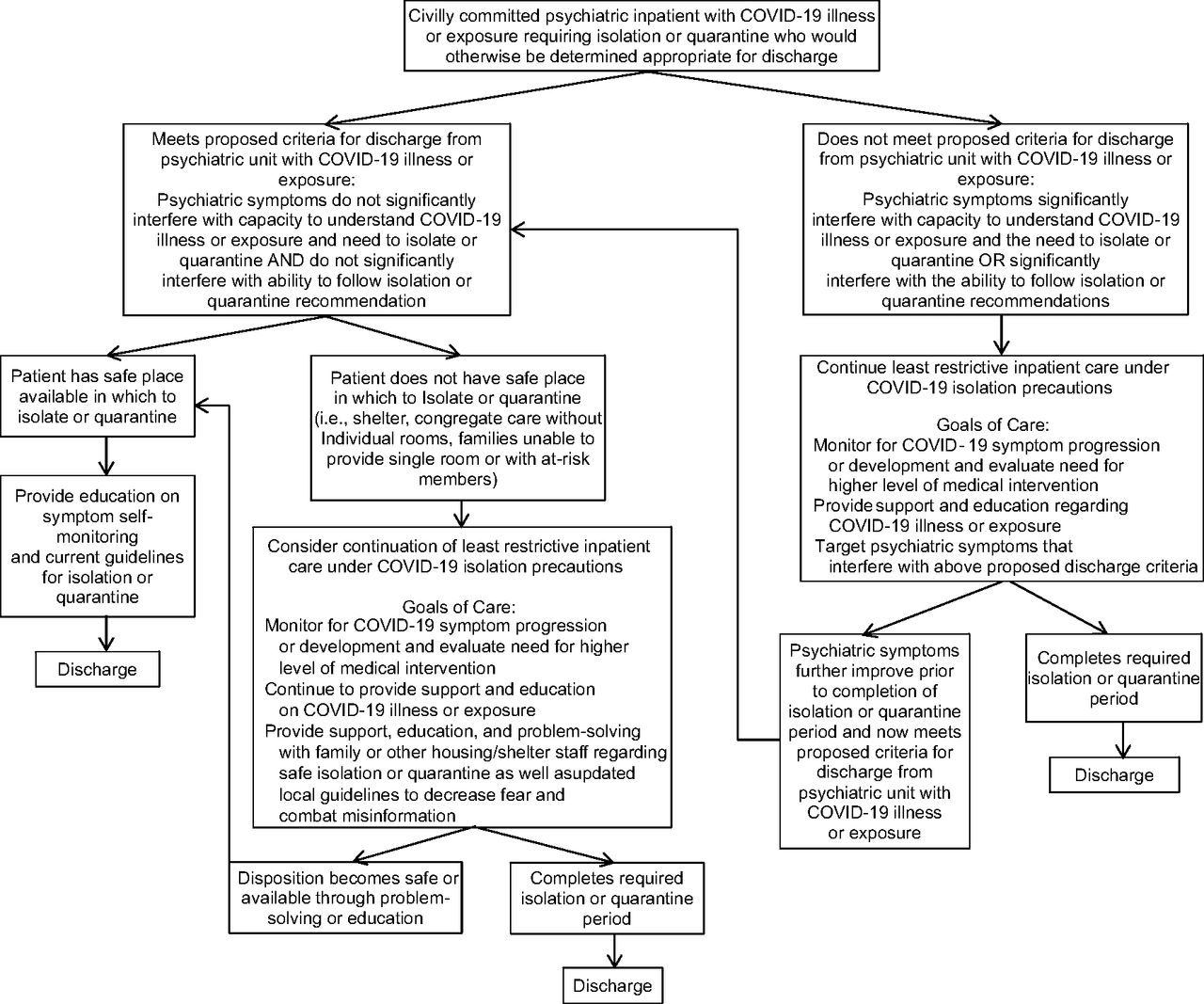
Based on our significant experience on an inpatient psychiatric unit that has at times been a COVID-19 positive psychiatric unit or under quarantine for outbreaks of or exposures to COVID-19, we suggest an algorithm and guidance for managing this complex scenario in Figure 1. The psychiatrist must first modify the determination of whether patients are safe to live alone or with family in the community to include consideration of whether patients have ongoing psychiatric symptoms that significantly interfere with either their capacity to understand that they have COVID-19 or have been exposed to SARS-CoV-2 and need to isolate or quarantine or their ability to follow isolation or quarantine procedures. The distinction here that ongoing psychiatric symptoms are what interfere with this ability and capacity is important. There are certainly individuals in the community who may not agree with isolation or quarantine or who may not have the ability to follow these guidelines, and this by itself should not be the basis of keeping someone in the hospital. But if the psychiatric symptoms for which the patient was hospitalized are the limiting factors that interfere with the ability to understand or follow isolation or quarantine, then it is reasonable to suggest that further treatment via inpatient hospitalization could target these symptoms and mitigate the risk that the patient poses to families or communities via infection.
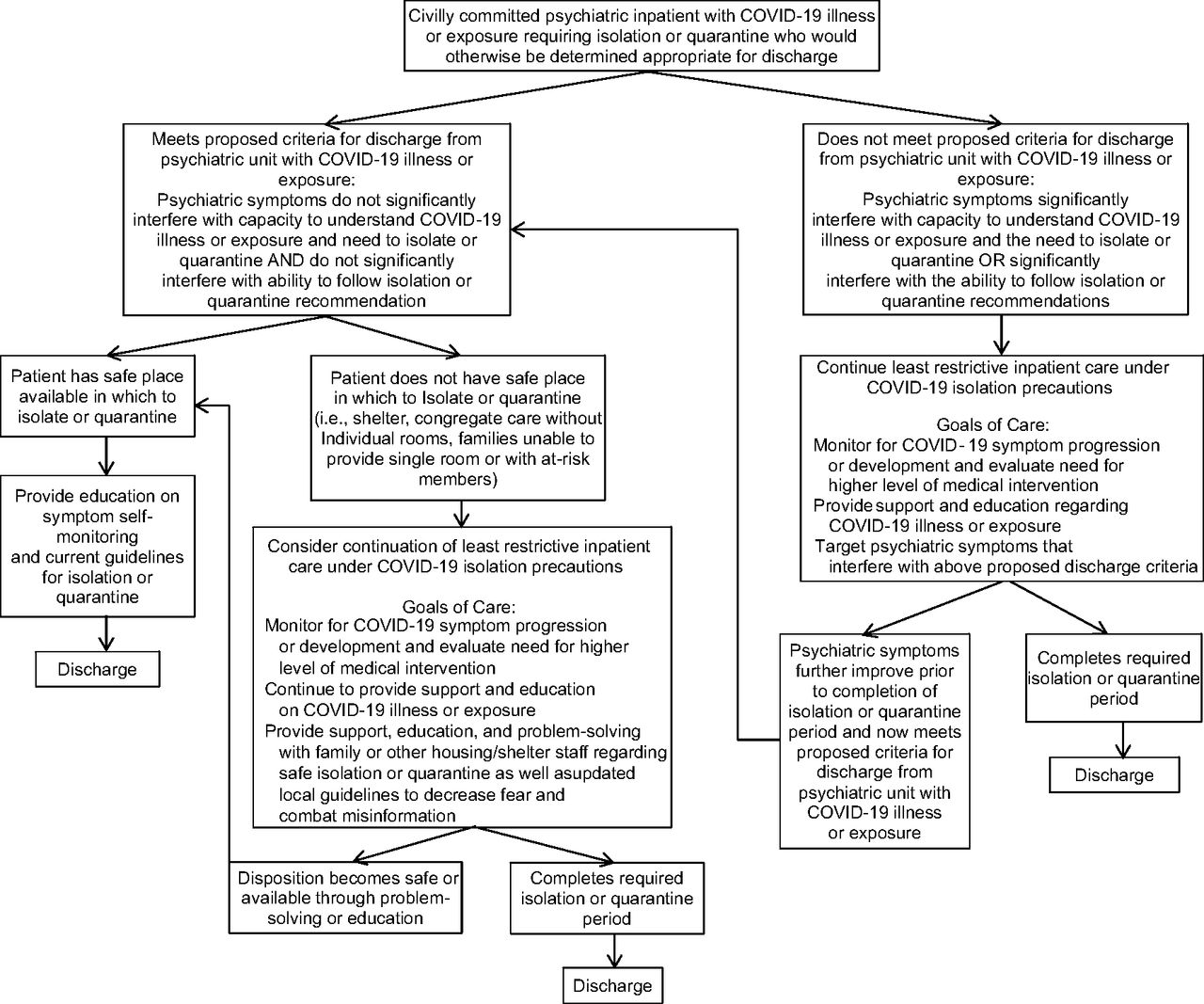
Algorithm for ethical and safe psychiatric discharge for COVID-19 positive or exposed patients.
Once a patient is then determined to be safe to live alone or with family in the community and no longer has psychiatric symptoms that interfere with understanding or cooperating with COVID-19 isolation or quarantine recommendations, the patient will still require a safe place in which to self-isolate or quarantine. An acute inpatient psychiatric unit is the most restrictive treatment environment and is not an ideal place to quarantine or isolate a patient, due to strict safety protocols, limited resources, and a milieu that is specifically designed to promote patients being out of their room and interacting with others as an important element of treatment. Despite this, there are a few other options to consider for alternate levels of inpatient care that should be evaluated when psychiatric symptoms are no longer interfering with a patient’s ability to isolate or quarantine and there is no other safe place to support the patient in doing so. These options, shown in Table 1, include transferring the patient to a general medical unit bed (no longer under civil commitment), transferring to a designated COVID-19 positive psychiatric bed (if under isolation rather than quarantine), or decreasing restrictions on psychiatric patients on a typical inpatient unit who require strict isolation or quarantine. Cases that fall in this category should be discussed with hospital leadership, infection control and infectious disease consult teams, complex case consult teams, medical ethics teams, risk management, and hospital legal teams. One solution that has been posed internationally comes from China where psychiatric hospitals created isolation wards specifically for psychiatric patients with suspected and confirmed COVID-19; however, concern was raised that these wards had the potential to increase hospital-acquired infection without proper infection control.28 Psychiatric hospitals in China also considered building designated quarantine facilities for clinically stable psychiatric patients with mild to moderate symptoms of COVID-19 infection.28 Hospital systems, cities, and states should consider similar creative and resourceful alternatives for isolation.
Potential Options for Least Restrictive Inpatient Care while under COVID-19 Isolation Precautions
If continuing inpatient treatment is the only option, every effort should be made to work with the patient to collaborate on a plan, including discussing the option to convert to voluntary legal status and the patient’s legal right to request discharge if the patient is not in agreement with the care provided. Bringing the case to court may help decrease the burden on the psychiatrist and adds the support of a judge with legal expertise to contribute to the decision of whether continued inpatient level of care is warranted under civil commitment. Throughout this process, it is necessary to continue to educate and advocate for patients to have a safe place to go by having regular communication and interaction with family, residential staff, shelter staff, and case workers to disseminate current medical information and improve caregiver understanding and ability to support the patient through an isolation or quarantine period.
Safe discharge planning was frequently challenging before the COVID-19 pandemic given a lack of supportive housing options for psychiatric patients and often a paucity of family or other social supports, but has become even more so now with additional restrictions on congregate care, the need for social distancing, and often others’ competing interests of wanting to protect themselves and limit exposure. As the health care system continues to navigate this new era it is imperative to support public policy to create safe and sustainable temporary housing for our most vulnerable and needy population of patients with serious mental illness.
Acknowledgment
The authors would like to thank Dr. Tia P. Powell at The Montefiore- Einstein Center for Bioethics for her guidance and support in discussing ethical conflicts related to COVID-19 and inpatient psychiatry, as well as her encouragement in pursuing this manuscript.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2022 American Academy of Psychiatry and the Law





{kind=link}