


Abstract
This study aimed to provide a descriptive analysis of the geriatric forensic population referred to a Regional Forensic Psychiatric Service by the court for evaluation (as inpatient, outpatient, or while incarcerated) in New Zealand, over a 7-year period. Data were collected retrospectively from forensic hospital records, including court-ordered reports for those aged 60 and older. Two-fifths (42%) of the 97 referred study subjects were diagnosed with some form of cognitive impairment such as dementia. The majority had a prior history of offending. Two-fifths (39%) were facing sexual charges, and one-third (33%) violent charges. Over one-quarter (28%) of the elderly sample was found unfit (incompetent) to stand trial. A better understanding of this group is needed to ensure forensic assessments and health and social services meet their various psychiatric needs.
As the population ages, the number and proportion of older age offenders has also increased. In New Zealand, the elderly prison population is increasing, with 6.2 percent of the prison population being over age 60 as of September 2020.1 Because forensic evaluations and clinical services have traditionally been focused on younger populations, this demographic change signals a growing need to better understand clinical and legal concerns in older age offenders.
Previous international studies, although limited in number, have found that in comparison to younger offenders, those elderly defendants referred for forensic evaluations are more likely to lack trial capacity than younger defendants. This is frequently a consequence of dementia,2,3 with lower rates of schizophrenia and personality disorder in this population than in younger samples.3,4 They are also more likely to be charged with sexual offending than younger age groups.4 While the elderly currently make up a small proportion of offenders overall, they require unique assessment, diagnostic, treatment, and placement considerations.2,–,8
The present study is intended to add to the literature by describing the characteristics of forensic evaluees over the age of 60 in New Zealand, including their demographics, psychiatric and physical health, and interaction with judicial and psychiatric services. Based on the literature and our clinical experience, we hypothesized that this group would have frequent cognitive impairment which may compromise their competency to stand trial, a higher proportion of alleged sexual offending than seen in younger offenders, more medical problems, and fewer cases with a history of mental illness. In those with cognitive impairments, we were interested in the temporal associations between the cognitive impairment and any sexual alleged offending, and specifically whether charges were for historical or more recent sexual offending.
Methods
Sample
In New Zealand, courts may order forensic psychiatric assessments to assist determinations of capacity to stand trial, insanity, disposition, and assessment of risk. In Auckland, New Zealand’s most populous city, the public forensic psychiatric service is the Auckland Regional Forensic Psychiatry Services. The catchment area comprises a population of 1.8 million people. From 2009 to 2017, 2.6 percent of criminal defendants charged and convicted in New Zealand were over age 60, increasing from 1.95 percent to 2.95 percent over the course of the study.9 The current study included all 97 defendants over the age of 60 referred to the Auckland Regional Forensic Psychiatry Service between February 2009 and November 2016. Defendants in the Service are evaluated while incarcerated pretrial, on bail in the community, or as inpatients.
Study Design
Data were collected retrospectively from forensic documents and reports; variables collected are described in Table 1. Items reviewed included medical records, police reports, criminal histories, and psychiatric and psychological reports.
Data Collected
Charges were classified as violent if they involved use of physical force or a weapon against another individual. The following charges were classified as sexual: rape or attempts to rape, abduction for sex, indecent assault, unlawful sexual connection, indecent act (including indecent act with intent to assault), induce indecent act, incest, sexual connection with a young person, and attempted or committed sodomy. For those facing multiple charges, the classification was considered violent or sexual if they had at least one such charge.
We classified offending as “historical” if it was alleged to have occurred more than 10 years prior to the most recent psychiatric evaluation reviewed in the study, and otherwise as “recent” offending. This cutoff was chosen because survival for most forms of progressive dementia is less than 10 years.18 It would therefore be unlikely that dementia was a contributory factor in any such “historical” offending.
The New Zealand Mental Health Act 199216 dictates the legal definition of a mental disorder, akin to the civil commitment criteria in the United States. New Zealand’s Protection of Personal and Property Rights Act 198817 is the guardianship legislation which describes the process for the appointment of proxy decision-makers for people who have lost decision-making capacity and establishes Enduring (durable) Powers of Attorney (EPOA).
Impairment in Activities of Daily Living (ADLs) was determined using information in the forensic reports. Activities of daily living were defined as basic actions of self-care (e.g., washing, dressing, eating, and mobility) while Instrumental Activities of Daily Living (IADLs) are those that require a greater degree of cognitive ability (e.g., paying taxes, shopping, and preparing meals).19
Cutoff scores for defining cognitive impairment were derived from the recommendations of the original authors or subsequent reviews of Addenbrooke’s Cognitive Examination (ACE)10 (<82), Mini-Mental State Examination (MMSE)11 (≤24)11,20, and the Rowland Universal Dementia Assessment Scale (RUDAS)12 (≤22)12,21 using thresholds with an established high specificity for dementia. The Montreal Cognitive Assessment (MOCA)13 cutoff of less than 21 was chosen based on a study by Cheung and colleagues22, taking into account the information provided by the MOCA13 which, although indicating a cutoff of 26 to differentiate normal cognition from mild cognitive impairment, indicates that the optimal cutoff point for predicting a dementia diagnosis was less than 21.
Data were analyzed utilizing SPSS (Version 21), using descriptive statistics, chi-square tests or Fisher exact tests, as appropriate. Approval for this project was obtained through the Awhina Research and Knowledge Centre after locality approval by the Mason Clinic Research Forum.
Results
Demographics
Table 2 summarizes the demographic information for the sample. The mean age for the group was 68.5 years, and most were over 65 years of age (n = 70, 72%). The majority were male (93%) and Caucasian (56%). Māori, the indigenous people of New Zealand, were the next most common ethnic group (23%). Only one quarter of the sample (24%) lived alone, while it was most common for subjects to live with family (42%), including spouses and extended relatives. Most had offspring (85%). Over one-third (34%) had experienced significant trauma, including life-threatening experiences (vehicle accidents, physical abuse, sexual abuse, loss of loved ones to accidents, war, and torture). Regarding prior criminal history, the majority had previously been incarcerated (62%), with 31 percent previously convicted of violent crimes, and 19 percent convicted of sexual crimes. The age at first offending for those who had previously been convicted ranged from 13 to 78 years.
Demographics
Substance Use History
Table 3 summarizes substance use history. Half of the study subjects were noted by the forensic evaluator to have a history of problematic substance use (n = 48, 49%), including diagnosis of a substance use disorder. Current alcohol misuse was common (n = 35, 36%). As well, 13 (13%) had a record of inpatient treatment for drug or alcohol use.
Problematic Substance Use History
Medical History
The medical histories of the subjects are summarized in Table 4. Major neuro-cognitive disorders (38%), hypertension (36%), and heart disease (33%) were the most common. Only four (4%) of the sample did not have any significant health problems. At least half (n = 50, 52%) had been prescribed medication related to their physical health.
Medical Historya
Psychiatric History
One-third of the sample had previously been admitted to a psychiatric hospital (n = 32, 33%). Fifteen of the 72 evaluations commenting on suicide (21%) indicated a history of a suicide attempt.
Cognitive Evaluation
Cognitive testing was completed for 64 (66%). The MMSE was most frequently used (n = 36), followed by the ACE (n = 25), the RBANS (n = 5), the MOCA (n = 2), and one using the Cognitive Assessment of Minnesota. (Several defendants were given more than one test.) According to the predetermined criteria, 13 scored below the cutoff on the MMSE, 17 did so on the ACE, three on the RBANS, one on the MOCA, and none on the Cognitive Assessment of Minnesota, for a total of 30 (31%) scoring below the cutoff.
ADLs were not impaired in most, with over two-thirds (n = 68, 70%) being fully independent. Sixteen (16%) had difficulties completing IADLs, however, and 13 (13%) had impairment in even basic activities of self-care.
Psychiatric Medication Use
Less than half of the sample were known to be prescribed psychiatric medication at the time of the evaluation; 42 percent (n = 41) were specifically noted not to be prescribed medication, and medication use was unknown in 15 percent (n = 15). Only one individual had been prescribed medication for dementia. The most common psychiatric medications prescribed were antipsychotics (n = 21, 22%), followed by antidepressants (n = 20, 21%), mood stabilizers (n = 13, 13%), and anxiolytics (n = 8, 8%). Those facing non-sexual charges were more likely to be prescribed antipsychotic agents (44%, 18 of 41) at the time of assessment than those facing sexual charges (9%, three of 35) (p = .008).
Forensic Evaluation & Court Outcomes
Table 5 summarizes the psychiatric diagnoses made at assessment by evaluators. Cognitive impairment or disorders were by far the most common (42%), followed by substance use disorders (16%), mood disorders (15%) and psychotic disorders (14%). Fifteen subjects (15%) referred for forensic evaluation were not found to have any diagnosable psychiatric condition. Mental disorder as defined by the MHA was opined to apply to 42 (43%) of the subjects. Few had PPPR Act court orders or activated Powers of Attorney (n = 5; 5%) and only five others, at the time of assessment, were already under consideration for PPPR Act application or EPOA activation.
Psychiatric Diagnoses at Forensic Assessmenta
Reports solely investigating competency to stand trial were the most common reports ordered (n = 50, 52%), followed by risk assessment/disposition (n = 42; 43%), insanity (n = 2; 2%), reports investigating all three topics (n = 2; 2%), and competency to stand trial combining risk assessment and disposition (n = 1; 1%).
The alleged offending was violent in 32 (33%) cases, including primarily assaults, but also assaults with instruments, manslaughter, and murder charges. The majority of the sample were on bail at the time of assessment (n = 61; 63%), with the rest (n = 36; 37%) remanded in custody. Of those remanded in custody, one was treated at a locked inpatient geriatric psychiatry unit, and one other was an inpatient at the forensic hospital.
Of those evaluated for competency to stand trial, 60 percent (32 of 53) were opined to be unfit/incompetent; of the 32 recommended as incompetent, 27 were judicially determined to be incompetent to stand trial (28% of the entire sample). Of the four who were referred for NGRI evaluations, only one was opined to be insane and found insane; two died prior to judgment; and the fourth was found guilty on all charges. Ten defendants had their charges withdrawn. Among those diagnosed with cognitive impairment, two were incarcerated and two were found competent to stand trial, but disposition data were unavailable.
Treatment recommendations given by forensic evaluators are described in Table 6. Most commonly, recommendations were for treatment by community mental health teams (n = 31; 32%).
Treatment Recommendations Made by the Court Report Writera
Offending
Index offending (see Table 7) included historical offending in one-quarter (25%), with half of those (12% of total) having both historical as well as more recent index offending (within 10 years of assessment). The majority of victims were female. Friends and acquaintances were most likely to be victimized (40% of offenses involving victims) with adult strangers being next most common (24% of those involving victims) followed by their own children (17% of those involving victims). One had a child stranger victim. Most of the index offenses were committed in the subject’s own home, followed by the residences of the victims for over one-third of offenses. Of note, over one-third lived with their victim at the time of the index offense. Alcohol use around the time of alleged offending was noted in one-quarter (n = 26; 27%).
Characteristics of Alleged Offendinga
Under 65 versus Older
There was a higher prevalence of major neurocognitive impairment among those aged 65 and over (n = 34; 49%) compared with those aged 60 to 64 (n = 4, 15%; p = .001). Otherwise, no significant differences regarding any of the aforementioned variables were found between the age groups.
Sexual Offending
Thirty-eight in our sample (39%) were facing sexual charges (see Fig. 1). Of these in whom the presence of past charges was known, 15 (42%) had prior sexual convictions. The vast majority of the sample facing sexual offending allegations were men (n = 37; 97%), aged from 20 to 78 years at the time of the alleged offending.
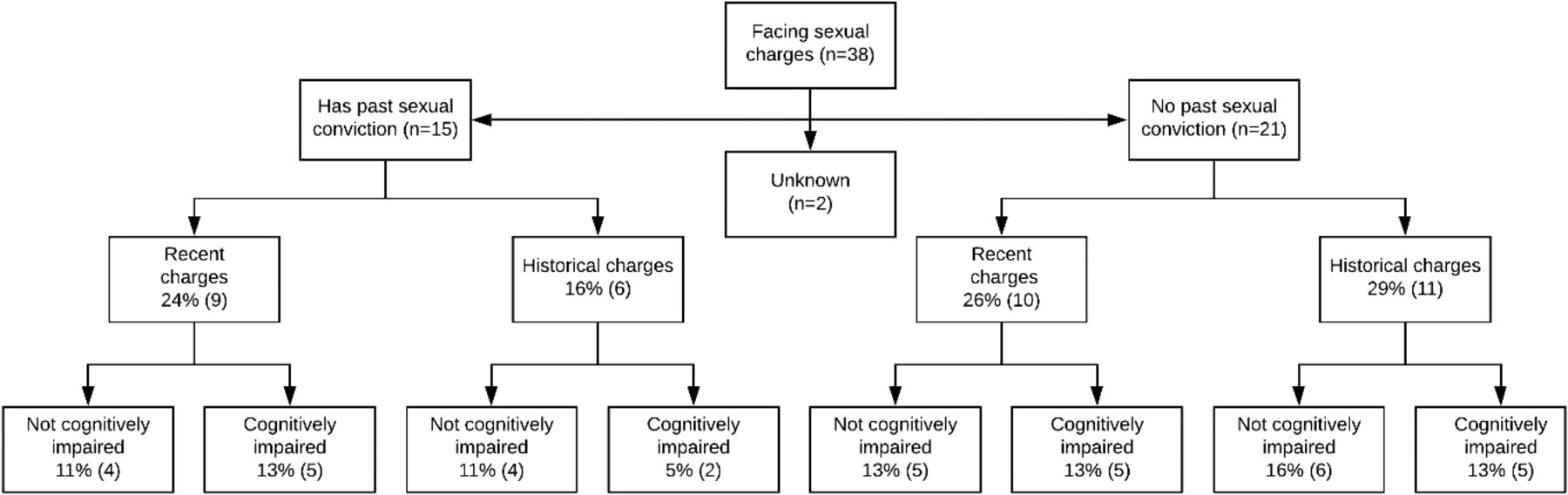
Subgroups of alleged sexual offenders (n = 38).
Among the 38 defendants facing sexual charges, 28 had alleged sexual offenses of more than one charge type. Types of charges faced by these 38 included indecent assault (28 defendants); unlawful sexual connection (18); indecent act (14); rape (12); attempts to rape (5); sexual connection with a young person (3); induce/permit indecent act (3); abduction for sex (2); parent incest with child (2); indecent act with intent to insult (2); committed sodomy (1); attempted sodomy (1); assisting person under 18 in providing sexual services (1); dealing with people under 18 for sex (1); and making a contract for commercial sexual services from a person under 18 (1). (Of note, adult prostitution is legalized in New Zealand.)
Only four of those 38 defendants were facing a single sexual charge, and these four had charges of: performing an indecent act on a boy aged 12 to 16; indecent assault upon a girl under the age of 12 years; indecent act upon a girl under 12; and indecently assaults female over 16 years.
Seventeen (47%) of the alleged sexual offenders were diagnosed with cognitive disorders at assessment. Only five (13%) were diagnosed with substance use disorders. Paraphilic diagnoses were made in two cases (5%), both pedophilia.
The types of alleged sexual offenders were further classified into sub-groups based on factors of prior sexual conviction, recency of alleged offending, and cognitive impairment as noted in Figure 1 (2 of the 38 had missing information). One quarter (9 of 36) had both prior sexual convictions, and more recent sexual charges. Another quarter (10 of 36) had no history of convictions for sexual offenses but faced recent charges. Within this group, some had evidence of cognitive impairment. Finally, some had no prior sexual convictions but were charged with historical sexual offending (two had both historical and recent sexual offending and were not noted to be cognitively impaired). It is worth noting that, in this group, the alleged periods of offending for those with “non-historical” offenses also were not recent but had fallen just short of the ten-year threshold defined for the study.
Nine of the alleged sexual offenders (24%) were alleged to have victimized adults, 22 (58%) to have victimized children, and seven (18%) both adults and children. Thirty (79%) were alleged to have victimized people known to them. Partners were the alleged victims of two (5%) and their own children in 10 cases (26%). Of those who involved their children, all but one involved daughters, either solely or included both sons and daughters. Those who victimized other family made up 24 percent (n = 9) of this subgroup, acquaintances accounted for 42 percent (n = 16), and strangers accounted for 18 percent (n = 7).
Disposition of Elderly Alleged Sexual Offenders
Alleged sexual offenders were significantly less likely to be recommended for mental health follow-up (45%) compared with the rest of the study population (67%; p = .029). Alleged sexual offenders were largely incarcerated (n = 17, 45%) by the court. Eight returned home (21%), seven (18%) went into nonsecure residential care facilities, and two (5%) were sent to a secure dementia care facility.
Discussion
Forensic services have traditionally been organized around the assessment and treatment needs of young men, and to a lesser extent young women. Older offenders represent a growing number of forensic evaluation cases and are expanding within the prison population. The current study adds to the limited literature on this sub-group. This older group presents a different set of challenges to the forensic evaluator and to mental health services regarding diagnosis (including comorbidities), treatment, risk assessment, and placement.
In our sample, forensic evaluees age 60 and over were predominantly men, with high rates of prior offending. There were significant rates of cognitive impairment (42% of the total sample and 49% in those over 65). A recent study23 of Swedish forensic evaluees found that about half of those diagnosed with dementia were under 65; head trauma, alcohol, and cerebrovascular disease were most frequently the underlying pathology. Our sample also had a high prevalence of other physical health problems such as cardiovascular disease, metabolic disorders, and lung disease, reflecting the challenge faced by health care providers and the need for cooperation and coordination of correctional, geriatric, psychogeriatric, and forensic psychiatric services. Our findings were remarkably similar to those of Lewis et al.3 who found that 81 percent had a prior arrest history. Similarly in the present study, a high proportion had prior offending, including 62 percent who were previously incarcerated but also some first-time offenders. Consistent with the high rates of cognitive impairment, 28 percent of the evaluees in the current study were found incompetent to stand trial, whereas 32 percent of Lewis’s American sample were incompetent to stand trial. Similarly, Frierson and colleagues noted that 37 percent of defendants more than age 65 years were found incompetent to stand trial.2
Ekstrom and colleagues23 found that in those Swedish evaluees with dementia, crimes tended to be impulsive rather than premeditated, although the role neurocognitive disorder plays in recidivism has yet to be fully determined. Booth24 noted that though older offenders generally have a lower risk of reoffending, individual risk assessments are critical. For example, in cases of new-onset sexual offending and neurocognitive disorder, the risk of recidivism may be higher due to reduced cognitive function that exacerbates risk. We speculate this may include sexual disinhibition exposing latent aberrant sexual thoughts.
In a memory clinic sample, Liljegren and colleagues25 found new onset criminal behavior, including violent and sexual offending, was more likely in the behavioral-variant frontotemporal dementia than in those with Alzheimer’s disease. The high proportion in our sample facing sexual charges is consistent with Fazel and colleagues4 but higher than Lewis and colleagues3, whose sample had higher rates of violent crime. The increased proportion of violent or sexual crimes in the elderly may also reflect very low rates of other crimes such as arson, robbery, and assault in this age group.
Many in our sample were subsequently incarcerated. The rapidly growing aging prison population is increasingly the subject of review and policy development.26 Concerns about accelerated aging have led to recommendations that the prisoner group be considered old at 50 or 55 years, in recognition of high rates of physical morbidity and cognitive impairment. There is concern that lack of recognition of these support needs in the older prisoner group and failure to provide ADL supports and adapted environments may further disadvantage this group.26,27
Our findings prompted further attempts to consider a link between sexual offending and cognitive impairment in the elderly. The sample included many who had cognitive impairment, but these were not universally those who were offending for the first time in older age. Our attempts to categorize offenders lead us to conclude that some people who have offended earlier in life will continue to offend into old age. In this group, cognitive impairment may potentially add to the risk of offending. The majority of the sexual offending sub-sample had either convictions or charges for offenses more than 10 years prior to the assessment and only a small minority (13%) began offending (or at least were apprehended) for the first time in old age in the context of cognitive impairment. Though small in absolute numbers, a similar number of those who appeared to begin offending late in life had no cognitive impairment evident. (Of note, however, elderly defendants may have a higher vulnerability for fluctuating mental status such as may occur with new medication causing a change in mental status.)
Risk Management and Cognitive Impairment
Lewis et al.3 noted that 44 percent of their sample had dementia, which compares with 42 percent of our sample being diagnosed with neurocognitive impairment or disorder. In our sample, one third (33%) were accused of violent offending, compared with the majority (61%) in the American sample.
Victims among those in our sample tended to be those with whom the evaluees were frequently in contact as opposed to victims who were strangers and physically distant. This may relate to an increased likelihood of disinhibition in this population. Similarly, Lewis and colleagues3 had found neighbors and spouses to be the most common victims. This has important implications for risk management in these individuals; no matter what long-term options are considered, strategies to protect those with whom they are in contact should be implemented.
More than two-fifths of our sample were living with family and a quarter lived alone. Although many were ultimately incarcerated, a significant proportion (44%) of sexual offenders either returned home or were discharged to residential care, most to nonsecure settings. The risk of reoffending among those who have cognitive impairment is unknown, but one might assume that factors such as disinhibition, and a limited capacity to learn from threat of legal censure, add to risk of reoffending. The discharge of this group back to a setting where they are in proximity to family, friends, vulnerable older people, or children visiting residential care, raises cause for concern. Chua and colleagues4 noted that sexual offense victims often included vulnerable persons such as minors (grandchildren), the elderly, and those with intellectual disability. Although disinhibited sexual behavior is not uncommon in aged residential care, this group may pose a different set of risks which have potential to go unrecognized or unmanaged. One local solution for some men with dementia and sexual disinhibition has been all-male secure dementia care facilities. The demand for such facilities is likely to grow.
Recommendations for Evaluations
Our sample had high rates of cognitive impairment, compared with the prevalence in the general population over age 60, which is estimated to be 6.9 percent (ranging from 1.8 percent at age 60–65 to 12.5 percent at age 80–84).28 Forensic evaluators should consider the relevance of cognitive impairment and the temporal relationship with offending. Diagnosis of a cognitive disorder involves not just use of a cognitive assessment test but an interview with the subject, obtaining collateral history, and typically, neuroimaging and screening investigations for reversible causes of dementia, including thyroid function, vitamin B12, folate, syphilis, and HIV serology. A comprehensive assessment approach looking for fluctuating course or rapid onset, psychosis, or mood symptoms may also assist in detecting transient or reversible cognitive impairment. We recommend that cognitive evaluation, including gathering of collateral history focused on cognitive change, should be universal in older offenders, given the high prevalence and potential implications for competency, relevance to current and future offending, and subsequent risk management. One should keep in mind that secondary gain could potentially affect reporting by family members. Neuropsychological testing may be of assistance in defining the pattern and severity of deficits, and neuropsychiatric or psychogeriatric opinions may be useful when there are questions about the threshold for a dementia diagnosis or differential diagnosis for the cause of cognitive impairment.
In addition to collateral history, use of standardized cognitive testing tools such as the MOCA, ACE-III, and the Executive Interview (EXIT)29 should also be used to increase detection and reliability of diagnosis of cognitive impairment. Alcoholism and traumatic brain injury both may present with executive dysfunction. Assessors should remain aware of the limitations of any cognitive test. Vigilance for those with predominantly executive dysfunction as a consequence of disorders such as fronto-temporal dementia, brain injury, occult cerebrovascular disease, or substance abuse should be high as these conditions may present in people younger than 65. New-onset offending should also trigger a search for cognitive change, in particular executive dysfunction.
Selective neuropsychological testing in combination with a focused history and attention to relevant mental state features is also recommended where cognitive dysfunction is suspected. Where cognitive impairment is detected, careful consideration should be given to what supports the person may need with self-care and ADLs, whether their disposition is within the criminal justice system or in the community. Forensic psychiatrists should develop an awareness of how to access local health and support services for older people and consider consulting colleagues working in the field.
Whatever the legal circumstances, recommendations for living situation upon sentencing or release from prison, or for those found incompetent to stand trial should take into account an individualized approach to risk evaluation and management. Evaluating the risk of subsequent offending (or being victimized) should take into account the complexity of this group. This includes both those who offend sexually for the first time in late life, in the context of cognitive impairment, and those with an established propensity for offending whose risks may have altered (either increased or decreased) depending on cognitive and physical factors. Further longitudinal research may improve our ability to calculate the risk of recidivism in older offenders.
Current services may be ill-equipped for management of such individuals in the longer term. Significant rates of incompetency to stand trial and the irreversible, degenerative nature of dementia warrant that long-term options be considered. Rest homes and dementia facilities are often reluctant to accept high-risk individuals (e.g., those involved in the criminal justice system) and may be poorly equipped to mitigate risk for those they do accept. Neurocognitive disorders have been observed to accompany problematic behavior in these settings.30,31 Nursing homes would need to ensure the resident was not unattended when other patients’ grandchildren visited.24 There will be a tension between ensuring supervision and preventing isolation from the wider community. Tomaka and Thompson32 reported the negative effects of isolation on physical health (across multiple organ systems and diseases), whereas Holwerda and colleagues33 demonstrated that neurocognitive degeneration is linked to feelings of loneliness (though not necessarily social isolation), both in elderly samples.
Sending members of this population home after they are found incompetent to stand trial may increase risk to the community. For those who faced sexual charges, beds at secure dementia facilities were not readily available, despite half of them having been diagnosed as having cognitive disorders. What becomes clear is that none of these options sufficiently addresses the problems with risk and health management while optimizing outcomes for the offender.
Prisons may not be an appropriate long-term management option for many either. Upon incarceration, older inmates are often met with challenging environments (physically and socially) that promote poorer physical and mental health outcomes, as well as increased barriers to accessing important social and health services.34,–,37 Growing impairments to activities of daily living and victimization by other prisoners are key concerns for this population.37 Compassionate release, palliative care, and the need for services on release are other concerns.
Limitations
This study included all those referred for forensic evaluation in the geographic area, but not all those who allegedly offended. Our sample was aged 60 and above, whereas samples in prison settings have often included slightly younger age groups (e.g., over 50). We further separated 65 and above and below age 65 for analysis since 65 is often the cutoff in the general population in non-forensic studies. Our sample included people from an indigenous ethnicity (New Zealand Māori) not extensively evaluated in the past.
This study sample is relatively large considering the dearth of research into the elderly forensic population and more specifically elderly sexual offenders. This study was a retrospective record review, however, and therefore data were occasionally unavailable. Formal testing for cognitive impairment was not completed on all evaluees, and a range of screening tools with variable sensitivity were used, allowing for the possibility that cases of cognitive impairment were missed. The representation of ethnicities is consistent with younger local forensic populations but may have implications for generalizability outside of the New Zealand context. The sample size was also limited, especially in analysis of subgroups with violent or sexual offending, which could mask small but significant differences.
Conclusions
Forensic evaluators need to become more familiar with the assessment and management of disorders which more typically present in older age groups and consider how these disorders affect competency to stand trial, offending behavior, and managing future risk of reoffending. The assessment of dementia in forensic evaluations requires a different set of collateral history gathering skills and routine cognitive assessments to screen for cognitive impairment when this is suspected.
The predominance of sexual offending in the older age group also presents somewhat different diagnostic and risk assessment challenges. We have suggested an approach to the conceptualization of elderly forensic evaluees accused of sexual offenses (regarding new onset offending versus historical and new offending; and regarding the presence or absence of cognitive impairment), which we believe has utility for both clinical and medicolegal evaluations. Finally, we emphasize the need for better coordination between geriatric and forensic services, and advocate for the development of secure rest home facilities for those who are unable to be safely managed at home or in less secure residential care facilities.
Footnotes
Dr. Hatters Friedman is involved in the editorial leadership of The Journal; however, she did not participate in any aspect of this article’s review and acceptance.
Disclosures of financial or other potential conflicts of interest: None.
- © 2022 American Academy of Psychiatry and the Law





{kind=link}