


In 2006, during my forensic psychiatry fellowship, I observed an evaluation for restoration of firearm rights. Until then, I had been unaware that these types of proceedings existed. Because the petitioner in the case was a police officer, whose duties (and potentially his job itself) hinged on the outcome of the petition, I realized that laws that prohibit firearm possession can have a profound impact on some individuals, beyond what I had naïvely thought about before, namely, interference with hobbies such as hunting or target shooting, and relatively abstract concerns (for most people) about self-defense. This realization sparked a lasting interest in the subject of mental health firearm laws.
At the time, there were very few publications on the topic in the mental health literature that I could use to educate myself. Coincidentally, 2006 was also when Norris et al. published one of the first papers to provide a comprehensive review of mental health firearm laws.1 The stated purpose of that article was to “educate clinicians about the impact of firearms statutes and restrictions for their patients” (Ref. 1, p 1392). The authors also pointed out that “[c]linicians would be wise to familiarize themselves with the provisions of the relevant statutes in their particular states” (Ref. 1, p 1392). This advice, I will argue, is even more important now than it was in 2006. Unfortunately, few have heard or heeded it, and today many or perhaps even most American psychiatrists still lack sufficient knowledge of this critical subject.
Over the past decade and a half, a body of academic literature on mental health firearm laws has developed. I reviewed California's statutory scheme2 and with Sharma reported the results of our empirical research on restoration of rights proceedings in Los Angeles County.3 Gold and Vanderpool explicated the complexities of restoration of rights procedures in a set of two articles.4,5 Two recent books each include several chapters discussing mental health firearm laws in detail.6,7 Also in the last decade, the American Psychiatric Association has published and updated a Position Statement on mental health firearms laws,8 as well as two resource documents, one on so-called “red flag laws,”9 and another on restoration of firearm rights.10
Over a similar time frame, there has been increasing interest in the subject within AAPL. I conducted an informal, nonrigorous search of programs of past AAPL Annual Meetings, available in PDF format on the AAPL website, to identify presentations covering some aspect of mental health firearm laws.11 I found that for the six meetings between 2007 and 2012, that number ranged from zero to two presentations per year. In 2013, the count jumped significantly, to approximately seven. Although this did not reflect a lasting change, and some subsequent years have also had none or very few, in 2017 there were four presentations, and in 2018, six. Not counting the 2020 and 2021 virtual meetings, which had a smaller total number of presentations, the last year that an AAPL annual meeting had no posters, panels, or workshops addressing mental health firearm laws was 2015.
Mental Health Firearm Laws
Prohibition after Mental Health Events
The federal law prohibiting people with certain mental health histories from possessing firearms was enacted over half a century ago, in 1968.12 And, as anyone who pays even slight attention to American politics knows, the debate about how to regulate private firearm ownership in the United States has been raging for decades. Thus, one might wonder why it was not until the middle of the last decade that authors in the mental health field began to examine the complex subject of the federal and state firearm laws that affect people with a mental health diagnosis or a history of certain types of treatment, most often some form of involuntary detention or commitment. One factor may have been the passage of the Brady Handgun Violence Prevention Act in 1993.13 This law established the National Instant Criminal Background Check System, or NICS, a set of centralized, national computer databases, which became operational in November 1998. The noncriminal database, called the NICS Index, gradually accumulated the names of people prohibited from possessing firearms for mental health reasons. After several years of operation, the NICS Index remained relatively quite small, containing less than a quarter of a million names of individuals with a mental health prohibitor in 2004.14
Beginning in 2008, incentives provided by the NICS Improvement Amendments Act of 2007,15 as well as the increasing media and legislative attention in response to tragic mass shooting events in the 21st century, led a growing number of states to send their internal lists of prohibited persons, which they had previously not shared, to the NICS Index. By the end of 2021, the number of people who were listed in the NICS Index for a mental health reason had increased by roughly a factor of 30, to over 6.75 million.16 Thus, the likelihood of a psychiatrist encountering patients who are in the federal NICS Index database has dramatically increased in recent years.
The Gun Control Act specifies that people who have been “adjudicated as a mental defective” or “committed to a mental institution” are prohibited from possessing firearms.12 These two terms are explicated in the Code of Federal Regulations. “Adjudicated as a mental defective” is defined as a
determination by a court, board, commission, or other lawful authority that a person, as a result of marked subnormal intelligence, or mental illness, incompetency, condition, or disease: (1) Is a danger to himself or to others; or (2) Lacks the mental capacity to contract or manage his own affairs.17
“Committed to a mental institution” is defined as a
formal commitment of a person to a mental institution by a court, board, commission, or other lawful authority. The term includes a commitment to a mental institution involuntarily … [it] does not include a person in a mental institution for observation or a voluntary admission to a mental institution.17
It should be kept in mind that although emergency short-term detentions and voluntary hospitalizations are not addressed by the federal statute, some states prohibit firearm possession after one or both of these types of events.1,18
Because the federal prohibition is for life, and the NICS Index now provides a straightforward means to identify banned subjects at the point of attempted firearm purchase, an ever-increasing number of people have discovered that they are prohibited from possessing firearms, sometimes decades after an involuntary commitment. Some of these individuals have not experienced symptoms of mental illness for many years. Congress has not provided for a direct federal process for individuals to petition for restoration of firearm rights. Instead, states may choose to develop a process, which, if approved by the Bureau of Alcohol, Tobacco, Firearms, and Explosives, allows for restoration after a federal ban.4 Because some states lack such a process, there have been several lawsuits filed arguing that a lifetime ban with no feasible means of relief from the disability is a violation of the Constitution. Some of these suits have reached federal courts of appeal, which have been divided on the question.19,–,21 Such a “circuit split” is a common reason for the U.S. Supreme Court to review a given type of case. Although this has not occurred yet, if the highest court does weigh in, it could have a significant impact on state relief procedures, or perhaps lead to a change in the federal process.
Temporary Restraining Orders
There is a second, newer category of mental health firearm law that is highly relevant for psychiatrists: court orders restricting firearm access.22 These are often referred to colloquially as “red flag” laws. Such orders impose a temporary prohibition on firearm possession on the basis of current dangerousness to self or others. (Dangerousness may be due to symptoms of a mental illness or substance abuse, but this is not required in most of these statutes.) Laws providing for these types of court orders, referred to in some states as Extreme Risk Protection Orders (ERPO) or Gun Violence Restraining Orders (GVRO), have proliferated in recent years. They exist in 19 states and the District of Columbia at the time of writing.23 Although only a small minority of these jurisdictions provide for licensed mental health professionals to request the initiation of such an order, it is unquestionably important for practitioners in those jurisdictions to understand them. Also, in the future, there may be new laws affecting mental health practitioners in states that currently do not have them, or modifications of existing laws that add mental health professionals to the list of people who may request initiation of the order.
The American Gun Culture
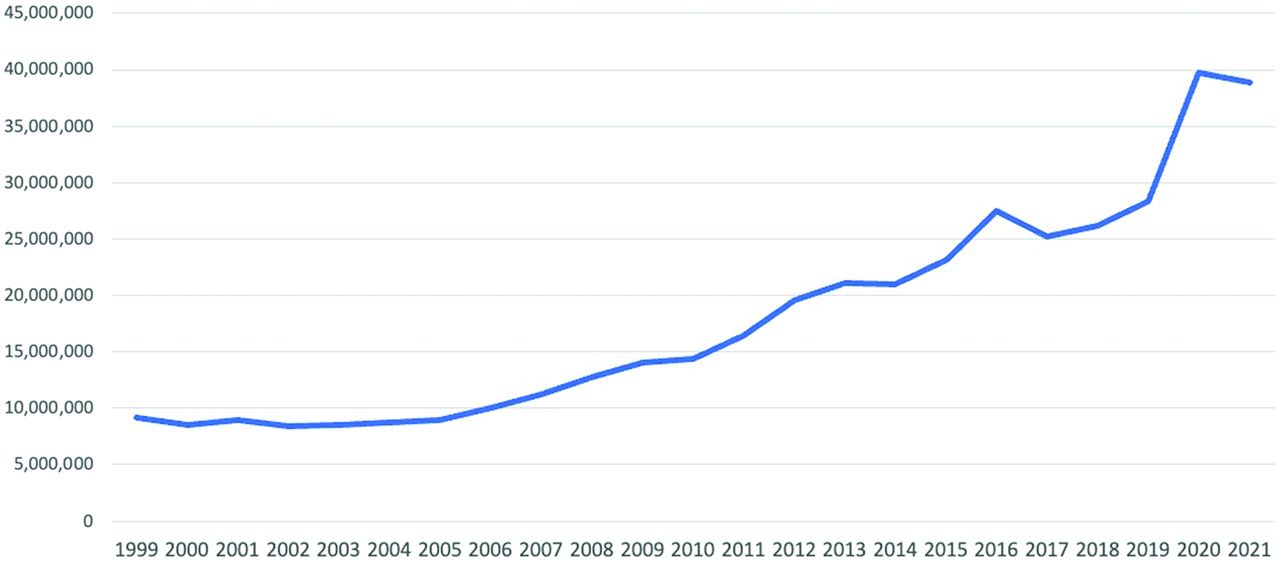
Echoing and amplifying Norris et al.,1 Pirelli and Gold argued in 2019 that knowledge about firearms (including mental health firearm laws as well as the “gun culture” in the United States) is “an essential competence” for mental health professionals.24 It is important to understand the ubiquity of firearms in the country. The United States has by far the highest per capita civilian firearm ownership in the world. A survey conducted in 2017 estimated the ownership rate at 120 firearms per 100 people.25 The second-ranked country, Yemen, had 53 per 100. The next 23 countries ranged from 39 to 19 per 100. And the collective American desire for firearms, though by no means uniform, has been increasing steadily. The number of attempts to purchase a firearm legally, as measured by NICS background checks, quadrupled between 1999 and 2021 (Fig. 1). Thus, even though the gun culture may be unfamiliar to some mental health professionals, the commonality of gun ownership in the United States, and its evident importance to many patients, means that all psychiatrists need to have knowledge of the federal firearm laws that may affect their patients as well as any such laws in the state(s) where they practice.

Number of NICS background checks by year, 1999–2021.26
The Current State of Knowledge
Despite the exhortations to learning by eminent authors such as those mentioned above, the fact remains that the average psychiatrist has a poor understanding of mental health firearm laws. This was demonstrated by two recent publications reporting on the results of surveys of psychiatrists. Newlon et al.27 surveyed over 500 psychiatrists, practicing in ten different jurisdictions, and found that many had mistaken beliefs regarding federal law or the laws in their state. Asked whether a court-ordered commitment leads to loss of gun rights, 37 percent incorrectly said it does not; because this is the federal law, it applies regardless of jurisdiction. For respondents in states where a voluntary admission is sufficient to cause the loss of gun rights, 57 percent incorrectly said it does not. The paper included some telling quotes from survey respondents, such as: “I was not aware … that involuntary admission results in revoking of rights to possess firearms” (Ref. 27, p 161), and “I was NOT aware that firearms could be restricted based off of involuntary commitments” (Ref. 27, p 162).
Nagle et al. conducted a survey of nearly 200 South Carolina psychiatrists.28 Out of five mental health firearm law knowledge questions, three were answered incorrectly by more than half of the respondents; only 61 percent correctly identified South Carolina's criterion for prohibition, that is, judicial commitment to a mental hospital. Only four percent of the survey respondents answered all five questions correctly.
There are a number of mistakes that psychiatrists insufficiently knowledgeable about mental health firearm laws might make, and they can only be briefly touched on here. They include providing incorrect information to patients or family members about the implications of voluntary or involuntary hospitalization for firearm rights; letting one's decision about hospitalizing a patient be influenced by misconceptions regarding the relevant laws; or conducting an inadequate evaluation when asked to clear someone for return of firearms or to perform a full forensic examination in a restoration of rights case. The result of a flawed evaluation could be continued prohibition for someone who does not pose a danger, or restoration of rights to someone who is foreseeably dangerous to themselves or others. Both would be an injustice, and the latter would by definition increase the risk of violence or suicide.
Responding to the Lack of Knowledge
In a commentary on the Nagel et al. article, I argued that forensic psychiatry fellowships should be required to provide education regarding mental health firearm laws.29 I have since changed my opinion: I now believe that the subject should be required earlier, in general psychiatry residency training.30,31 Over the last 16 years, I have given talks on mental health firearm laws in a variety of venues, including local and national forensic psychiatry conferences, the California state hospital system, grand rounds at university psychiatry departments and VA medical centers, and psychiatry residency and forensic fellowship didactic sessions. In keeping with the findings of Newlon et al.27 and Nagle et al.,28 the feedback I have most often received from audience members has been that they were only dimly aware even of the existence of mental health firearm laws. Very few have known anything about laws and procedures regulating restoration of firearm rights.
Given the widespread availability of remote lecturing following the COVID-19 pandemic, I contacted 11 psychiatry residency programs in the greater Southern California area in March 2021, offering to provide an online lecture covering the basics of mental health firearm laws, or to collaborate with their faculty in developing such a talk for the upcoming academic year. The response I received was not encouraging: only three programs expressed interest, of which two actually arranged for me to speak to their residents. I do not think this was because the other programs were not interested in the topic or had already addressed it in their syllabus. More likely, the directors believed that there was no room in their lecture schedule to incorporate additional, nonmandated subjects.
Norris et al.1 first called for psychiatrists to educate themselves about mental health firearm laws in 2006, and several others have done so since.7,9,10,22,24,27,–,31 My personal experience, in addition to the results of the surveys described above, indicate that despite the increasing impact of mental health firearm laws on our patients, few psychiatrists have availed themselves of the published information to educate themselves. As a group, they have not absorbed the information in the academic articles, or in the APA publications. The most effective way to rectify the situation would be for the Accreditation Council for Graduate Medical Education (ACGME) to make didactics on mental health firearm laws a psychiatry residency requirement.
Of course, the process of changing ACGME requirements is onerous and ultimately a drive for new requirements may not succeed. This does not prevent educators from exposing their residents to this critical subject voluntarily. Given the resources that now exist, it would be a simple matter for any faculty member to develop a lecture or two. Our field simply should not allow trainees to graduate and begin independent practice lacking such important knowledge.
Footnotes
The views expressed in this article are the author's own and do not reflect University of Southern California or University of Nevada, Reno policy.
Disclosures of financial or other potential conflicts of interest: None.
- © 2023 American Academy of Psychiatry and the Law





{kind=link}