


Abstract
Electroconvulsive therapy (ECT) is a safe and effective treatment used for numerous psychiatric conditions. While many patients for whom ECT is indicated are able to give voluntary informed consent, some lack decision-making capacity (DMC), at least temporarily. Case reports from numerous countries involving ECT for patients who lack DMC indicate overall positive outcomes and high patient satisfaction with results comparable with those of consenting patients; some patients regain DMC with ECT. Laws and regulations pertaining to ECT vary widely around the world and across the United States. Many United States jurisdictions over-regulate ECT relative to other interventions with comparable risks and potential benefits. While laws restricting whether and under what circumstances patients who lack DMC may receive ECT likely are aimed at protecting incapacitated persons, such laws sometimes undermine important ethics obligations and should be re-evaluated.
- decision-making capacity
- electroconvulsive therapy
- informed consent
- involuntary treatment
- nonvoluntary treatment
Electroconvulsive therapy (ECT) is used to treat numerous psychiatric conditions, including major depressive disorder, bipolar disorder, neuroleptic malignant syndrome, schizophrenia, schizoaffective disorder, catatonia, and mania.1,–,4 It also appears near the bottom of the treatment algorithm for several treatment-resistant psychiatric and neurological disorders, including obsessive compulsive disorder, dyskinesias, Tourette syndrome, epilepsy, and Parkinson's disease.1–2 ECT delivers electrical stimulation to the brain through electrodes placed on the head to induce cerebral seizures while patients are under general anesthesia. ECT is deemed safe and effective, yet some physicians hesitate to consider it as a legitimate option.5,–,10 Lack of experience with ECT, organizational structures or policies, legal uncertainties, subjective or emotional reservations, reliance on treatment algorithms that generally render ECT as a treatment of last resort, concerns about memory loss, and stigma might contribute to physician, patient, and family hesitance and result in under-utilization.5,–,7,9,11,12
There are isolated critics of ECT, including individuals who propose eliminating its use.13,14 Their criticisms are at odds with a large consensus body of literature demonstrating that quality of life and function generally improve in people who receive ECT.15,–,24 Lack of physician familiarity or comfort with ECT is explained largely by training deficits.8,25,–,27 Direct personal experience observing ECT is not a requirement for residency training in psychiatry, and some psychiatrists leave training without ever observing ECT.
While many patients for whom ECT is indicated are able to give voluntary informed consent, some lack decision-making capacity (DMC), at least temporarily. This includes patients with severe catatonia, severe suicidal ideation, or other severe psychiatric symptoms.5,28 Such patients face additional barriers to ECT. Inconsistencies in DMC assessments and the absence of an agreed-upon method for capacity assessment in the ECT context might help to explain the significant restrictions some jurisdictions impose on ECT for patients who lack DMC.29 It remains unclear what percentage of patients receiving ECT lack DMC. United States and European estimates range from one to three percent.8 There are studies and case reports from numerous countries (including France, Germany, Ireland, Japan, Scotland, Singapore, Taiwan, Spain, and the United States) that involve ECT for patients who are unable to consent. These studies indicate overall positive outcomes and high patient satisfaction with results comparable with those of consenting patients; some patients regain DMC with ECT.5,28,30,–,41
Laws and regulations pertaining to ECT vary widely around the world and across the United States.8,29,39,40,42 Many U.S. jurisdictions regard ECT differently from other interventions with comparable risks and potential benefits, contrary to the American Psychiatric Association's (APA) recommendations.1 ECT can be life-saving and has been shown to improve quality of life and function.15,–,24,43,–,45 ECT risks must be evaluated in light of the risks associated with the patient's condition, which can include death. In terms of mortality, the risks of ECT are low.46,47 The primary risks and side effects of ECT involve transient problems with recent memory loss that resolve over a few days or weeks. These cognitive side effects can be minimized by the use of right unilateral electrode placement instead of bitemporal placement and the use of ultrabrief pulse stimuli.1,48 Authorization by legally authorized representatives (LARs) routinely is accepted for patients who lack DMC to undergo far riskier procedures as well as procedures with comparable or worse side effects. For instance, the risk of “chemo brain” or cognitive impairment associated with some medications prescribed for overactive bladder syndrome are wide-ly accepted and do not typically lead to additional restrictions on consent or authorization by surrogates.49,–,51
The lack of alternatives to ECT from the 1930s and into the 1960s and its application to many different psychiatry disorders during that time might have contributed to the over-regulation of ECT relative to other medical treatments.29,42,52 Various laws address minimum age for eligibility to receive ECT, provider eligibility, how to obtain and document informed consent, reporting and other administrative obligations, and the conditions for treating patients who lack DMC.8,29,39,42 Today, more is known about the safety and efficacy of ECT with respect to improved quality of life and function.15,–,24 Improvements in the technique of ECT, including the use of ultrabrief pulse stimuli and the use of right unilateral stimulus delivery, have reduced the cognitive side effects of ECT with virtually no reduction in efficacy.48,53 This suggests that current restrictions do not reflect present-day evidence. While laws restricting whether and under what circumstances patients who lack DMC may receive ECT likely are aimed at protecting incapacitated persons, such laws sometimes undermine important ethics obligations and should be re-evaluated.
DMC, Nonvoluntary ECT, and the Law
The term “involuntary” often refers to any intervention without the patient's voluntary informed consent. Sometimes it describes treatment against the patient's wishes.8 Following others, we distinguish between involuntary and nonvoluntary treatment to acknowledge important differences among patients that raise different ethics considerations.54 As Figure 1 illustrates, we use involuntary treatment to describe treating patients who have DMC without their voluntary informed consent. Sometimes such compulsory treatment of patients with DMC is justifiable through the police powers of the state when they pose an imminent threat to themselves or others and the treatment is necessary, reasonable, and proportional to the harm to be avoided.55 Examples include some instances of vaccination, isolation, and quarantine. Compulsory ECT is rarely, if ever, indicated.56
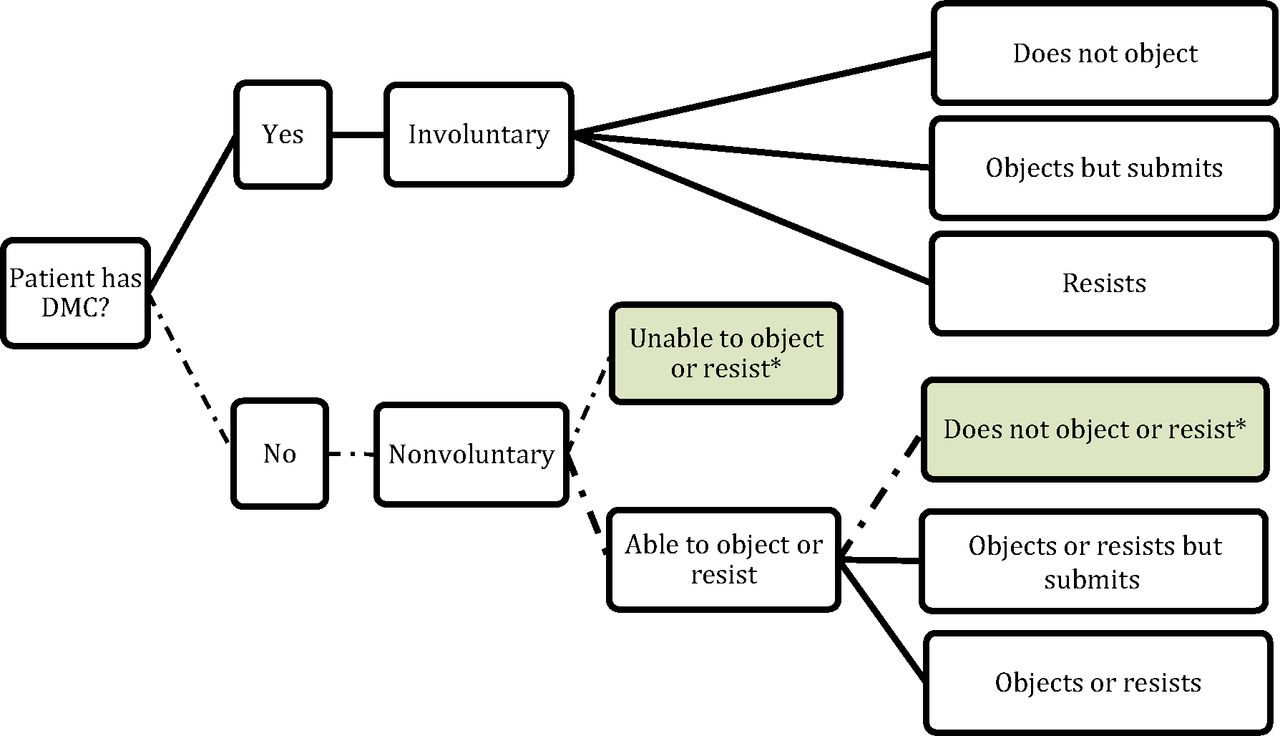
Treatment in the Absence of a Patient's Voluntary Informed Consent.
* These are the circumstances this paper addresses.
Nonvoluntary treatment refers to treating patients who lack DMC and thus are unable to give voluntary informed consent or make an informed refusal. DMC assessments are medical judgments regarding patients' ability to understand and appreciate relevant information, use that information to reason about treatment options, and make and communicate a decision.57 Typically, when adults lack the capacity to make their own health care decisions, LARs may serve as surrogate decision-makers. In the United States, LARs may be appointed by the patient (durable power of attorney for health care), designated based on their relationship to the patient as determined by state law or local policy or practice, or guardians assigned by a court. LARs receive information that typically would be part of the informed consent process. They are responsible for making decisions based on the patients' previously expressed wishes, if they are known. Where patients' wishes are not known, LARs apply substituted judgment, making decisions based on what can be inferred from available knowledge of the patient. Where that is not possible, the best interest standard (BIS) guides decisions.58,59 We address strictly nonvoluntary ECT, that is, ECT for patients who lack DMC and thus cannot give voluntary informed consent. We focus on patients who lack DMC and are not actively resisting treatment because active refusal of an invasive intervention, possibly resulting in the use of force, raises additional ethics considerations.60,61
In the United States, many states and the District of Columbia restrict nonvoluntary ECT by limiting the authority of LARs and court-appointed guardians to consent to ECT.29,42 One might think of these laws as preemptive applications of states' parens patriae powers. These powers concern the care and protection from harm or neglect of persons unable to protect and care for themselves, namely children and incompetent adults.55,62 Laws restricting nonvoluntary ECT might seek to reduce the likelihood that ECT will be provided when it is not in the patient's best interest or is not what the patient would have chosen. In some states, such as Oregon, patients who cannot make their own decisions and are hospitalized for treatment may not receive ECT.63 Numerous states require court involvement for nonvoluntary ECT.42 In some, such as Minnesota, a court must authorize LARs or guardians to consent to ECT.64 In others, such as Arkansas, patients who lack DMC may receive ECT only when a court authorizes the treatment.65 It is unknown whether ECT, including for patients without DMC, is treated differently from other medical decisions in states where the law is silent.
ECT sometimes is indicated urgently to prevent death or serious irreversible harm for patients who cannot provide consent.32,35 With a few exceptions, such as Illinois, state laws restricting ECT for patients who lack DMC often have no provisions for emergency ECT.66 In Texas, ECT for patients who lack DMC requires authorization of a court-appointed guardian rather than a surrogate decision maker; it can take several weeks to appoint a guardian.35,67 A case report from Texas concerns a patient who lacked DMC and whose spouse was willing to authorize ECT but was prohibited from doing so by Texas law.35 The patient was treated successfully only after the physician, hospital attorneys, and the spouse, with input from a court investigator, concurred that they could characterize the situation as a medical rather than a psychiatric emergency. This enabled them to invoke the Texas Emergency Health Care Act to justify ECT without patient consent or authorization of a court-appointed guardian.68 In most emergencies, physicians are not required to consult with hospital attorneys and court investigators to provide treatment necessary to prevent serious harm or death, nor are surrogate decision makers prohibited from authorizing medical treatment deemed necessary to prevent serious harm or death. The patient in this case regained DMC after ECT and consented to further ECT treatments.35 Without the creative application of the Texas Emergency Health Care Act, the outcome likely would have been very different. It is not known how many patients who lack DMC and could benefit from ECT never are treated because of administrative and legal burdens and delays.
Ethics Considerations in Nonvoluntary ECT
Decision-making regarding ECT for incapacitated patients has been described in terms of balancing tension between respecting patients' rights or autonomy, preventing harm (nonmaleficence), and doing good or promoting health (beneficence).30,56,69,70 ECT-specific laws and regulations appear aimed at balancing the first two of these obligations. First, they seek to protect patients' rights to refuse treatment and give voluntary informed consent (e.g., laws that require disclosure of specific information as part of the consent process or that allow LARs to authorize ECT only when the patient has granted this authority in an advance mental health care directive). Second, they seek to protect patients from harm (e.g., laws restricting who may prescribe and administer ECT, requiring verification by additional physicians or facility administrators that ECT is warranted and offers a greater prospect of benefit than harm, and mandating ongoing training or reporting). At least one state, Connecticut, limits ECT to cases in which no other treatment option is available or all other options have been exhausted.71 Some states, such as Virginia, require clear and convincing evidence that ECT is necessary.72 Many of these laws impose burdens on patients with psychiatric disorders and their families that do not apply to patients with physical conditions. This unduly burdens a population based on their health status. It suggests that psychiatric illness is not as serious as physical illness and perpetuates disparate treatment of mental and physical health.
Appropriately balancing competing ethics obligations requires a comprehensive understanding of the full range of relevant obligations and their implications. As demonstrated below, some restrictive ECT laws may not appropriately balance respect for incapacitated patients' rights and protection from harm, and they fail to give sufficient attention to at least two other obligations, doing good by promoting health and treating people equitably.
Patients' Rights or Autonomy
In the United States, respect for patients' rights is often described in terms of respect for autonomy.70,73,74 These rights include individuals' right to make voluntary informed medical decisions, to select persons to make decisions on their own behalf if they lack DMC, to make decisions in advance regarding treatment preferences if they lose DMC, and to have their known values and preferences inform decisions others make on their behalf. Laws requiring the disclosure of specific information about ECT or particular practices for documenting consent, and laws restricting ECT based on what is specified in advance mental health care directives appear grounded in this obligation. Some laws that restrict nonvoluntary ECT undermine or strip away some of these rights. Requiring court authorization for ECT rather than allowing LARs to consent to treatment could be seen as violating patients' right to have LARs (who are chosen in advance or appointed because of their relationship to the patient) make decisions on their behalf, rather than having strangers do so.
Laws restricting nonvoluntary ECT might be grounded in the assumption that patients would not want ECT because of the public's general negative attitudes toward ECT.74 Yet, studies of patients' perspectives after receiving ECT, including studies of patients who received ECT nonvoluntarily, suggest that the majority saw it as beneficial and many of them are or would be willing to undergo ECT in the future.5,28,37,60,75,–,77 Although patient satisfaction studies and studies that focus on hypothetical choice face numerous problems and patient perspectives vary across studies, they provide support for the view that patients who lack DMC would not necessarily want to refuse ECT were they able to make voluntary informed decisions.75,78,–,80
Making ECT inaccessible or far less likely to be used in patients who lack DMC also might deny them treatment that could help to restore their DMC. Several studies and case reports of nonvoluntary ECT note that many patients regained DMC after nonvoluntary ECT.5,32,35,60 Restricting nonvoluntary ECT in the name of respect for autonomy might undermine autonomy by denying patients access to an intervention that could help to restore their DMC and thus enable them to exercise their autonomy.
In many countries, there has been growing attention to mental health advance directives, also called psychiatric advance directives.81,–,87 Until such time as individual states revise laws in a direction that is less prejudicial toward psychiatric treatment, patients in those states may need to complete psychiatric advance directives that protect their ability to receive treatment authorized by their LARs in the future. Given existing laws in some states, such as Texas, even patients with explicit directives might have to have a legal guardian appointed to receive ECT.67 In the United States, advance directives that prohibit potentially life-saving medical treatment ordinarily are expected to be honored. Thus, although sometimes directives may be overridden, patients who want to refuse particular treatments in the future, including but not limited to ECT, also may complete directives to this effect.88
Do Not Harm
Perhaps the most widely cited fundamental obligation of physicians is, “First, do no harm.”73 Laws restricting who may provide ECT and where, requiring that multiple parties agree that the patient needs ECT to avoid interventions that pose more risk of harm than potential benefit, mandating use of less invasive therapeutic interventions before resorting to ECT, and requiring ongoing training appear grounded in the ethics obligation of nonmaleficence. Yet, laws restricting nonvoluntary ECT can result in delays that increase morbidity and mortality.52,56,89,–,92 In addition to published case reports regarding the negative impact of ECT treatment delays or prohibitions for patients who lack DMC, psychiatrists from throughout the United States shared with us examples of such situations. While we cannot share details of those cases as a matter of patient privacy, they illustrated how legal barriers to accessing ECT can result in harm. Examples included self-harm, contractures, bowel and bladder incontinence, bed sores, and medical complications of catatonic stupor (such as inanition requiring percutaneous endoscopic gastrostomy (PEG) tube feeding). We abstract from these examples to demonstrate some of the ways legal restrictions could harm patients. Consider, for example, the Kansas law that allows guardians to authorize ECT only if guardianship papers specifically include this authorization.93 For patients who have medical guardians, but the guardianship papers do not mention ECT, treatment with ECT will not be possible until a court revises the guardianship order. Similarly, in Texas, persons who lack DMC may receive ECT only after being adjudicated incompetent to manage their affairs, having a legally appointed guardian named, and obtaining the guardian's authorization.67 Both laws can result in significant expense and delay, creating the possibility that a patient will deteriorate. Sometimes, families may be unable to afford to pursue guardianship or to have the scope of their guardianship updated. This will leave them unable to authorize ECT.
Some laws both in the United States and elsewhere render ECT inaccessible for some patients, denying them access to a safe and effective intervention.28,37,40 ECT-restrictive laws might contribute to the stigma associated with receiving or providing ECT and mental health treatment more generally, resulting in additional harm.94,–,96
Do Good or Promote Well-Being and Health
Numerous studies and case reports indicate that ECT is a safe and effective treatment for a number of conditions, that it might be the only effective treatment in some cases, and that patients who lack DMC can benefit from ECT as much as those with DMC.5,28,31,–,34,36,37,42,52,60,69,76 Laws that significantly restrict ECT and make it inaccessible or far less accessible for some patients can undermine physicians' ability to fulfill their obligation to benefit patients or to do good and promote health.56 Such laws appear not to give due consideration to physicians' obligations of and patients' interest in bene-ficence, giving far more consideration to narrow interpretations of the duties to respect rights and avoid harm. Where the law allows ECT only as a last resort, physicians may be required to provide ineffective or less effective treatments.
Treat People Fairly or Equitably
Discussions of justice, understood as the obligation to treat people fairly or equitably, often focus on social justice today, emphasizing access to health care coverage and health disparities associated with race or socioeconomic status.73,97 Yet, fairness and equity also concern factors that may contribute to disparities in treatment or outcomes such as disability status and age. Legal restrictions on ECT in general, and nonvoluntary ECT in particular, can result in increased costs and other burdens that decrease the likelihood of people receiving treatment even where they legally could do so through court involvement.42 Laws that severely restrict access to ECT for patients who lack DMC could be seen as unfairly discriminating against patients based on their disability. They deny patients access to a safe, effective, and necessary medical treatment because their health status renders them unable to provide informed consent. This is particularly poignant in states where nonvoluntary ECT for patients hospitalized medically and psychiatrically are treated differently, requiring court involvement for the latter but not the former. The Texas case described above in which ECT could be provided emergently for medical indications without a court-appointed guardian but not for a psychiatric indication illustrates this.35 Similarly, in Massachusetts a special Rogers Guardianship is required to administer “extraordinary treatments,” including ECT, for patients with mental illness who lack DMC.98 No comparable requirement is in place for patients with physical conditions who lack DMC and require ECT. In limiting or delaying access to treatment, such laws also might contribute to or exacerbate health disparities that people with psychiatric disorders experience, undermining health promotion and harming patients.99
Conclusion
A comprehensive understanding of the ethics considerations relevant to nonvoluntary ECT suggests that some legal restrictions on ECT for patients who lack DMC might be unethical in light of the available evidence regarding safety, efficacy, and patient satisfaction with ECT.30 Instead of protecting patients, they may undermine patients' best interests, lead to harm, treat people inequitably based on their disability status, and deny some patients access to treatment that could restore their DMC and promote autonomy. Such laws should be re-evaluated.
Psychiatrists should consider advocating for legal reform so that laws are consistent with the APA's recommendation to treat ECT comparably to how those laws treat other medical interventions with similar risk-benefit profiles. Such advocacy is consistent with Section 3 of the American Medical Association's Code of Ethics, which the APA has adopted, and which states: “A physician shall respect the law and also recognize a responsibility to seek changes in those requirements which are contrary to the best interests of the patient.”97
Guidance, such as a model institutional policy, should be developed to inform nonvoluntary ECT decisions and delivery. In the development of policies and practices, patients who lack DMC but actively refuse ECT raise special concerns that merit additional attention.60 The policy development process should engage stakeholders and experts, including patients, family members, psychiatrists, and individuals with expertise in ethics and law. This would be consistent with the commitment to patient-centered care in psychiatry and across medicine and other efforts to involve patients in developing health care systems and services to improve quality, accessibility, acceptability, and outcomes.100,101 Additional research on nonvoluntary ECT also should be conducted to guide policy and practice.
Acknowledgments
We are grateful to Professor Christine Coughlin from the Wake Forest University School of Law for her guidance with legal research.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2023 American Academy of Psychiatry and the Law
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵





{kind=link}