


Abstract
Justice-involved youth experience a high number of mental health symptoms. There has been an increased effort to address the mental health needs of these youth through specialized juvenile mental health courts (JMHC). To date, there have been few studies that examined characteristics related to successful completion of a JMHC program. This study is a retrospective case file review of 99 individuals ages 10 to 18 years who were involved in a JMHC program. Information collected included educational history, parental factors, psychiatric and abuse history, legal history, risk of removal from home, and risk and protective factors from the Structured Assessment of Violence Risk in Youth (SAVRY) measure. The primary outcome was successful completion of the program. Forty-eight participants (48.5%) successfully completed the program. Neglect, removal from the home, new charges, probation violation, and number of previous charges were negatively associated with successful completion. Positive attitude toward intervention was positively associated with successful completion. Measures that juvenile justice systems may use, such as the SAVRY risk factors and abuse and neglect screens, were not associated with completion. More studies are needed to identify factors associated with successful completion of a JMHC program and to develop interventions to improve outcomes.
In the United States, a large population of youth are involved with the juvenile justice system, with 728,280 arrests of persons younger than eighteen years in 2018.1 Multiple studies have established that justice-involved youth have higher rates of maltreatment history and mental health diagnoses than the general youth population.2,–,5 Up to 100 percent of justice-involved youth report criteria consistent with at least one mental health diagnosis,6 and many have multiple mental health diagnoses. Drerup and colleagues identified criteria for one mental health diagnosis in 92 percent of male youth and 97 percent of female youth involved in the juvenile justice system.7 In the same study, 34 percent of males and 60 percent of females met criteria for three or more mental health diagnoses.
Justice-involved youth have high rates of maltreatment history compared with that of the general population.2,–,5 More than 67 percent of males and more than 75 percent of females involved in the juvenile justice system report a history of physical abuse, and more than 10 percent of males and 40 percent of females report a history of sexual abuse.2 Rates of neglect among justice-involved youth are also higher than the general population, with 30 percent of justice-involved youth having a history of neglect.3,8 A history of maltreatment in the form of neglect may also confer increased risk of becoming involved in the justice system compared with experiencing physical or sexual abuse.8,9
Justice-involved youth with histories of trauma experience an average of five distinct traumas, with the majority of those occurring in the first five years of life.3 In a study of 350 youth involved in family court, juvenile detention, residential facilities, and juvenile court, 94 percent reported a history of one or more traumas, defined as natural disasters, serious motor vehicle accidents, the unexpected death of a loved one, being the victim of a mugging or robbery, assault resulting in bodily harm, childhood physical and sexual abuse, and witnessing other disturbing, terrifying, or distressing events. Of this overall population, 45.7 percent met criteria for posttraumatic stress disorder (PTSD).9,10 Burke et al.5 found that while three quarters of 75 studied youth had evidence of a mood, anxiety, or behavioral health disorder at first contact with the juvenile court, only about 20 percent of justice-involved youth accessed mental health services over a three-year period. A diagnosis of Oppositional Defiant Disorder was most likely to precipitate contact with mental health services, and justice-involved youth meeting criteria for depression, anxiety disorders, and attention deficit hyperactivity disorder (ADHD) were less likely to have accessed mental health services.5 Eighty-five percent of justice-involved youth reported at least one barrier to accessing mental health services. Most frequent barriers included the belief that the problem will resolve on its own, uncertainty of where to find help, difficulty in accessing help, fear of others' perception, and cost.11 Brady and colleagues have outlined “structurally embedded stressors” in school, community, and home environments (such as socioeconomic stressors and inadequate access to care) as contributing factors for development of symptoms that manifest as externalizing behavior. Lack of resources often leads systems to focus on response to the externalizing symptoms rather than conceptualizing the etiology of those symptoms.12 This approach may be more likely to result in punitive responses rather than treatment interventions at a systemic level.
Family and social modeling may also mitigate or exacerbate depressive symptoms for justice-involved youth. Family support has been shown to reduce the report of depressive symptoms.13 Even nonparent family members (especially siblings and extended family) are important emotional supports for teens.14 Children receiving mental health services in the community are more likely to become justice-involved if their living situation is disrupted15 and to have more significant justice involvement as the number of their living transitions increases. Delinquency in adolescents with depression has also been associated with affiliation with other justice-involved youth and lack of prosocial involvement.16
Because of the large number of mental health diagnoses in the justice-involved youth population, there has been an increased effort to address the mental health needs of these youth. In a review by Lyons, et al. on the effect of linkage to mental health services on overall functioning and recidivism, 75 percent of eligible youth were successfully linked to mental health services, with subsequent improvement of depression, anxiety, and psychosis symptoms.17 Youth also demonstrated improved functioning in family and school settings and fewer dangerous behaviors.17 Recidivism was also reduced, with only 42 percent of youth who were linked to mental health services having another arrest, compared with 72 percent of all arrested youth.17
An increasingly popular method of addressing the mental health needs of justice-involved youth is the development of a Juvenile Mental Health Court (JMHC). The first JMHC in the United States was established in 1998 in Pennsylvania; by 2012, there were at least 41 JMHCs in 15 states.18 In 2020, the GAINS Center noted there were 56 JMHCs in 17 states.19 The programs are usually run through a juvenile court, or a probation agency, or a combination of the two.18 The most common diagnoses of youth involved in JMHC are bipolar disorder, depressive disorder, and ADHD, and about half of the JMHCs allow all youth with a mental health diagnosis to participate.18 Most JMHCs include both felony and misdemeanor charges.18 There are a number of characteristics that are common to nearly all JHMCs, which include: a regularly-scheduled special docket; less formal interaction style; age-appropriate screening and assessment for mental health, substance use, and trauma; team management of treatment and supervision; system-wide accountability; use of graduated incentives and sanctions; and defined criteria for success.20 The incentives most commonly used are gifts cards or other gifts, praise by the judge or probation officer, reduction in court hearings, and dismissal of charges.18 The most common sanctions are increased supervision, placement in detention, community service, and other tasks like writing essays.18 The JMHC facilitates access to mental health services, including individual outpatient treatment, family therapy, and case management, and guardian participation is almost always required.18 The average amount of time spent in a JMHC program is one year.18 Studies that have examined outcomes for JMHCs have found that youth who participate in a JMHC have lower recidivism rates.21,–,24 There are data suggesting a reduction in mental health symptoms for those who participate in a JMHC. 23
Despite the growing number of JMHCs, to date few studies have examined characteristics related to successful completion of a JMHC program. Reported rates of successful completion of JMHC programs range from 48 to 56 percent,22,23 although differing characteristics of these courts make comparisons more difficult. Heretick and Russell examined factors related to successful completion of a JMHC in Colorado and found that the number of court reviews and new charges while participating in the JMHC were statistically significant predictors of failure to complete the program.21 A study of characteristics related to success and failure in a juvenile drug court, a similar type of juvenile diversion program, found 46 percent of the youth successfully completed the juvenile drug court program.25 Youth with a higher number of prior offenses, more negative and antisocial attitudes, or a lifetime history of child abuse (not further defined) were less likely to successfully complete the program.25
The aims of this study are twofold. First, the study is descriptive, with the aim of characterizing the risk and protective factors of youth who had been detained and met criteria for involvement in a JMHC. The second aim is to determine which characteristics are predictive of successful completion of the JMHC probationary period. Success is defined as completion of the probationary requirements and dismissal from the JMHC. Failure is defined as termination of probation with subsequent removal to state custody. We hypothesized that youth who were at risk for commitment to state secure facilities based on a screening form at the outset of their probationary period would have lower successful completion rates compared with those youth who did not screen positive for risk for removal to state custody.
Methods
In 2005, a juvenile court serving a population of approximately 250,000 established a specialized court for juveniles with serious mental illnesses or developmental disabilities who commit delinquent acts. The purpose of this specialized court is to utilize a treatment-oriented disposition whenever possible, ensuring that the specific needs of juveniles with serious mental illness or cognitive disability are addressed appropriately while ensuring community safety and reducing the risk of recidivism. Juveniles adjudicated Delinquent or a child of a Family in Need of Services (FINS) and who are diagnosed with serious mental illness or cognitive disability are eligible for the program. Qualifying diagnoses include mood disorders, psychotic disorders, anxiety disorders, intellectual disability, autism spectrum disorders, and brain syndromes (including severe head injury). Youth with attention deficit hyperactivity disorder, oppositional defiant disorder, or conduct disorder alone do not qualify for inclusion in the JMHC. Individuals with substance use disorder as a single or most prominent diagnosis are excluded and referred to the local juvenile drug court.
The presiding judge, the prosecuting attorney, the defense attorney, the probation officer, and juvenile detention staff have the authority to refer youth for JMHC screening. Upon referral, the court's mental health coordinator conducts an assessment which includes The Massachusetts Youth Screening Instrument–Version 226 clinical interviews with the youth and family and review of historical documentation provided by outside mental health professionals, school representatives, and family members. If the mental health coordinator deems the youth potentially eligible for the JMHC, the youth is referred to a licensed clinical psychologist or psychiatrist for diagnostic evaluation. If assessments support placement in the specialized probation program, a treatment plan is presented to the JMHC judge. The JMHC charter requires that treatment plans embrace a wraparound philosophy that is strength-based, culturally relevant, and delivered in the least restrictive environment that ensures individual and community safety. Treatment plans might include individual therapy, family therapy, group therapy, emergency crisis services, medication management, educational support, family respite, skills building, and recreation programs. Therapies available include Multisystemic Therapy, Functional Family Therapy, and trauma-focused therapies. While involved in the JMHC, youth meet regularly with probation officers with a background in counseling and a master's level education. Probation officers meet face-to-face with each child at least once a week, maintain frequent contact with family, other natural supports, and the treatment team. Probation officers are available 24 hours a day and collaborate with the treatment team to de-escalate crises and enhance the stability in the child's environment. A licensed Master's level social worker, with a background in counseling, supervises the unit and provides guidance for treatment plans with a focus on cross-system collaboration and promotion of evidence-based interventions.
This study is a retrospective case file review of 99 individuals who participated in the JMHC program. All JMHC participants aged 10 to 18 were included, except for those admitted to an inpatient psychiatric facility at the time of the study. This study was approved by the Institutional Review Board at Louisiana State University Health Sciences Center, Shreveport, Louisiana and approved by Caddo Parish.
Measures
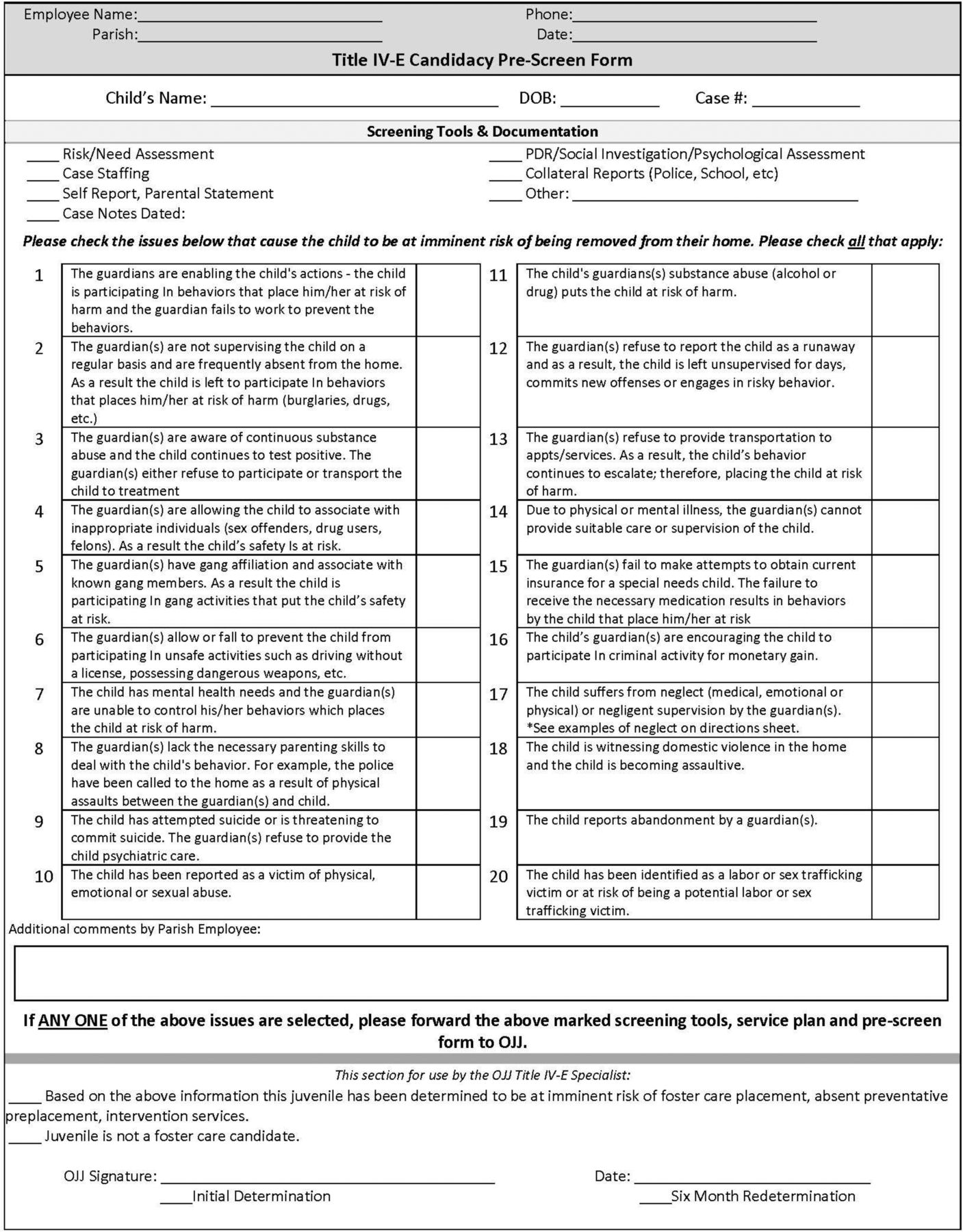
Information was collected by review of JMHC files, which included educational history, parental factors, psychiatric and abuse history, legal history, risk of removal from home, and risk and protective factors determined by the Structured Assessment of Violence Risk in Youth (SAVRY) measure.27 A list of items assessed on the SAVRY measure can be seen in Table 1. Risk of removal from the home was captured on the Title IV-E Social Security Act Foster Care Eligibility Form (Figure 1) completed by juvenile court staff for each youth. The Title IV-E Form queried for abuse and neglect risk factors resulting in an “at risk” or “not at risk” determination. The SAVRY is a validated measure that is composed of 24 items in the three risk domains of Historical Risk Factors (10 items), Social/Contextual Risk Factors (6 items), and Individual/Clinical Factors (8 items). The risk factors are rated as high, medium, or low risk. SAVRY risk factor scores were determined by quantifying each item (absent = 0, moderate = 1, high = 2) and adding all items. The measure also includes the presence or absence of six Protective Factors, which were summed for a total Protective Factor score. Each risk and protective factor's relationship to successful disposition was also analyzed individually.

Title IV-E Form.
SAVRY Risk Factors
Psychiatric history included number of psychiatric diagnoses, number of psychotropic medications, and pertinent history, including suicidal behaviors, nonsuicidal self-injury, psychiatric inpatient treatment, psychiatric outpatient treatment, and psychotherapy. Maltreatment history included history of physical abuse, sexual assault, neglect, past referral to Department of Child and Family Services (DCFS), and history of removal from the home.
Educational factors included history of special education, repeated grade, poor attendance, or placement at an alternative school. Parental factors included parental marital status, parental substance use, parental incarceration history, presence of parental mental illness, and whether both parents had graduated from high school. If participants were adopted, characteristics of adoptive parents were used. Legal history included number of previous charges, the presence of new charges during probation, and the presence of a probation violation. An “at risk” determination on the Title IV-E Form indicated that the individual was at risk for removal to state custody.
The primary outcome of this study is disposition from the JMHC program, with the outcome of interest being successful completion of the JMHC program. Successful completion is defined as release from probation after fulfillment of probation requirements. Lack of successful completion is defined as being removed to state custody or any other disposition, which included transfer to adult court for new charges, moving, or aging out of the program.
Statistical Analysis
We examined the association between successful disposition and the following factors: demographic variables (age, gender, race), psychiatric history, school history, parental history, legal history, and SAVRY scores.
Data were summarized as mean (standard deviation) or median (inter-quartile range) and frequency (percentage), as appropriate. Differences between groups were assessed using two-sided t test or Wilcoxon rank sum for the analysis of continuous variables. For the analysis of categorical variables, chi-square test or Fisher's exact test, as appropriate, was used.
To test the strength and direction of the association between each single predictor and the outcome variable (successful completion), three analyses were conducted. Because of the number of predictors, an unadjusted analysis (univariate logistic regression) was conducted to identify the significant variables to retain in the multivariate logistic regression. Based on the likelihood ratio test outcomes of the univariate logistic regression analysis, the variables with p < .05 were selected to be included in the multivariate logistic regression. Next, all the predictors were entered at once to test the associations when all variables are working together (Model 1). Model 1 tests the relationship of the predictors to each other and the outcome variable. After that, multiple regression with a stepwise logistic regression model was conducted to identify redundant variables in the multivariate modeling (Model 2). In Model 2, the regression is done many times, each time removing the weakest correlated variable. At the end, the remaining variables are those that explain the relationship best. Significance level was set at .05. All statistical analyses were performed using STATA 15.1 (StataCorp, College Station, TX).
Results
Sample characteristics of study participants and the proportion of each characteristic within the successful and unsuccessful groups are shown in Table 2. Forty-one percent of those who did not successfully complete had a history of neglect compared with 14.9 percent of those who successfully completed (p = .006). The groups had no differences in documented history of referral to Child Protective Services (CPS); 43 percent of participants who were not successful, however, had a history of removal from the home by CPS, compared with 22.9 percent of those who successfully completed the program (p = .032). Participants who were unsuccessful also had larger numbers of previous charges (p = .005), obtained more new charges during the program (p = .003), and had a higher rate of probation violations (p = .005).
Sample Characteristics by Disposition
As shown in Table 3, total SAVRY risk scores and total subcategory risk scores (historical, social, and individual) were high for both groups and protective category scores were low for both groups. Because these scores did not indicate any significant differences between groups, total and subcategory scores were not included in the model for further analysis. Individual SAVRY risk factors within these subcategories also indicated no significant differences between the two groups. Both groups demonstrated high rates of poor school achievement and social/contextual factors such as stress and poor coping, lack of personal/social support, and community disorganization. In addition, highly-reported individual risk factors for both groups included risk taking/impulsivity, anger management problems, and attention deficit/hyperactivity symptoms. As shown in Table 4, one protective factor, positive attitude toward intervention, was found to be significantly positively associated with successful completion of the program (p = .008).
Comparison of SAVRY Total Scores by Disposition
Comparison of Individual SAVRY Protective Factors by Disposition
Table 5 shows the unadjusted and adjusted odds ratios with their corresponding 95 percent confidence interval and p values. In the initial multivariate regression model (Model 1), only the number of previous charges was found to be significantly associated with the outcome variable (successful completion). Each additional previous charge significantly decreased the odds of successful completion (aOR: .68, 95% CI .50–.91, p = .011). In Model 2, being a victim of neglect and number of previous charges were found to be significantly associated with lack of successful completion. For victims of neglect, the odds of successful completion were significantly lower (aOR: .32, 95% CI .11–.93, p = .037). In Model 2, new charges during the program approached significance demonstrating lower odds of successful completion (aOR: .4, 95% CI .16–.99, p = .050). We identified the best multivariate model by comparing the Akaike information criterion28 (AIC) of the models. In AIC comparison, a lower value indicates the better model. We found that Model 2, with AIC = 122.28, df = 4, was more efficient compared with Model 1, with AIC = 122.69, df = 7, and best explains the relationship.
Odds Ratios by Successful Disposition
Limitations
The main limitation of our study is the nonstandardized nature of the case file data. The initial information was gathered by multiple providers and staff in narrative form, which was subsequently interpreted and categorized by the research team. Any conflicting information present was coded by researcher judgment. For parental factors, the court typically collected the characteristics of adoptive parents rather than those of biological parents. The files contained only scattered references to biological parents, so the variables are more consistent with environmental influences than biological. Information that was not present in the file was coded as negative, which likely resulted in under reporting of some variables. A significant limitation of this study was the inability to capture the hours of interaction between the assigned probation officer and the youth and their families or the impact of those relationships. These relationships were highly individualized as was the response to probation violations and new charges. Additional sanctions and removal to state custody often came down to a collaborative decision between the juvenile court judge and the assigned probation officer.
Discussion
The rate of successful completion in this study (48.5%) was comparable with the 46 percent successful completion rate in the juvenile drug court study.25 Also as in that study, we found that a history of neglect, removal from the home, and a higher number of previous charges were associated with lack of successful completion of the program and eventual removal to state custody. These are static risk factors that may correlate with less familial support and supervision and may indicate the need for targeted interventions with increased intensity of family support and engagement at the outset of JMHC involvement. Having new charges or probation violations during JMHC were significant risk factors for court failure that might be modified with increased family engagement and supervision. Having a positive attitude toward intervention correlated with successful completion of the program and could also be a target for modification during the probation period for both the family support system and the youth. Having a caregiver who is unable to engage in the requirements of a JMHC and unable or limited in ability to promote and support youth attendance and engagement in treatment may lessen a youth's positive attitude toward intervention and lessen engagement in therapeutic aspects of the diversion court. In addition, prior involvement in the court system without a treatment focus (such as exists in the JMHC) may bias the caregiver and child against a positive attitude toward intervention through a justice-sponsored mechanism.
Previous involvement with mental health treatment was not correlated with rates of program completion. Youth involved in the JMHC had significant history of prior inpatient and outpatient psychiatric treatment. Standard treatment for these high-risk youth may not be protective against involvement with the juvenile justice system. Files in this study indicated less frequent, but still considerable, physical (35%) or sexual (40%) assault history than previous studies of justice-involved youth. Yet more than two-thirds of participants had a history of referral to child protective services. These youth would likely have been candidates for trauma-related services and would have benefited from trauma-informed care earlier in their lives.
The measures that the jurisdiction in our study and other systems relied on for prediction of successful completion were not found to effectively predict program disposition. The Title IV-E form, which was used in the jurisdiction in our study to predict risk of removal to state secure facilities, was not predictive of success or failure in the program. The Title IV-E is a foster care eligibility form evaluating risk of removal from home, and a large number of youth in this study, whether they successfully completed or not, screened positive on this form. The process for determining eligibility for foster care changed in the state, and thus the Title IV-E form is no longer in use.
The SAVRY measure also did not reveal any relationship between its listed risk factors and participants' successful completion of the program or violent behaviors during the program. Similarly, the predictive value was limited because the majority of the youth involved in this study screened as high risk. It is also likely that while the SAVRY is a validated measure to predict future violence, it may not predict recidivism or violence after intervention.
Future studies could look more closely at type, duration, and compliance with evidence-based mental health treatments and any correlation with positive attitude toward intervention and successful completion of a youth diversion program. Future study should attempt to correlate a history of violent charges or novel violent charges while involved in a JMHC with initial SAVRY scores and with successful completion of the JMHC to better elucidate the role of the SAVRY instrument in the JMHC. Educational data obtained in this study also indicate opportunities for screening and early intervention. More than two thirds of the participants in this study repeated a grade in school, but fewer than half were receiving special education services. Truancy was also a common occurrence for youth involved in this JMHC. The school setting may be the ideal location for early mental health screening and to assure that those students who have a pattern of truancy or grade failures are screened for mental health distress and need for special education services.
Juvenile Mental Health Courts are an increasingly popular method for linking justice-involved youth with mental health services and deserve more study to identify the most effective application and greatest chance of success for our most vulnerable youth. Once youth are involved in a diversion or probation program, implementing a wrap-around services approach (including support for family and home life, educational supports, and linkage with community-based supports and interventions) may improve positive attitude toward intervention and lessen the opportunity for new charges and probation violations, which could correlate with improved rates of successful completion of a JMHC program and reduced recidivism.
Acknowledgments
This study was supported in part by the TTUHSC Clinical Research Institute with statistical analysis by Eneko Larumbe, PhD, and Rohali Keesari, MPH, at the TTUHSC Clinical Research Institute.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2023 American Academy of Psychiatry and the Law





{kind=link}