


Abstract
Civil commitment is a legal process in which persons may be involuntarily detained for psychiatric evaluation and treatment if, because of mental illness, they are at imminent risk of harming themselves or others. Procedures that protect such persons from undue infringements of their personal liberties vary by state. Some jurisdictions permit individuals to waive their right to contest a hearing and instead stipulate to civil commitment. This differs from voluntary hospitalization in that the individuals accede to treatment for the term of commitment and forgo the possibility of either subsequent voluntary consent or withdrawal of consent. The authors describe a 50-state review examining whether statutory law permits these waivers. We show that many states allow a waiver but do not require that the person have decision-making capacity. Capacity assessment is essential because persons with impaired decision-making may accept a commitment that might otherwise have been successfully challenged, and commitment can have unwanted consequences, including extended hospitalization, loss of rights, and stigma. We propose procedures and criteria for assessing capacity to stipulate that include not only understanding that stipulation will result in commitment but also understanding the nature, purposes, consequences, and processes involved in commitment.
Civil commitment is a legal process in which a person with mental illness may be involuntarily detained for mental health evaluation and treatment if, as a result of the mental illness, the person is at imminent risk of causing harm to self or others.1 Civil commitment has a long tradition in Anglo-American jurisprudence and stems from the state's dual obligations to protect vulnerable individuals who cannot adequately care for themselves and to shield the community from possible danger.2 Although civil commitment has noble aspirations, historical abuses and an increasing emphasis on patients' rights have given rise to procedural protections from unjust or undue infringements of the personal liberties of persons with mental illness.3 The U.S. Supreme Court has established that states must prove by at least clear and convincing evidence in an adversarial civil proceeding that a person satisfies commitment criteria.3 A successful commitment petition results in a judicial order authorizing clinicians to provide involuntary treatment in a psychiatric unit that may extend into the outpatient setting if outpatient commitment is also ordered. An unsuccessful commitment petition, meanwhile, results in the person's release from detention. In addition, persons facing civil commitment can interrupt the process if they consent to voluntary treatment. Voluntary consent requires that persons convey a desire to remain hospitalized and that they understand: that they are admitted to a psychiatric unit for the purpose of treatment, that the hospital may choose not to release them upon their request, and that staff may help them initiate the procedures for release.4 This definition is termed “assent” in some contexts in recognition of the lower standard of decisional abilities it requires, compared with other health care decisions.4 Individuals who consent to psychiatric hospitalization may later withdraw their consent and oblige their treatment team either to discharge them or to reinstate civil commitment proceedings.
Although federal courts have declared minimum procedural requirements, states still have substantial leeway in the implementation of civil commitment hearings. One way that procedures can vary is whether or not the state permits individuals to waive their right to contest a court hearing and instead stipulate to civil commitment. Stipulation to civil commitment differs in important ways from voluntary consent to psychiatric hospitalization in terms of both process and outcome. A person who gives voluntary consent preempts the civil commitment process while leaving open the possibility of subsequent withdrawal of consent. No court order is issued, and no term of inpatient or outpatient commitment extending beyond the immediate hospitalization is specified. In contrast, a stipulation advances the court proceeding. A hearing often is still held, though it may be perfunctory or abbreviated in nature without presentation of testimony or evidence. The hearing results in the issuance of a court order for commitment. For the remainder of the commitment, the patient does not have the option to consent or withdraw consent.
In states that rely exclusively on inpatient commitment that ends upon a person's discharge from the unit, the chief distinction between voluntary inpatient treatment and stipulated inpatient commitment is the removal of the option to withdraw consent. A voluntary inpatient can later request to be discharged against medical advice (AMA). The treatment team must then decide whether to permit the AMA discharge or reinitiate the civil commitment process from the beginning. Patients who have stipulated to commitment have no such choice. They must remain for the duration of the commitment, which is usually determined by the treatment team's assessment of the patient's need for treatment or until the commitment order expires.
In states whose commitment laws permit subsequent episodes of care beyond the immediate hospitalization, such as outpatient commitment, stipulation can have profound effects even after a person is released from the hospital. Patients may be subject to ongoing monitoring and may be required to engage in outpatient treatment and adhere to treatment recommendations like psychotropic medications. Persons who do not cooperate may be apprehended and rehospitalized without having another judicial hearing.
In our experience in Arizona, for example, patients who stipulate to commitment often fall into one of two categories. Some patients are acutely ill when first brought into a psychiatric unit under a petition for civil commitment but nevertheless cooperate with treatment and begin to recover by the time the commitment hearing is scheduled. Rather than agreeing to voluntary status, which would terminate the commitment proceedings and cancel the hearing, they choose to stipulate to a year of combined inpatient/outpatient commitment at the court hearing and obtain a judicial order for treatment. This order serves as a fallback if their condition deteriorates in the future and they lose insight or cease adherence to treatment. With the commitment order in place, treatment providers can rapidly rehospitalize and restabilize the patient even before the patient decompensates to the point of dangerousness.
A second group of patients chooses to stipulate to involuntary commitment because they believe (often erroneously) that stipulation is the most expedient method of securing their release from the hospital. These patients may dispute that they have a mental illness or need psychiatric treatment, and they misunderstand the nature and purpose of commitment or stipulation to commitment. Such individuals in Arizona may be prevented from stipulating to commitment if they cannot demonstrate a proper understanding of the consequences of their decision; this results in a full commitment hearing.
To summarize, there are several paths through which civil commitment can be resolved, and these different paths are presented as a flowchart in Figure 1. The patient can engage in voluntary treatment, terminate commitment proceedings, and be discharged at the conclusion of voluntary treatment. For patients who choose to leave AMA and still meet commitment criteria, the treatment team can reinitiate commitment. Depending on jurisdiction and timing, the initial emergency hold may still be in effect, or a new emergency hold may need to be issued. Patients who sign out AMA but are no longer appropriate for commitment may be discharged. Depending on whether a suitable discharge plan can be arranged prior to the patient's exit from the hospital, the team may perform a standard discharge or an AMA discharge.
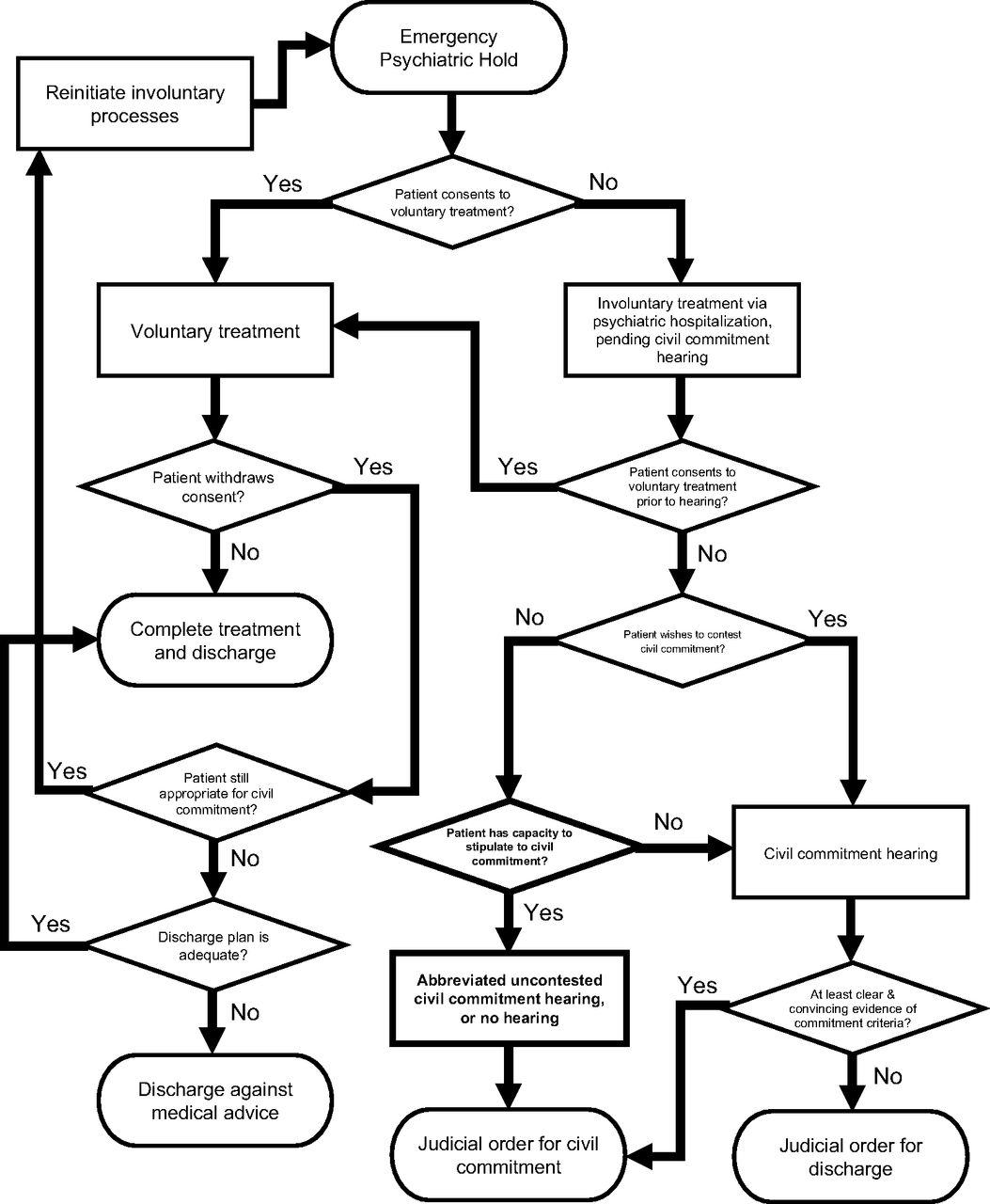
Paths through civil commitment and voluntary treatment.
Alternatively, for patients who do not or cannot consent to voluntary treatment, a court hearing is held to determine whether they meet commitment criteria. Voluntary treatment remains an option up until the court hearing occurs. In states that allow stipulated commitments, the patient must decide whether to contest the commitment. If a patient does not contest the commitment, the judge issues an order for commitment, with either no hearing or an abbreviated, perfunctory hearing. If the patient does contest the commitment (or lacks the capacity to stipulate in the states that require capacity), the state must present at least clear and convincing evidence that the patient meets commitment criteria. If the state is successful, the judicial order for commitment is issued. If the state is unable to meet its burden of proof, the judge orders the patient's discharge.
Stipulations to civil commitment can be abused if an individual lacks the capacity to make such a decision or is poorly informed about the ramifications of the decision. Persons participating in civil commitment proceedings may be experiencing acute serious mental illness that can affect their decisional abilities and understanding of the commitment process and its consequences. Concerns about abuse and inappropriate waivers or stipulations are not merely theoretical. For instance, in A.A. v. Eskenazi, a patient sued an Indiana community mental health agency after his right to appear in his commitment hearing was improperly waived.5 In that case, the patient's attorney waived his right to appear after being informed that the patient was agitated, without ever meeting the patient. The court accepted that this was the patient's decision and the hearing proceeded in his absence, resulting in involuntary civil commitment. Indiana's state code permits such waivers and does not expressly require that the waiver be competent. Subsequently, the Indiana Supreme Court vacated the commitment order, holding that personal waivers of hearing appearance must be knowing, intelligent, and voluntary, and be executed by the respondent rather than the attorney by proxy.5 Despite this ruling, the relevant sections of Indiana's statutes remain unchanged.6
Although civil commitment has a substantial effect on an individual's liberty and treatment, and robust procedures are important to protect vulnerable populations, scholars thus far have paid scant attention to civil commitment hearing waivers and stipulations. In this article, we investigate the extent to which states permit individuals to waive their right to a hearing or stipulate to civil commitment. We focus on adult commitment, as juvenile commitment may have additional considerations. To our knowledge, this is the first article of its kind, and we are aware of no published data or studies documenting the prevalence, effects, or other characteristics of this practice. The authors can attest anecdotally that waivers or stipulations occur with regularity in at least some states, resulting in patients' being committed for up to months at a time. To better understand the practical significance of waivers and stipulations, we also informally queried the National Association of State Mental Health Program Directors (NASMHPD) Forensic Division listserv about civil commitment practices. Respondents indicated that waivers or stipulations have occurred in Alabama, Arizona, Arkansas, Colorado, Georgia, Illinois, Missouri, Mississippi, Ohio, Rhode Island, Tennessee, Utah, Vermont, and Wisconsin.
We begin with a brief overview and history of civil commitment in the United States. We then present a comprehensive survey of commitment statutes in the 50 states, focusing on language concerning waivers and stipulations. We show that most states permit detainees to waive their right to a commitment hearing or stipulate to the commitment. Yet, most of those states do not articulate a requirement that the person waiving their rights must be competent to do so. In the few states that do delineate such a requirement, the methods and substantive criteria for determining such competence are absent. We argue that whenever someone seeks to waive the right to a civil commitment hearing or stipulate to commitment, there should also be a determination that the person has the decision-making capacity to do so. We describe a process by which capacity assessment can be integrated into the commitment and stipulation procedures and propose a set of substantive criteria that capacity evaluators should consider when determining whether someone is competent to consent to stipulation. This additional procedural protection can safeguard against the risk of unjust commitments.
Civil Commitment
In the United States, civil commitment is a process by which a judge or judicial authority may order that an individual with symptoms of mental illness who meets specific criteria be involuntarily hospitalized or receive supervised outpatient treatment for a specific period of time. The requirement for due process protections and a judicial order confers a greater degree of protection from liability for the hospital confining the patient. Every state has its own laws that govern the local standards and procedures for this process.7 Regardless of the state, commitment proceedings must provide for due process protections under state and federal law; for example, a qualified right to refuse treatment and the general right of law-abiding persons not to be confined unless they pose some risk of harm.8 As a result, the specific clinical criteria that must be met to qualify for civil commitment typically relate to safety concerns: either that the person poses an imminent risk of harm to self or others or cannot sufficiently attend to basic needs for food, clothing, shelter, or safety. Being civilly committed can affect other individual rights beyond the mere act of confinement and its infringement on bodily freedom. For example, federal and certain state laws limit the right of a previously committed individual to possess firearms.9,10
The history of involuntary psychiatric hospitalization in the United States is long and complicated. Explicating the full extent of this history is beyond the authors' intended scope, but a brief review of the principles that shifted this landscape is important for the theoretical understanding of contemporary civil commitment. Prior to the 1800s, individuals with mental illness were typically relegated to prisons and shelters.11 In the 1800s, private and publicly-funded mental institutions (also known as asylums) were developed and became the primary means for treating individuals with severe illness. At that time, the standard for civil commitment required only the presence of a mental illness and that there was a recommendation for inpatient psychiatric treatment.12 The standards for civil commitment shifted to a focus on dangerousness in the 1960s with Congress' enactment of the Ervin Act,13 which was furthered in the 1970s in Lessard v. Schmidt.14 These were important not only for shifting commitment standards but also for recognizing alternatives to hospitalization as a potential treatment option.8 Later in the decade, the California legislature took an additional step forward by requiring that commitment be based on either dangerousness or grave disability (i.e., the inability to care for oneself) and was the first state to use such criteria.15
Two 1970s U.S. Supreme Court cases took additional steps forward in solidifying the legal expectations regarding civil commitment proceedings. In the 1975 case of O'Connor v. Donaldson,16 the Court emphasized the requirement for dangerousness as the foundation of civil commitment, holding that “a State cannot constitutionally confine, without more, a nondangerous individual who is capable of surviving safely in freedom by himself or with the help of willing and responsible family members or friends” (Ref. 17, p 573).16 In 1978, the Court articulated in Addington v. Texas17 that the applicable standard of proof required in civil commitment proceedings is a clear and convincing evidence standard.
Current civil commitment requirements in the majority of states share many common components.8 All states require the presence of a mental illness for an individual to be civilly committed. Statutes vary in their specific terminology but usually define mental illness in a manner that infers the expectation that the individual is given a diagnosis of a serious and persistent mental illness. In virtually all states, dangerousness to self or others is an explicit criterion, and in most states grave disability is also included as an alternative to dangerousness. The need for treatment is included in nearly every state, either explicitly as its own criterion or as a component of the statute's definition of mental illness (e.g., a mental condition requiring treatment). A smaller number of states describe the expectation that the individual is experiencing a “deterioration,” either separately or as a component of the grave disability definition. The individual's competence to make decisions is also referenced in some states. In addition, virtually all states incorporate consideration of the least restrictive alternative in their commitment statutes.18 This requires an assertion from the party seeking commitment that the individual's needs cannot be sufficiently met in a less restrictive setting or manner than the one recommended.
An important outgrowth of inpatient civil commitment laws has been the development of involuntary outpatient commitment (IOC; also known as assisted outpatient treatment or AOT). The American Psychiatric Association's Resource Document on IOC describes it as “a form of court-ordered outpatient treatment for patients with severe mental illness and who are unlikely to adhere to treatment without such a program. It can be used as a transition from involuntary hospitalization, an alternative to involuntary hospitalization or as a preventive treatment for those who do not currently meet criteria for involuntary hospitalization” (Ref. 19, p 1). In 2015, the American Psychiatric Association issued a position statement in support of the use of IOC as a tool to enhance treatment adherence, reduce relapse and re-hospitalization, and decrease the risk of dangerous behavior for a sub-group of individuals with severe mental illness.20 The use of IOC has frequently been criticized for its over-representation of under-represented minority populations.19 While statutes enabling its use have been established in 45 states, a 2016 survey found that it was effectively utilized in fewer than half of those states with its uneven implementation reflective of the judicial and mental health communities' ambivalence about its role and scope and that the cost of effective implementation cannot be borne by most state budgets.21
State civil commitment regimes share common ethics and legal principles, standards, and procedures, but specific implementation can vary widely. One such variation that can have significant impact on patients is the practice of allowing individuals to stipulate to commitment or waive their right to a judicial hearing. Civil commitment standards and procedures are intended to strike a fair balance between individual rights and state interests, and waivers of procedural protections have the potential to upset that balance.17 These concerns are especially acute for persons with serious mental illness whose decisional abilities may be impaired and who consequently may lack the capacity to enter into a competent waiver or stipulation. We examined state statutes concerning waivers and stipulations to investigate how widespread these practices are and whether capacity or competence is a required element of the waiver or stipulation.
50 State Review of the Capacity to Stipulate
Methods
Statutes outlining hearing procedures for involuntary civil commitment from all 50 states were reviewed. A preliminary inquiry of civil commitment state practices was conducted in December 2020 by querying the National Association of State Mental Health Program Directors (NASMHPD) Forensic Division listserv. The Treatment Advocacy Center website, which maintains a list of state commitment statutes, was used to determine the criteria for inpatient commitment for each state and whether these state laws were applicable to outpatient commitment (IOC or AOT).7,21 A separate inquiry was conducted by keyword searches in the Lexis+TM and Justia websites (online legal research databases). The keywords searched were “involuntary commitment in [insert state],” “psychiatric commitment in [insert state],” and “mental health commitment laws in [insert state].” The relevant statutes were cross-referenced with the results of the NASMHPD query results, as well as the published statute on the Justia website. After the pertinent statutes were procured, the language was reviewed to categorize a state's legal stance toward assessment of capacity as a prerequisite to stipulating to commitment or waiving appearance at the commitment hearing. The online searches and subsequent review of statutes occurred between March 29, 2021 and August 3, 2021.
The explicit language contained in the state's code may not provide a comprehensive understanding of the state's approach to civil commitment. Because statutes on civil commitment are further qualified by case law, court rules, legal manuals, patient bills of rights, legislation on psychiatric advanced directives, regulatory bodies, common practices, and other considerations, a review of case law using Lexis+TM or the state's Court Rules were completed to determine the state's court hearing procedures in instances in which the statutory language was ambiguous. To corroborate the findings of the initial search, a second survey was done utilizing Lexis+TM, Justia, and individual state legislative websites. A state's stance toward the respondent's presence at the hearing(s) or waiver of the respondent's right to a commitment hearing and stipulation to commitment were determined and categorized using a strict interpretation of the state's legislation. The designated categories were:
Respondent, who is capable of making a knowing or intelligent waiver of appearance, may stipulate to commitment or to the court's hearing decision;
Respondent can waive appearance and stipulate to commitment or concede to the findings of the commitment procedure, without explicit reference to respondent's capacity to make a knowing or intelligent waiver;
Respondent's attorney/representative or judge/court can waive respondent's appearance at the hearing; however, the hearing may continue in the respondent's absence;
Involuntary commitment may occur on the basis of physician certificate with no requisite hearing involving respondent; or
There was a dearth of language addressing hearing policy or procedures and capacity to stipulate to commitment or waive respondent appearance.
Results
Ten of the 50 states (AK, DE, HI, LA, MS, MT, NE, NH, NM, and UT) have statutes which reference the need for a knowing and intelligent waiver, informed consent, or capacity assessment prior to stipulating to inpatient commitment, waiving hearing appearance, or conceding to the hearing findings (Fig. 2, see online Appendix for additional details). Fifteen states (AZ, CA, GA, MA, MI, MN, ND, OH, RI, SC, SD, TN, TX, WI, and WY) have legislation allowing respondents to waive appearance, stipulate to commitment, or concede to the court's hearing decision without explicit reference to their capacity or competence to execute a knowing and intelligent waiver. Of note, codes in Tennessee and Wisconsin enable waiver of hearing appearance with the respondent's “consent.” While this may imply competent or informed consent, it could also be more loosely interpreted as general consent or even assent. Similarly, Minnesota permits waiver of hearing appearance if the waiver was “freely given.” While voluntariness is a necessary component of informed consent, it does not wholly equate to having competence to make such a decision.
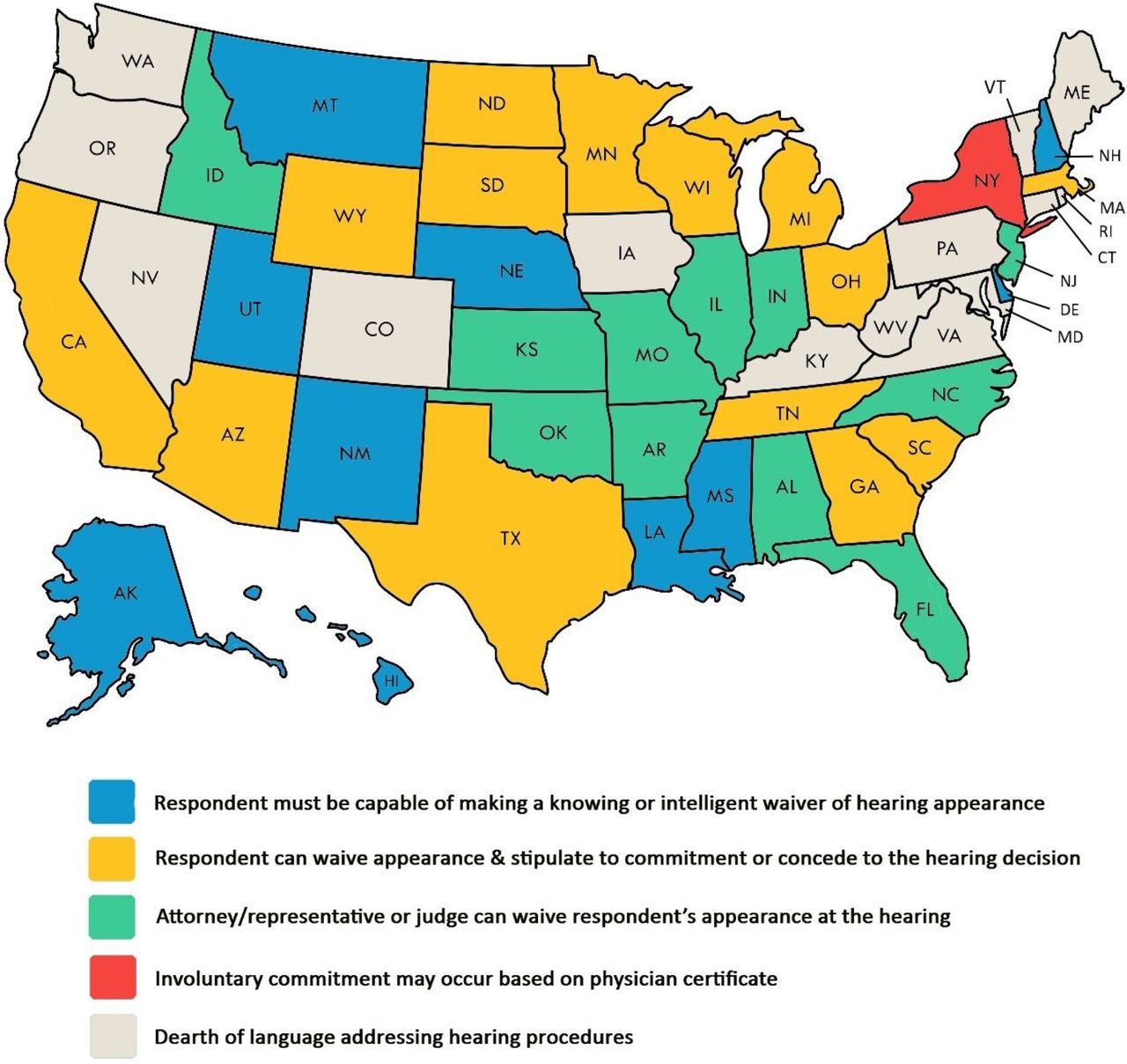
State statutes regarding inpatient civil commitment.
In 11 states (AL, AR, FL, ID, IL, IN, KS, MO, NC, NJ, and OK), the hearing on inpatient commitment can be waived by the judge or trial court or the respondent's representative or attorney, and the hearing can be conducted in the respondent's absence. New York is unique in that involuntary commitment can occur based only on a two-physician certification without a required judicial hearing. After admission, the respondent may petition for a hearing on the inpatient commitment, but no hearing occurs in the absence of the respondent's proactive request. Finally, 13 states (CO, CT, IA, KY, MD, ME, NV, OR, PA, VA, VT, WA, and WV) have statutes that are devoid of language addressing their hearing procedures or respondents' capacity or competence to stipulate to involuntary commitment or waive hearing appearance.
Respondents to the informal NASMHPD survey indicated that waivers or stipulations to civil commitment do in fact occur in states across these four categories. Mississippi and Utah represent states that require a competent waiver or stipulation. Arizona, Georgia, Ohio, Rhode Island, Tennessee, and Wisconsin represent states that permit a waiver or stipulation but do not explicitly require that it be competent. Alabama, Arkansas, Illinois, and Missouri represent states that permit persons other than the patient to waive or stipulate. Finally, Colorado and Vermont represent states whose statutes do not address this topic.
In states that permit outpatient civil commitment, the statutory language concerning capacity or competence to waive the hearing or stipulate to commitment in inpatient settings was applicable to, or mirrored in, their outpatient commitment statutes, with few exceptions. North Carolina allows respondents to waive their right to appear at their inpatient commitment hearing but requires their presence, enforceable by subpoena, for outpatient commitment. Meanwhile, Hawaii, Louisiana, and New Mexico permit inpatients to waive their hearing, but outpatient commitment hearings may occur in the absence of the patient, whether or not the patient explicitly waives the right to appear. In New York, inpatient commitment can proceed with a two-physician certification and no judicial hearing, but outpatient commitment requires a hearing, which may go forward in the absence of the patient. Three states, Connecticut, Maryland, and Massachusetts, have no laws permitting outpatient commitment.
Discussion
Of the 36 states that explicitly permit waivers or stipulations, only ten require that the patient be competent. In fact, more states (11) allow someone other than the patient to waive the patient's rights, while thirteen do not address waivers or stipulations at all. In short, there is a great deal of variation among states concerning a patient waiving the right to a hearing or stipulating to commitment, and competence to waive or stipulate is required in a mere handful of states. The language, moreover, may often be conflicting or ambiguous, which allows interpretation and procedures based on local practice, court administrative rules, and legal precedents. This lack of clarity is inconsistent with fundamental principles of law, medicine, and ethics. Further research is needed to quantify the extent to which waivers and stipulations occur and their effects on individuals progressing through the civil commitment process.
The notion that individuals are autonomous agents capable of deciding the course of their lives and bearing the responsibility for the consequences of their decisions is a foundational concept.22 Depending on the context, a person who possesses the mental and decisional abilities needed to make autonomous decisions is said to be competent or have decision-making capacity.23 In broad conceptual terms, competence or capacity typically requires that a person can understand, both generally and personally, the nature of the relevant decision and the consequences the decision carries. The person must also employ a reasonable thought process in arriving at the decision and be able to convey that choice to others. Individuals who have attained the age of majority are generally presumed to be competent, though this presumption can be challenged when decisional abilities appear to be impaired in some way.23 In health care settings, the Four Abilities model of decision-making capacity formalizes these criteria as understanding, appreciation, reasoning, and choice.24 Related concepts in other spheres require similar decisional abilities, though they differ in the types of decisions, relevant knowledge, and terms used. For instance, the factual understanding a defendant must demonstrate to be competent to stand trial in a criminal case corresponds to understanding, while rational understanding roughly maps onto appreciation and reasoning.25 Similarly, in assessments of testamentary capacity, evaluators must determine that the testator understands and appreciates the nature of a will, the extent of the relevant assets, the potential beneficiaries of those assets, and the consequences of distributing the estate. The testator must also be able to articulate a rationale that is free of disordered thinking.26
Requirements that a person be competent or capable protect vulnerable persons from behaving in ways that are contrary to their autonomous desires. When life, liberty, or significant amounts of property are at stake, society has a duty to assure that people are not compromised in their ability to make decisions.
Waiving a civil commitment hearing or stipulating to commitment is a decision that can have considerable effects on a person's health, liberty, and prospects. Although the initial emergency psychiatric hold may already be highly disruptive, advancement to civil commitment can significantly lengthen or intensify the effects of involuntary treatment. People who are civilly committed give up a number of important rights. Inpatients are detained in a psychiatric unit; under certain circumstances or with additional legal authorization, they may also be given medications over objection.27 Outpatients are required to attend mandatory appointments and accept medication to remain in the community.28 Treatments, including not only psychotropic medications but also psychosocial and milieu interventions common on psychiatric units, may have unwanted or adverse effects on mental or physical health.29 Committed individuals also lose the ability to own firearms based on federal law.9,10,30 A history of commitment and psychiatric treatment can be stigmatizing.31
Thus, as with health care, criminal proceedings, and wills, it is critical that decision-making capacity be assessed when a person wishes to waive the right to a commitment hearing. Fortunately, mental health professionals are well-positioned to make this determination during the civil commitment proceedings. Psychiatric clinicians are intimately involved in the civil commitment process as treating clinicians, initiators of the commitment, or court-appointed evaluators of the need for commitment. Thus, it would be relatively straightforward to fold the assessment of capacity to waive a commitment hearing or stipulate to commitment into the assessment of whether the person meets commitment criteria in the first place. Once the person expresses the wish to waive the hearing or stipulate to commitment, the clinician responsible for assessing eligibility for commitment could set up an additional meeting to ascertain whether the proposed waiver is competent. This additional assessment would also provide an opportunity for the evaluator to disclose or remind the patient of the consequences of the waiver, so that any such choice is made with proper information.
The next question is how an evaluator should determine whether a waiver is competent or the person has the relevant decision-making capacity. During a civil commitment hearing, a state must prove by at least clear and convincing evidence that a person, as a result of mental illness, poses a danger to self or others or is unable to provide basic self-care (grave disability). If the state is unsuccessful, the person is released from involuntary detention. A person who is committed will be detained in a psychiatric unit and provided mental health treatment for a specified period of time. Once a commitment is in place, states typically provide a mechanism to review or overturn the commitment at a later date.
Thus, we propose the following substantive criteria, keeping in mind the conceptual basis for competence and capacity, as well as the particular concerns at stake in commitment. Persons who are waiving their right to hearing or stipulating to their civil commitment should be able to understand and appreciate that:
They are giving up their right to a hearing, in which the state must prove that they have a mental illness and that they pose a danger to themselves or others or are gravely disabled.
They are not required to waive this right.
If there were a hearing, there would be a possibility that the state would fail to prove the necessary facts, and they would be released.
Without the hearing, the commitment will go forward.
They will be committed for the duration specified in statute. This would involve some combination of confinement in a psychiatric unit (for inpatient commitment) or a requirement that they adhere to outpatient psychiatric treatment, with consequences for failing to adhere to such treatment (for outpatient commitment).
Commitment is for the purpose of receiving mental health treatment for a presumed mental illness.
They have the right to request a review or challenge the commitment after it is put in place at statutorily defined intervals.
In addition, persons should be able to discuss their waiver using a rational thought process. Assessing these criteria will ensure that persons entering into a waiver do so with a full knowledge of the nature of the hearing and alleged facts and of the consequences of the waiver.
Conclusion
Civil commitment allows states to provide treatment for people with serious mental illnesses who may pose a danger to themselves or others or who are so debilitated that they cannot adequately care for themselves. The benefits must be weighed against the restrictions placed on people's autonomy. Commitment statutes and case law have established procedures to provide appropriate care while also mitigating against unjust deprivation of liberty, but these procedures can be circumvented when individuals waive their right to a hearing or stipulate to commitment. As we have shown, most states currently do not require waivers and stipulations to be competent, and this oversight can be detrimental to people whose decision-making capacity is impaired. Procedural protections must be extended so that when people waive their rights, they do so competently. A modification of current evaluation practices, in which commitment evaluators also assess competence to waive or stipulate when the situation arises, can address this gap and ensure that civil commitment continues to strike the proper balance between liberty and welfare.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2023 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}