


Abstract
Individuals with a history of offending behavior show high rates of mental disorder as well as fetal alcohol spectrum disorder (FASD). Neurocognitive impairments are common in both mental disorders and FASD and may interface with offending behavior. Understanding these impairments could effectively inform clinical considerations among this population. The purpose of this study was to characterize the life experiences and examine the neurocognitive profile of a group of adult forensic psychiatric outpatients. We also investigated potential differences between offenders with FASD and the rest of the sample. Data were collected on 45 subjects on numerous variables, including demographics, background information, offending histories, and comorbidities. Subjects also completed extensive neurocognitive testing. The sample was primarily male (82.2%) with a mean age of 42 years. There was a high prevalence of lifetime adversity and varied offense histories. Subjects showed the most significant neurocognitive impairment in executive function, visual memory (immediate and delayed recall), and full-scale IQ. The FASD group (n = 12) did not differ significantly from the No-FASD group (n = 33) on any background variables. The FASD group showed significantly lower neurocognitive scores in the areas of verbal IQ, full-scale IQ, working memory, processing speed, and expressive vocabulary.
The rates of mental disorders within offending populations are high, and current evidence shows that they are increasing. For instance, an international meta-regression analysis that collated a population of 33,588 prisoners from 24 different countries reported that “high levels of psychiatric morbidity are consistently reported in prisoners from many countries over four decades” (Ref. 1, p 394). In other studies, 41 percent of all inmates (and up to 73% of incoming male offenders) presented with at least one severe symptom of mental disorder.1,2 Researchers have also reported that, between 1967 and 2004, the number of offenders with mental disorders (OMDs) admitted to federal institutions in Canada increased by 60 percent,3 and the increase was even greater when substance use disorders were included (84%).3,4 It is possible that improved awareness of mental health concerns and greater access to psychiatric diagnostic services have contributed to the increased rates. Implicit in these high rates of mental disorders among incarcerated individuals is the expectation that psychiatric health will also be a significant concern for offenders released into community support settings. Therefore, understanding the unique characteristics of OMDs is important for providing efficacious support for these individuals in correctional and forensic outpatient settings as they reintegrate into the community.
OMDs appear to experience an increased susceptibility to negative institutional, health, and criminal outcomes compared with offenders without mental disorders. Challenges in adjustment and victimization within institutions have been reported in this group, which can further perpetuate mental health symptoms during incarceration.5 Upon release from correctional settings, OMDs are at risk for psychiatric rehospitalization or criminal recidivism because of numerous transitional difficulties and a lack of reintegration support.6,7 Parolees with mental disorders are about twice as likely to return to prison within one year as parolees with no mental disorders.7 These challenges underscore the importance of finding means to understand and better support this group of individuals to improve their criminal justice and psychosocial outcomes, and for the safety of the communities in which they live.
The specific contributors to negative outcomes for OMDs have not been studied sufficiently, but researchers have advocated for early screening programs that identify OMDs and assess their needs for interventions in the criminal justice process.8 By understanding the intersection of mental disorder with offending, as well as utilizing proactive case management to create community-based treatment plans, the needs of offenders could be more suitably met. Innovative and comprehensive treatment coupled with diversionary measures have also been recommended for OMDs to provide more appropriate services, which may ultimately improve readjustment to the community and address recidivism.9 This, in turn, could improve compliance with public safety mandates.10
Neurocognitive Impairment
Current evidence points toward an interface between neurocognitive impairment and offending behaviors.11,–,13 Deficits in inhibition, executive function, set shifting, attentional disturbances, and memory have been tied to impulsive offending and violent behaviors.12,14,–,16 Neurocognitive profiles of offenders diagnosed with antisocial personality disorder17 and attention deficit hyperactivity disorder18 have been investigated previously. Existing studies, however, are often limited by focusing on institutionalized patients and using neuropsychological screening rather than extensive batteries of tests.19,20 Disorder-specific investigations have offered valuable insights for support and rehabilitation of offenders in these contexts. The neurocognitive profiles of individuals diagnosed with prenatal alcohol exposure (PAE) has been studied far less.
Fetal Alcohol Spectrum Disorder
In the most recent edition of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), an important update was the recognition of the etiological role of PAE in the development of mental and behavioral disorders.21 PAE has wide-ranging effects, including the potential to disrupt fetal development, which can produce adverse physical, cognitive, behavioral, and social outcomes.22 In Canada, fetal alcohol spectrum disorder (FASD) is a diagnostic term defining “a broader spectrum of presentations and disabilities resulting from alcohol exposure in utero.”23 Prevalence estimates are higher than originally thought, ranging from 1 to 5 percent of the general population.24,–,26
Several researchers have attempted to establish FASD prevalence within correctional settings, but the precise prevalence is still unknown. In one study, approximately 60 percent of adolescents and adults with FASD reported interface with the legal system, and 35 percent reported having been incarcerated for a crime.27 Others have indicated that youth with FASD are 19 times more likely to have trouble with the law compared with those without FASD.28 Experts believe that there is an even greater number of undiagnosed or misdiagnosed persons in both juvenile and adult correctional facilities who are affected by FASD.29,30 In one study, Fast and colleagues evaluated a sample of 287 remanded Canadian young offenders and determined that 23.3 percent had an alcohol-related disability, but only three (1%) of these youth had a prior diagnosis.29 More recently, Australian researchers reported that 36 percent of youth in a detention center were diagnosed with FASD.31 Canadian researchers found that 18 percent of adult offenders in a correctional facility met the diagnostic criteria for FASD.32 Justice involvement among individuals with FASD has a significant impact on the Canadian economy, reportedly accounting for the largest proportion (40%) of the total annual cost of FASD, outweighing health care (21%), education (17%), and social services (13%).33 Unfortunately, neither the justice system nor the postrelease community support structures are currently well-suited to support offenders with disabilities of any kind. Despite the over-representation and economic costs associated with FASD in the justice system, there are at present no evidence-based FASD-informed justice interventions or postrelease supports described in the literature.
Individuals with FASD tend to experience a range of neurocognitive challenges, including deficits in attention, set shifting and encoding, self-regulation, and metacognition.34,–,39 Among those with FASD in the criminal justice system, some researchers suggest that the functional consequences of various impairments (in working memory, planning, organizing, problem solving, integration of knowledge, linking consequences to actions, and impulse control) might affect potential offending behaviors and capacity to comply with postrelease expectations.40,41 Neurocognitive deficits in individuals with FASD may also relate to a heightened vulnerability for manipulation and alliance with deviant groups, potentially leading to a higher likelihood of getting involved with activities that may result in trouble with the law.42 Once involved in the justice system, offenders with FASD may also have difficulties comprehending the purposes and processes of legal proceedings.43 Researchers have described several FASD-related challenges that may be especially relevant to sentencing offenders with FASD, including difficulties linking punishment to crime, compromised ability to instruct counsel, risk of being taken advantage of in prisons, trouble with differentiating right from wrong, and risk of being influenced by someone else in committing the crime.44
Adding to the complexity of the disorder, individuals with FASD are reported to experience exceptionally high rates of mental health challenges. Researchers have reported that mental health problems are the most prevalent adverse outcome associated with FASD, with 94 percent of adolescents and adults affected by such difficulties.29 Although there is very little research to examine the relationship between mental health and criminality in FASD, several recent studies have suggested high rates of mental illness and addictions among offenders with FASD.45,46 Improved understanding of the intersection between mental disorders, neurocognitive impairment, FASD, and offending behaviors will advance the potential for responsive rehabilitation and help guide practical change for better supporting this group toward positive outcomes.
Study Purpose
There are very few studies of FASD or neurocognitive functioning in OMDs, and those that exist are limited to using screening tools rather than comprehensive assessment batteries. These types of studies are insufficient when the goal is to identify different domains of neurocognitive deficit that may be unique to individuals involved with the legal system. Research examining PAE and neurocognitive functioning among offenders is just emerging, and studies in outpatient settings are rare. Research in this setting is vital because outpatient treatment is one of the most common means of support for individuals transitioning to the community.
The broad purpose of this study was to characterize a group of outpatient OMDs with a special focus on neurocognitive functioning and FASD. To do so, we explored the characteristics and life experiences of outpatient OMDs, examined neurocognitive profiles among the OMDs, and investigated differences in life experiences and neurocognitive functioning between OMDs with and without FASD.
Methods
Recruitment
This research was approved by the Research Ethics Board of the University of Saskatchewan. The study sample was recruited from an outpatient forensic psychiatric clinic in Saskatchewan, Canada. Offenders were referred to this clinical setting through Probation Services, the Parole Board of Canada, by having been found not criminally responsible of a criminal offense or unfit to stand trial due to mental disorder, or because of previous trouble with the law requiring forensic psychiatric monitoring and management. Over the period of the study, the yearly count of the eligible active and inactive outpatients in the clinic was between 85 and 150 patients. All those who were active attendees of the clinic were consecutively approached for the study based on their attendance at the clinic. Inactive enrollees were not contacted. A nonclinical research coordinator approached eligible individuals regarding their interest in participating in the study and provided detailed information about the research before obtaining informed consent. A total of 79 subjects consented to the study. Over the course of the study, 34 subjects did not complete full data collection for multiple reasons, including moving away, losing interest, or not responding to attempts to contact. Acceptable data completion was reached with 45 subjects, and only those were included in the analyses.
Data Collection
Subjects completed a series of self-report questionnaires to provide data on demographics, background characteristics, and offense histories (provided by subjects and crosschecked with external sources where necessary). A research coordinator was present throughout the completion of all questionnaires to provide clarification and support as required.
A subset of subjects completed comprehensive psychological testing to assess functioning in several neurocognitive domains. Assessments were conducted by one of two registered psychologists with the assistance of one of two trained psychometrists. Neurocognitive functioning was assessed in six to eight domains that correspond with the areas of neurocognitive functioning tested in the assessment for FASD.47 The assessment battery varied slightly depending on which psychometrist conducted testing in accordance to the psychometrists' training and level of experience with specific tests for each domain represented. The number of tests completed by the first psychometrist provided more domain results (n = 8), compared to six domains provided by the other psychometrist (Table 1). Some subjects did not complete testing for motor or adaptive functioning. All test results were converted to z scores to establish a consistent unit for comparison across tests. Refer to Table 1 for a list of all administered tests and the domains assessed by each measure. The level of complete data also varied based on the subjects' capacity for prolonged testing across multiple sessions.
Neurocognitive Tests and Domains Assessed
Establishing the FASD group
Canadian guidelines for diagnosing FASD were originally developed in 2005,48 and were updated in 2015.23 Because this study was conducted prior to the 2015 update, the original 2005 guidelines were used as the basis for informing the research. According to the 2005 guidelines, assessment for FASD requires a multidisciplinary team to examine facial features and growth abnormalities, evaluate neurodevelopmental function in numerous brain domains, and establish the likelihood of PAE.48 For a diagnosis to be made, significant impairment is required in at least three of the eight brain domains outlined in Table 1. Confirmation of PAE is also required for diagnosis under the Canadian guidelines.39,49
In our study, subjects underwent a physical examination for facial dysmorphology, head circumference, and growth restriction (as per the 2005 guidelines).48 To establish the FASD group, subjects with evidence of three dysmorphic facial features closely associated with PAE (i.e., thin upper lip, flattened philtrum, and small palpebral fissure lengths) were considered to meet the criteria for FASD. Anyone with a previously documented FASD diagnosis in their medical records was also placed in the FASD group. Because the clinic is in Canada, it is likely that the Canadian diagnostic guidelines were used for these previous diagnoses; however, this information was not confirmed. On the basis of these criteria, a total of 12 subjects were identified with FASD either by the presence of the three dysmorphic facial features or by a previously documented FASD diagnosis. The remaining 33 subjects formed the No-FASD group.
Collateral information related to PAE was sought for all subjects. Steps included interviewing subjects regarding maternal drinking information, collecting contact information for a main support person and any caseworkers to obtain collateral information, checking clinic files for any mention of PAE, and attempting to obtain any additional records. Despite these efforts, there was no conclusive way to establish additional diagnostic rigor nor to rule out the possibility of PAE in the No-FASD group, as is very often the case in FASD research.49
Data Analysis
Descriptive statistics were used to examine trends in subject demographics, background information, offense histories, and neurocognitive profile. Because neurocognitive data were collected from multiple measures, all test results were converted to z scores to establish a consistent unit for comparison across tests. Differences between the FASD and No-FASD groups were examined using chi-squared and t tests for demographics, background information, and offense histories, and using multivariate analysis of variance for neurocognitive profile. Across analyses, statistical significance was set to P < .05, and effect size was determined using Cramér's V and partial eta-squared (ηp2).
Results
Demographics
A summary of demographic variables of the 45 subjects is displayed in Table 2. Data on subject backgrounds revealed extensive life adversity in the areas of child welfare involvement (29.7%), social service access (40.0%), and problems with school (75.0%) and employment (52.5%). This group was also clinically very complex, with high rates of substance misuse and other comorbid mental health concerns (Fig. 1). Data on mental health history were only available for 28 to 36 subjects, depending on the variable.
Participant Demographics
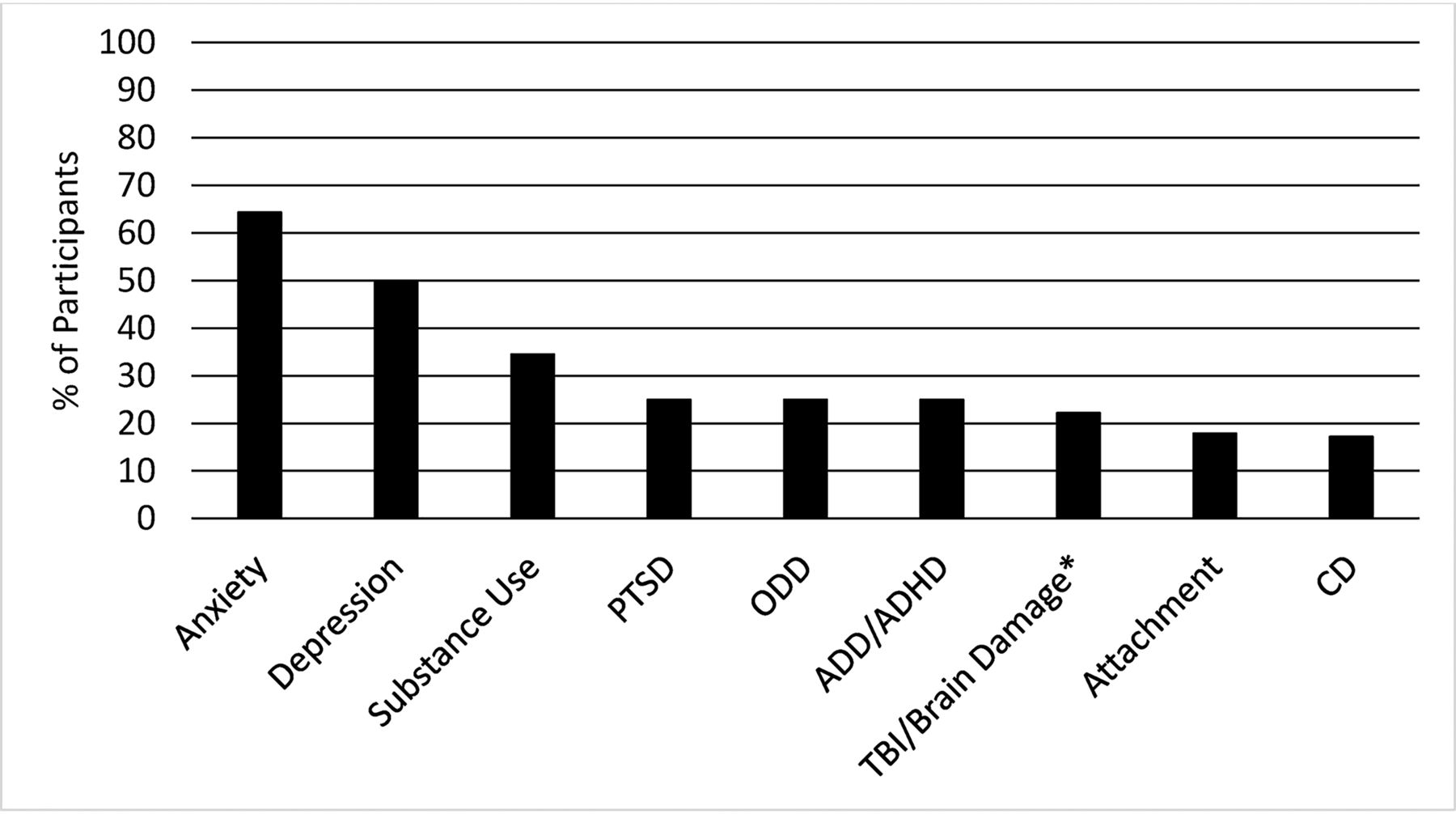
Subject clinical diagnoses. PTSD, posttraumatic stress disorder; ODD, oppositional defiant disorder; ADD/ADHD, attention deficit disorder/attention deficit hyperactivity disorder; TBI, traumatic brain injury; CD, conduct disorder. *For subjects with FASD, a diagnosis of TBI/brain damage required an incident above and beyond the damage caused by PAE.
Offense Histories
Two thirds (66.7%) of the subjects committed multiple crimes, and the mean number of offenses committed per subject was 3.7 (= 0–17). Figure 2 shows the broad categories used to estimate the most common type of offense represented in our sample, which included property/vehicle crimes (i.e., break and entry, robbery, possession of weapon, vehicle theft, theft under $5,000 or over $5,000, possession of stolen property or equipment, arson, vandalism/mischief, major driving offense, or fraud), followed by violent crimes against persons (i.e., assault, murder/manslaughter), obstruction/breach (i.e., administration of justice offenses), sex crimes, drug crimes, and nonviolent crimes against persons (i.e., kidnapping or death threats).
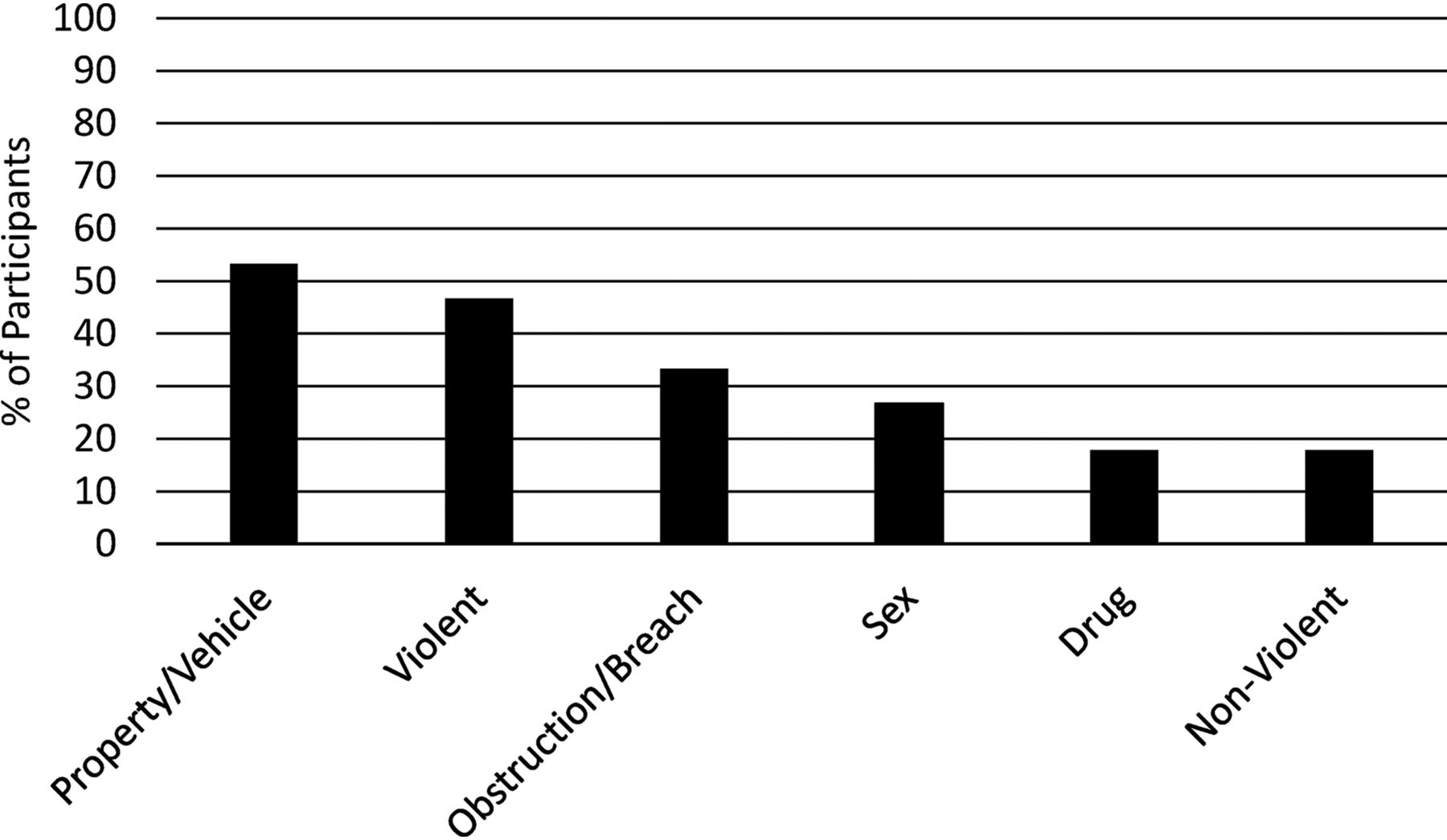
Subject offense histories.
Neurocognitive Profile
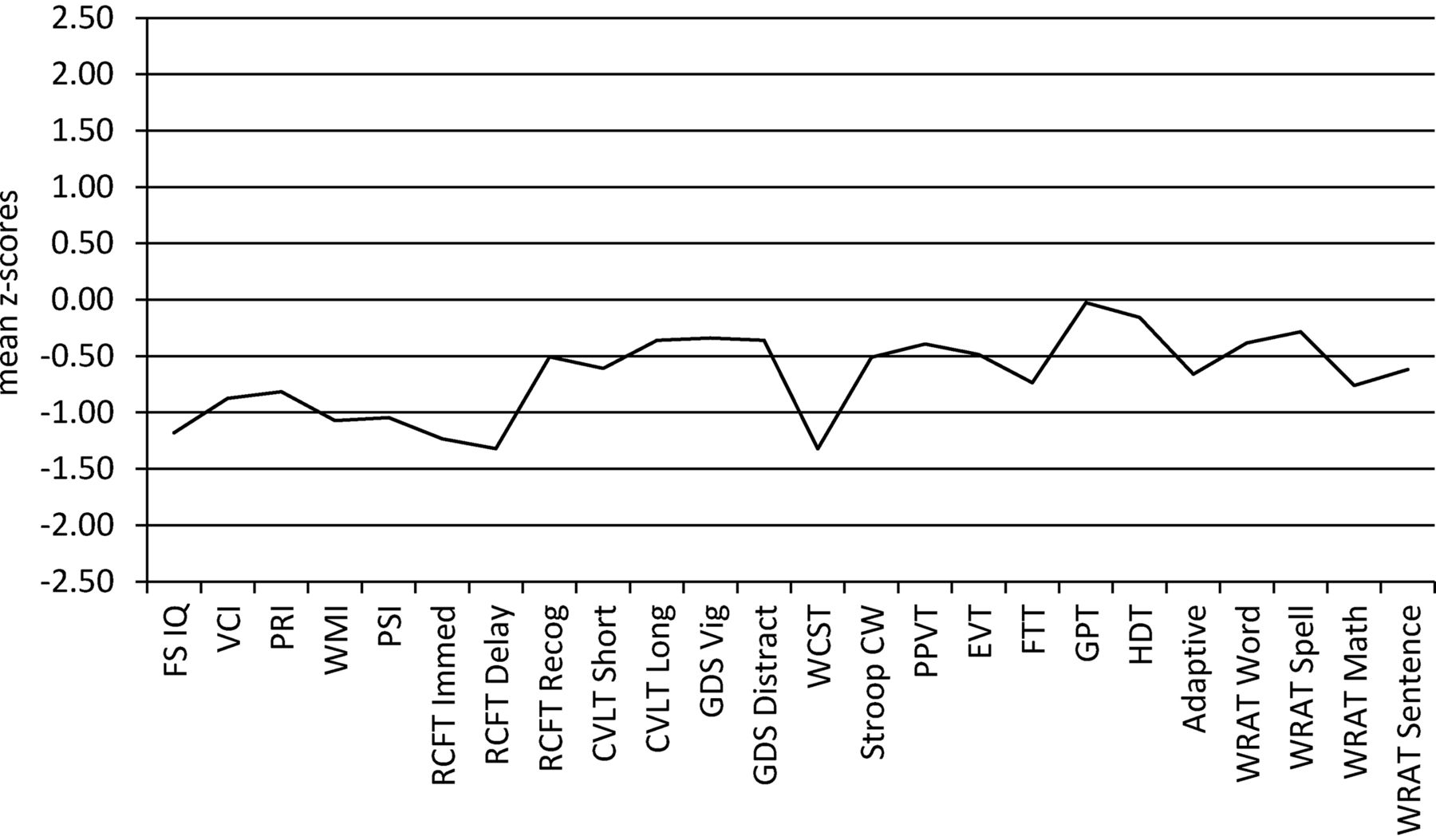
A total of 36 subjects completed neurocognitive testing (10 of 12 of the FASD group, and 26 of 33 of the No-FASD group). Figure 3 illustrates the mean test scores and number of subjects in each domain. Test results are presented as z scores, which have a normative mean of 0 and a standard deviation (SD) of 1. Individuals who score < −1 SD on neurocognitive tests might be considered clinically “at risk,” and those who score < −2 SD may be considered “significantly impaired.” In offender populations specifically, researchers examining cognitive trends have identified performance thresholds of < −1 SD as being “poor” and < −1.5 SD as “very poor.”50

Neurocognitive testing profile of all subjects. FS, full-scale (n = 36); VCI, verbal comprehension index (n = 36); PRI, perceptual reasoning index (n = 36); WMI, working memory index (n = 36); PSI, processing speed index (n = 36); RCFT, Rey Complex Figure Test (n = 35); CVLT, California Verbal Learning Test (n = 32); GDS, Gordon Diagnostic System (n = 19); WCST, Wisconsin Card Sorting Test (n = 31); CW, Color Word (n = 34); PPVT, Peabody Picture Vocabulary Test (n = 19); EVT, Expressive Vocabulary Test (n = 35); FTT, Finger Tapping Test (n = 19); GPT, Grooved Pegboard Test (n = 19); HDT, Hand Dynamometer Test (n = 19); WRAT, Wide Range Achievement Test (n = 19).
Subjects scored below the general population's normative means in every neurocognitive domain. They showed the weakest (i.e., poor) performance in executive function (as measured with the Wisconsin Card Sorting Test [WCST]), visual memory (immediate and delayed recall), working memory, processing speed, and full-scale IQ. Performance was somewhat stronger (i.e., between −0.5 and 0 SD) in motor dexterity, grip strength, spelling, word reading, attention, delayed verbal recall, and receptive and expressive vocabulary, suggesting relative strength in these areas, but nonetheless lower than the normative mean.
FASD Group Differences
Chi-squared and t tests revealed no significant differences between the FASD and No-FASD groups in terms of age (t(43) = .044, P = .965), gender (χ2(1) = 0.014, P = .906, V = .018), living situation (χ2(4) = 5.588, P = .232, V = .360), employment (χ2(5) = 5.004, P = .415, V = .341), highest level of education (χ2(3) = 1.540, P = .673, V = .194), or marital status (χ2(2) = 2.744, P = .433, V = .250). Despite some apparent group differences in clinical diagnoses, none of these were statistically significant (Table 3). The small sample size may explain this lack of statistical significance.
Rates of Comorbid Diagnoses in the FASD and No-FASD Groups
Subjects in the FASD group committed fewer total crimes (mean = 2.33, SD = 2.84) than those in the No-FASD group (mean = 4.21, SD = 4.83), and a smaller proportion of subjects in the FASD group than No-FASD committed crimes in every category except for violent crimes. None of these differences were statistically significant (Table 4).
Offense Histories in the FASD and No-FASD Groups
Neurocognitive test scores were compared only on domains where at least five subjects in each group completed the testing measure. Depending on the domain, the number of FASD subjects in these analyses ranged from 8 to 12, and the number of No-FASD subjects ranged from 14 to 22. As was found with overall group profile, both groups scored below the normative mean across domains (Fig. 4).

Comparison of neurocognitive profile between the FASD and No-FASD groups (*P < .05, **P < .01). FS, full-scale; VCI = verbal comprehension index; PRI, perceptual reasoning index; WMI, working memory index; PSI, processing speed index; RCFT, Rey Complex Figure Test; CVLT, California Verbal Learning Test; WCST, Wisconsin Card Sorting Test; CW, Color Word; EVT, Expressive Vocabulary Test.
Subjects in the No-FASD group showed the weakest performance (< −1 SD) on a test of executive function (as measured with the WCST) and visual memory (immediate and delayed recall). Their scores hovered around −1 SD on full-scale IQ, processing speed, and working memory. Subjects in the FASD group showed clinically significant impairment (< −2 SD) in visual memory (delayed and immediate recall), with additional pronounced deficits (< −1.5 SD) in full-scale IQ, verbal IQ, working memory, and processing speed.
Somewhat higher scores (> −0.5 SD) were obtained by subjects in the No-FASD group in expressive vocabulary, long-term verbal memory, and cued visual memory. Those in the FASD group showed their highest scores (> −1 SD) in verbal memory (short-term and long-term), executive function (both the Stroop Color-Word [C-W] test and the WCST), and cued visual memory.
To analyze group differences in neurocognitive profile, a MANOVA was conducted with group membership as the independent variable and test scores (where at least five subjects in each group had completed the measure) as dependent variables. Results revealed a group difference in overall neurocognitive profile bordering on significance [F(13,11) = 2.77, P = .050 (ηp2 = .766)]. A post hoc ANOVA showed group differences in multiple domains of neurocognitive functioning with significantly lower scores in the FASD group than the No-FASD group in verbal IQ, [F(1,23) = 11.25, P = .003 (ηp2 = .328)], full-scale IQ, [F(1,23) = 8.99, P = .006 (ηp2 = .281)], working memory IQ, [F(1,23) = 5.36, P = .030 (ηp2 = .189)], processing speed IQ, [F(1,23) = 4.63, P = .042 (ηp2 = .168)], and expressive vocabulary, [F(1,23) = 4.54, P = .044 (ηp2 = .165)]. The FASD group scored notably (but not statistically significantly) higher than the No-FASD group on the WCST, a measure of executive function.
Discussion
The overarching purpose of this study was to explore the experiences and characteristics of outpatient OMDs, with a focus on neurocognitive functioning. We also conducted a closer examination of whether OMDs differ in presentation depending on whether they have FASD. Considering the over-representation of mental disorders, neurocognitive impairment, and FASD in offender populations, and the paucity of research examining the intersection of these categories, this study represents a contribution to better understand and support this group. OMDs with FASD showed more neurocognitive impairment than those without FASD in the domains of full-scale IQ, verbal comprehension, working memory, processing speed, and expressive language. Those with FASD were less impaired than those without in the domain of executive function, although this difference was not statistically significant.
Characterizing Offender Backgrounds
The subjects in this study comprise a group of individuals with significant experiences of adversity, multiple comorbidities, and varied offending histories. Not surprisingly, this sample has many of the risks factors associated with criminality and adverse mental health outcomes, including high rates of anxiety and depression, substance misuse, school and work disruption, trauma, being currently unmarried, and histories of repeat offending.51 These findings contribute to the evidence that OMDs are a complex group of individuals with multifarious histories indicating urgent need for long-term, comprehensive, and multidisciplinary support, both while incarcerated and when released into the community.
Neurocognitive Profile
We found a pervasive pattern of impairment across neurocognitive domains for all subjects in this study, with mean scores for all measures falling below the normative mean. These findings are reflective of other research emphasizing the high prevalence of cognitive deficit among offenders. For example, Canadian researchers recently found that 25 percent of incoming male offenders had “some level of cognitive deficit” (Ref. 52, p 12) defined by the authors as at least two mild or one moderate domain of impairment as measured with the Cognistat screen of cognitive function. Cognitive deficit in that study was also associated with lower educational achievement, unstable employment history, learning disabilities, serious alcohol problems, and symptoms of attention deficit hyperactivity disorder.52 Cognitive deficits were not related to participation in or completion of required correctional programs, returns to custody, or reoffending.
Building on these earlier findings, our results provide additional evidence that OMDs and neurocognitive impairments warrant specialized support, including educational and employment strategies and mental health and addictions services. Furthermore, because offenders with neurocognitive deficits appear to be responsive to treatment and do not appear to present an elevated management concern while institutionalized or once back in the community,52 successful rehabilitation and reintegration is a practical goal.
In terms of a specific neurocognitive profile, the most notable areas of deficit for our subjects were identified in executive function, visual memory (immediate and delayed recall), working memory, processing speed, and full-scale IQ.
Due to the role of executive function in self-regulation, abnormalities in executive function have previously been associated with offending and reoffending,53 among other serious negative life outcomes.54 Deficiencies in mental flexibility, impulse control, and anger control have been proposed as some of the specific mechanisms by which executive function deficits are associated with criminal activity.55,–,57 It is therefore not surprising that executive function was one of the most pronounced areas of neurocognitive impairment among the subjects in our study.
Reoffending behavior can also be a reflection of the indirect manifestations of executive dysfunction, such as difficulty to plan housing and employment or challenges with self-regulation.58 Our subjects appear to be supported in these areas, as demonstrated by their reported housing situations (42% living independently), educational success (34% completing at least some postsecondary training), and occupations (33% employed or in full-time studies), suggesting that some of the daily manifestations of executive function impairment may be relatively well-managed in this group. More research is needed to better understand how executive function deficits impact specific groups of offenders, such as OMDs, and how this impact may translate to daily function. Investigations into what supportive factors contribute to positive outcomes despite executive function difficulties would also be warranted.
Another area of notable deficit identified in our subjects was visual memory, with both immediate and delayed verbal recall scores falling well below the normative mean. This finding is consistent with previous research demonstrating visual memory deficits in the general offender population.50 Subjects in this study scored much higher on a measure of cued visual memory. This finding has important practical implications in that visual cues may be one way to improve OMDs' understanding of and compliance with the justice process. For example, presenting visual reminders alongside verbal instructions may support a better understanding of sentencing decisions and memory for probation orders, potentially reducing the risk of breaching court orders, which was a problem for a substantial proportion (33%) of our subjects.
Working memory, processing speed, and full-scale IQ were also found to be relatively impaired among subjects in this study, with scores in these areas falling lower than 1 SD below the mean. The full-scale IQ score is based on (and therefore influenced by) the working memory and processing speed index scores, in addition to verbal comprehension and perceptual reasoning scores. It would therefore appear that the working memory and processing speed skills are the primary factors that pull down the full-scale IQ scores for these individuals. Again, these results are not surprising considering that IQ scores in forensic samples have been found to be lower than the general population mean.59
Clinically, working memory and processing speed impairments impede an individual's ability to multi-task, to hold large amounts of information in mind at once, to understand and follow multi-step instructions, and to make speeded decisions, especially in high-pressure environments. This has relevance in justice settings where offenders, especially those with disabilities, are likely overwhelmed and may struggle to understand instructions and criminal proceedings. Tailoring our practices to account for these deficits at all stages of the justice process (e.g., arrest, interrogation, sentencing, incarceration, probation, community integration, etc.) would help to ensure that offenders are given the best opportunities to achieve successful outcomes.
Subjects in this study also demonstrated areas of relative strength in the areas of motor dexterity and grip strength, spelling and word reading, attention, delayed verbal recall, and receptive and expressive vocabulary. These findings highlight important areas for targeting strengths-based justice interventions to build upon offender abilities rather than to focus solely on remediating one or more deficits. These areas of relative strength also provide a contextualized understanding that neurocognitive impairment is not experienced uniformly across all domains of functioning, suggesting that justice and clinical service providers should seek to understand the unique profile of functioning of each person to provide the best individualized care possible.
These neurocognitive findings indicate that OMDs show impairment in numerous areas of functioning, many of which overlap with deficits found in the general offender population. These findings have important implications for informing justice practices. Potential areas for reform include implementing screening for all offenders to identify neurocognitive deficit; conducting comprehensive individualized assessment for those with demonstrated need; and tailoring sentencing, programming, and treatment approaches to compensate for deficits and to build upon strengths. With emerging evidence that targeted therapies such as cognitive remediation show promise for improving a variety of functions in forensic and psychiatric patients,60 it becomes even more important to consider brain and mental health functioning in our understanding of the offender. In doing so, offenders with all levels of ability will have better access to appropriate supports and services.
Offenders with FASD
Our final research goal was to explore whether OMDs with FASD present differently than those without FASD. Typically, individuals with FASD are reported to experience high rates of trauma, early life adversity, and poor long-term outcomes.61 Thus, it was surprising to find that our groups showed comparable life experiences, with no significant differences in background characteristics, offense histories, or mental health profiles. These findings suggest that OMDs with and without FASD may experience similar life challenges and indicate that these struggles may not necessarily be unique to the FASD population. Rather, the relationships between life adversity, mental health, and PAE are complex and intertwined, warranting further research to explore how they might influence the pathway to justice involvement.
The finding that the FASD group appeared to commit fewer crimes across all offense categories except violent crimes (this difference was not statistically significant) is an important contribution to the literature because there is little research on specific offense patterns in the FASD population. These results should be interpreted with caution, however, because the current sample size was small and its statistical power was limited. Future research with larger samples should be conducted to continue examining these trends to reveal where differences, if any, in offending patterns exist between offenders with and without FASD.
Few studies have specifically investigated the unique components of neurocognitive deficit in offenders with FASD, though new research is beginning to emerge. In one recent study, researchers compared the neurocognitive profiles of young offenders with and without FASD and found that subjects in the FASD group showed significantly lower scores in cognitive flexibility, simple processing speed, working memory, and verbal and full-scale IQ, and they exhibited notable (but not statistically significant) deficits in verbal academics.62 Consistent with this previous research, subjects in our FASD group showed significantly lower scores than those in the No-FASD group in full-scale and verbal IQ, as well as in working memory and processing speed. These findings could have relevance for the structuring of interventions and supports for offenders with FASD within justice and community settings. For example, interventions that rely heavily on working memory or a certain level of processing speed may not be effective in this population. Additionally, offenders with FASD in our study showed significantly more impairment than offenders without FASD on a measure of expressive vocabulary. These findings related to language are important because expressive language disorder is known to be one of the most common comorbid conditions in the general FASD population,63 and verbal deficits are a particularly strong predictor of delinquency in youth.64 Combined, these findings indicate that further research is warranted to explore whether or how expressive vocabulary and verbal ability relate to offending behavior in FASD specifically and whether language-based interventions might influence outcomes.
Offenders with FASD in our study did not show more impairment relative to the No-FASD group on two measures of executive function. Whereas executive dysfunction is known to be a hallmark feature of FASD,65 our subjects with FASD showed comparable scores on the Stroop C-W task, and higher (though not statistically significantly) scores on the WCST compared to the No-FASD group. The Stroop C-W test is often thought of as an inhibition task, whereas the WCST measures planning and cognitive flexibility in response to feedback. Flannigan et al.66 also showed that young offenders with FASD demonstrated performance similar to that of a comparison group on the Stroop C-W task, but that they scored significantly lower on a measure of cognitive flexibility. These conflicting results suggest that more work is needed to tease apart which elements of executive function are most influential in the context of criminal behavior in FASD.
Individuals with FASD and mental disorders are not only over-represented in the criminal justice system as perpetrators, but may also be more likely to be victims and witnesses to crime.67,–,69 Individuals with FASD who offend have also often been victimized themselves and may struggle with adjusting to correctional environments, perpetuating the cycle of justice involvement.45 Given the over-representation and vulnerability of individuals with FASD in justice settings, there is an urgent need for proactive support for this population and for adjustments that protect individuals with FASD from encountering and reencountering this system.
Limitations and Future Research
Several methodological factors reduced the statistical power and generalizability of our study, such as the small sample size, limited geographical region, and specific subject population. Sampling error and drop out are likely also limiting factors, in that individuals who chose to participate or stayed in the study were perhaps higher functioning and more independent than those who declined or dropped out. The process of referral, including community supervision and links with health care, could have contributed to a more stable population, whereas individuals with lower functioning may not have been able or willing to participate. Although many of our results are consistent with previous studies, further research with larger and more representative samples is warranted to strengthen the validity of our findings. Longitudinal research would also shed light on the long-term influence of mental health problems on criminality, age-related changes in neurocognition, and whether or how the trajectory of criminal justice involvement is different for offenders with FASD compared with those without.
Another set of limitations in our study relates to challenges inherent in neurocognitive testing. First, one of the ongoing challenges of research using laboratory measures to assess neurocognitive functioning is ensuring ecological validity.70 Future research should employ tasks with more practical and clinical utility such as the Behavioral Assessment of the Dysexecutive Syndrome (BADS), which could better identify functional needs and inform treatment planning.71 Because assessment should always be connected to intervention, clinicians and practitioners need to carefully consider and utilize tools with a practical role. Second, our analysis of neurocognitive test scores was limited by the relatively small number of subjects who completed the measures. Although this study employed a more comprehensive battery than many previous studies of neurocognitive functioning in OMDs, important areas of deficit or strength may have been missed in our battery. Moreover, using two different psychometrists with different training and levels of experience was not ideal and could impact the findings of the neurocognitive tests. Because retesting the subjects within the study period would have introduced practice effect, and because having the patients come in repeatedly for additional testing was not feasible, we adjusted the domain numbers per psychometrist and utilized z scores. This allowed us to comment on neurocognitive impairments, but we lost the ability to analyze and compare the magnitude of neurocognitive tests by the two psychometrists as a continuous variable. Additional research with larger samples and even more comprehensive and consistent testing could provide a clearer picture of the neurocognitive profile of offenders with mental disorders and FASD.
Our exploration of FASD was also limited in several ways. The small number of subjects with FASD restricted our ability to examine differences between FASD and No-FASD groups with strong statistical power, and we were not able to compare groups across all domains of neurocognitive functioning. It is possible that important group differences in life experiences, criminal history, and neurocognitive function may have existed that we were not capable of detecting. Moreover, multidisciplinary assessments were not conducted with each subject, and some individuals in the FASD group were categorized based solely on facial dysmorphology where PAE could not be confirmed. Other individuals were included on the basis of a previous diagnosis in their medical record, which we did not confirm further. This may have included false positives on the basis that those diagnoses may not have been rigorous. Another challenge, which is common in FASD research, is that it was impossible to rule out PAE in the No-FASD group. In our study, confirmation of PAE was exceptionally challenging to obtain given the age of the sample, disengagement with biological family members, high residential instability, and inconsistent record keeping in subjects' clinical histories. These difficulties are similar to those often faced by other FASD researchers, as well as in clinical settings, particularly among adults.49
The complexity of our study population makes it difficult to draw firm conclusions about etiology of neurocognitive impairment. For instance, all subjects in our study had at least one mental health diagnosis, most experienced serious long-term life adversity, and many had previous brain damage or traumatic brain injury, all of which can affect neurocognitive functioning. Additionally, the age of our subjects raises potential etiological questions. Although an age of 42 years would not typically indicate brain-related implications of aging, emerging evidence suggests that individuals with FASD (with a mean age of 28 years) report rates of early-onset dementia that are 104 times higher than the general population.71 Furthermore, connections between accelerated aging effects and serious mental illnesses are also beginning to be discussed in the literature.72,–,74 Due to these confounding etiological factors, our ability to clearly understand the mechanisms underlying neurocognitive impairment, mental disorders, PAE, and criminal behavior is clouded. Nonetheless, our study points out that, even though deficits in neurocognitive functioning can arise from multiple pathologies, PAE is worth adding to the layers of consideration due to the pervasive and severe nature of the brain-based deficits associated with PAE and the high prevalence of FASD in justice settings. Although FASD is certainly not the only disorder over-represented in the justice system, lessons learned in this population can guide change in policy and practice that may directly benefits other groups of offenders with cognitive diversity.
Finally, many individuals with mental disorders and FASD do not engage in criminal activity, and these are crucial populations for further study. Exploring the factors that differentiate these individuals from those who offend would greatly improve our ability to develop strengths-based interventions, promote resilience, and support positive outcomes for at-risk populations.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2020 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}
{kind=link}
{kind=link}