


Abstract
Apologies are an integral part of human communication and can repair damaged relationships. Within the medical system, apologies remain controversial. Physicians often wish to apologize to patients harmed by medical errors, but they may not disclose errors to patients and their families because of the concern that disclosing errors could increase the likelihood of a malpractice claim. Yet physicians who apologize to patients may instead mitigate many of the communication problems known to prompt patients to pursue legal action. This idea has prompted many state governments to pass apology laws, legislation that aims to reduce rates of malpractice by encouraging physicians to apologize. These laws have not yet had their intended effect of reduced malpractice rates, likely because most apology laws protect expressions of regret but do not protect error disclosure. Apology laws therefore do not facilitate the type of communication that would improve physician transparency and overall patient satisfaction.
An apology can have tremendous therapeutic potential for both parties. Apologies can reduce anger, promote healing, and repair damaged relationships.1,–,3 To have positive effects, an apology must be given well. An effective apology generally contains four elements: the acknowledgment of harm, evidence of remorse, an offer to repair any damages, and the promise of behavioral change.3,–,5 Above all, an apology must be sincere.3,–,5 Many aspects of an apology signal sincerity, such as appropriate timing, a lack of defensiveness, clear evidence of reparative action, and an absence of any evident ulterior motives for apologizing (e.g., financial reward or avoidance of punishment).3,4 Of course, effectively incorporating all these elements requires significant interpersonal skills. Even the most effective apology may fall short if the offense is severe enough. Other factors that may affect an apology’s effectiveness include the relationship between the two parties and how motivated they are to reconcile the relationship.
A bad apology is often worse than no apology at all.5 Apologies perceived to be inadequate can be met with anger, hurt, and criticism.4,5 Ineffective apologies are so common that the word nonapology has been created, defined as a statement that takes the form of an apology but does not constitute an acknowledgment or regret for what has caused offense or upset.6 A classic example of a nonapology is a statement such as, “I am sorry if I hurt you.” While this statement appears apologetic, a closer look reveals a lack of responsibility or even true acknowledgment of harm.
As the saying goes, “to err is human.”7 A well-functioning society requires mechanisms to repair relationships when they are damaged by human error. Apologies, when used correctly, can be a restorative tool. This therapeutic potential has prompted the consideration of apologies and their role in health care systems.
Apologies in Medicine
Bad outcomes, such as illness, injury, and death, are expected in medicine. In the words of author and neurosurgeon Atul Gawande, “Death is the enemy. But the enemy has superior forces. Eventually, it wins” (Ref. 8, p 187). That said, a significant number of harmful patient events are caused by preventable medical errors.9 A report published in 2000 by the Institute of Medicine estimated that preventable medical errors cause as many as 98,000 deaths in the United States each year, more than the death toll from car accidents, breast cancer, or AIDS.9
When patients are harmed by medical errors, most physicians desire to apologize to patients.10,–,13 Many medical ethics arguments support error disclosure, including respect for autonomy, non-malfeasance, and beneficence. Consideration for patient autonomy suggests that patients have a right to make their own health care decisions, which requires knowledge of events that have affected their health. Knowledge of a harmful error could help patients avoid related future injury (i.e., non-malfeasance) and improve their health (i.e., beneficence).
Error disclosure in medicine is a relatively new phenomenon. The medical field has a long history of discouraging physician transparency. The American Medical Association’s first Code of Ethics, published in 1847, recommended physicians closely monitor their words and behavior, and “avoid all things which have a tendency to discourage the patient and to depress his spirits” (Ref. 14, p 9). A popular physician training manual written around the turn of the 20th century recommended that physicians be “at liberty to be silent or to say but little regarding the nature or degree of a person’s sickness . . . in every stage of your career aim to convince the world that you, as a physician, are an apostle of hope . . . and that your profession is not in league with the grim forces of death and mourning, but that, on the contrary, all its characteristics are indicative of health-giving and life-restoring power” (Ref. 15, p 140). For many years, physicians were encouraged to instill optimism in patients, at the expense of full disclosure.
With time, this expectation has changed. The landmark cases of Salgo v. Leland Stanford University,16 Natanson v. Kline,17 and Canterbury v. Spence18 established the expectation that physicians discuss information as part of obtaining informed consent from patients. Regulatory bodies and national organizations increasingly have called for improved physician and health care system transparency, prompted in large part by the Institute of Medicine’s report.9 The U.S. Department of Health and Human Services finalized rules in 2020 that permit patients full access to their electronic health record, adding a new dimension to physician–patient communication that will need to be navigated.
Patients want to learn about medical errors that affect their health.12,13 Most physicians support error disclosure and believe they have an ethics obligation to disclose harmful errors to their patients or families, even if this disclosure comes at a personal or professional cost.10,11,13 For psychiatrists, a common scenario is whether to apologize to a patient’s family after a patient suicide. A related consideration may be whether to attend the patient’s memorial service.
In practice, physicians typically do not disclose harmful errors to patients.10,11,13 In a survey of U.S. physicians published in 2007, 320 (95%) of the 338 responding physicians indicated that they felt obligated to tell patients about such a mistake; however, only 41 percent of respondents reported that they had in practice disclosed minor harmful errors to their patients, while only five percent reported that they had disclosed major errors.11 Clearly, a discrepancy exists between physicians’ desire to disclose and their practice of disclosing errors.
There are likely many reasons for the discrepancy noted above. Lack of comfort with this type of difficult conversation may pose a barrier to disclosure. Less experienced physicians are generally less likely to disclose errors, suggesting that a lack of practice and confidence are factors.11 Physicians also wonder what information to disclose, such as details about the error and prevention of similar errors in the future.11,13 Physicians can be affected deeply by harmful errors, with reactions including insomnia, guilt, poor concentration, anxiety, and self-doubt.11,13 Strong emotional reactions may make the prospect of having these already difficult conversations more daunting. Physicians may struggle with determining how much of their own emotions they should share with patients and families, concerned that these responses may be a burden.17 Physicians may also worry that disclosure could erode patients’ trust and damage the physician–patient relationships. 11,13 Professional ramifications of disclosure are another concern. Physicians fear negative reactions from colleagues and damage to their professional reputations.11,13 Finally, a major reason physicians worry about disclosing medical errors with patients is the concern that this disclosure will lead to a malpractice suit.11,13
Apologies and Malpractice
Most physicians in the United States face at least one malpractice lawsuit over the course of their careers.19 Malpractice is a common and costly occurrence in the United States.19,–,21 Malpractice also takes a significant emotional toll on physicians, regardless of the outcome.22 Most physicians worry about facing a malpractice suit and its many implications, including professional, financial, and psychological challenges.22,23 Physicians may therefore avoid disclosing errors to patients in an effort to avoid incurring a malpractice claim.
In theory, telling a patient about an error may make patients more likely to pursue litigation. In practice, however, bad outcomes alone are typically not reason enough for patients or their families to file malpractice claims.24,25 A major reason malpractice claims are pursued is related to bad feelings evoked.24,25 These bad feelings can be prompted by real or perceived problems with physicians’ communication skills.12,24,25 Physicians who appear to be insensitive, unavailable, or critical are much more likely to be sued.24,25 Patients and families are also more likely to sue if they feel a physician is hiding or withholding important information.12,24,25 In this instance, litigation may be viewed as a means of obtaining the desired information.12,24,25
Malpractice lawsuits may also be viewed as a way to prevent similar errors from occurring to other patients in the future.24 A physician who does not demonstrate remorse for a harmful error may make patients more likely to consider legal recourse. 24 An apology, through its acknowledgment of fault, expression of remorse, offer to repair damages, and promise of behavioral change, could assuage many of these patient concerns, thereby reducing the likelihood that patients will file malpractice claims. Many patients explicitly identify a lack of apology as a reason they chose to pursue a malpractice suit.12,24
Hospital-based error disclosure programs demonstrate a role for apologies in reducing malpractice claims.26,–,30 Several hospital systems around the United States have implemented disclosure programs with the goal of increased transparency and reduced medical errors.26,–,30 The programs generally involve the proactive identification of harmful medical errors and disclosure of these errors to patients and families.26,–,30 These programs often provide extensive communication training to providers, including advance preparation for challenging discussions and instruction on active and reflective listening skills.26,28 In addition, these programs offer financial compensation to those affected by medical errors.26,–,30
Hospitals with such disclosure programs have not seen a higher malpractice burden, and many have observed fewer malpractice claims and reduced costs overall.28,–,30 As an example, the University of Michigan Health System’s disclosure program has resulted in a decreased number of malpractice claims, from an estimated monthly rate of 7.03 per 100,000 patients in 2001 (i.e., at the start of program implementation) to 4.52 per 100,000 patients in 2007 (i.e., at the end date of data collection).28 They also observed a decreased average cost per lawsuit from $405,921 to $228,308, as well as an expedited claim resolution process in this time period.28 Another such program at an academic health system in Tennessee also demonstrated fewer malpractice claims, lower legal costs, and shorter time from claim to resolution.30 Disclosure programs and their demonstrated reductions in malpractice events and costs substantiate the hypothesis that physician apologies decrease, not increase, the risk of malpractice litigation.28,–,30 Patients themselves may prefer this process to a malpractice suit, particularly given that many of the outcomes may be comparable with the outcome of a successful malpractice suit, including physicians’ apologizing for the error and financial compensation being provided.
There are some potential criticisms of these programs. While financial compensation alone is typically not reason enough for a patient to pursue a malpractice suit,28 it is worth noting that offering an easier route for financial compensation could motivate patients to accept this offer in lieu of pursuing a malpractice claim. Some might also argue that these programs may hide information about medical errors about which the public should be aware. It is worth noting, however, that information about malpractice claims may not be routinely and publicly available. These programs therefore do not function inherently to restrict access to information that would otherwise be available to the public.
With these overall promising results of hospital disclosure programs with regard to rates of malpractice, other entities have also explored apologies as a tool for reducing malpractice claims. This consideration has led to the development of state-legislated apology laws that protect a physician’s apologetic statements in the event of a malpractice suit.31,–,71
Apology Laws
Apology laws render physicians’ apologetic statements to patients inadmissible should that patient subsequently choose to pursue a malpractice claim. By providing legal protection to apologies, physicians may be more inclined to apologize to patients and engage more transparently with their patients. For reasons discussed above, improved physician communication may make patients and their families less likely to pursue litigation.12,24,25 Massachusetts passed the first apology law in 1986.65 Currently, 39 states and the District of Columbia have apology laws (Fig. 1, Table 1).31,–,71 In 2005, then-senators Hillary Clinton and Barack Obama proposed federal apology protection as part of the National Medical Error Disclosure and Compensation (MEDiC) Act.72 The MEDiC bill involved protection of apologies, as well as the creation of a national patient safety database and a national error disclosure and compensation program.72 The MEDiC bill did not ultimately become law.72 Apology laws, like tort reform, aim to reduce rates of malpractice lawsuits. Some authors have argued that they represent a variety of tort reform.73
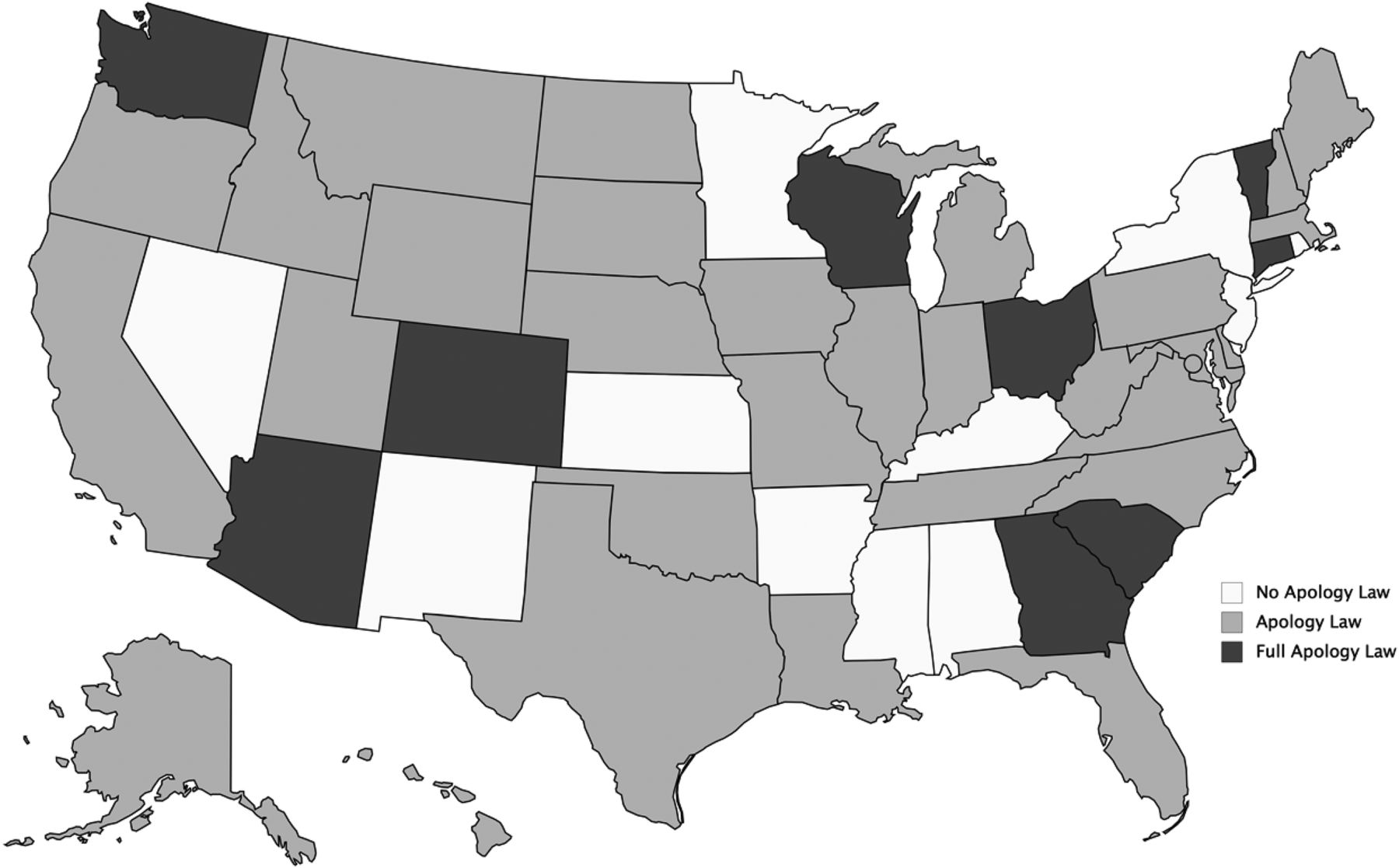
Apology laws in the United States as of October 2020.
Apology Laws in the United States as of October 2020
There are generally two types of apology laws, full and partial apology laws (Fig. 1, Table 1).31,–,71 Full apology laws protect statements that are consistent with the definition of an apology, i.e., an expression of regret and a disclosure of error.31,–,39 States with full apology laws explicitly protect statements of fault. For example, Arizona’s apology law protects “any statement, affirmation, gesture or conduct expressing apology, responsibility, liability, sympathy, commiseration, condolence, compassion, or a general sense of benevolence” from being admitted as evidence.31 This law protects statements of “responsibility” and “liability,” which firmly establishes Arizona’s apology law as a full apology law. Partial apology laws protect expressions of regret only, without any protection given to error disclosure.40,–,71 The vast majority of states protect sympathetic statements and do not protect expressions of fault explicitly.40,–,71 For example, North Dakota’s apology statute protects a “statement, affirmation, gesture, or conduct of a health care provider . . . which expresses apology, sympathy, commiseration, condolence, compassion, or benevolence to a patient or to a patient’s relative or representative.”45 In states with partial apology laws, physicians who make a full apology to a patient will only have the statement of regret excluded as evidence.
An example of apology laws in practice was seen in the case of Stewart v. Vivian.74 This Ohio malpractice case occurred after Michelle Stewart died by suicide while psychiatrically hospitalized.74 Dennis Stewart, Mrs. Stewart’s husband, sued his wife’s psychiatrist, Rodney Vivian. Mr. Stewart alleged that Dr. Vivian spoke with Mr. Stewart and said that “it was a terrible situation, but [Mrs. Stewart] had told [Dr. Vivian] she . . . wanted to kill herself” (Ref. 74, p 719). Mr. Stewart actually said that he did not recall Dr. Vivian apologizing or offering sympathy.74 Dr. Vivian testified that he had told Mr. Stewart he was “sorry this has happened” (Ref. 74, p 718). The court ruled in favor of Dr. Vivian, and the Court of Appeals of Ohio affirmed. The Court of Appeals also examined Ohio’s apology statute, which previously had been interpreted as a partial apology law.74,75 Upon examining the language, which specifically stated an “apology” should be excluded, the Court of Appeals determined that this statute should, in accordance with the definition of an apology, protect error disclosure.74
In general, the therapeutic benefits of apologies are associated more closely with full apologies.1,–,3 Partial apologies and their impact are much harder to interpret. One reason for this is that the impact of partial apologies can vary depending on the type of information sharing between parties. Two types of information-sharing systems exist: symmetric and asymmetric information sharing. Symmetric information-sharing systems are fully transparent, and all parties have access to all information. As a hypothetical example, if Mr. Doe has a postoperative infection, he reasonably may wonder if his surgeon, Dr. Smith, made a medical error that caused this infection. If Mr. Doe’s infection was not the result of any medical error, but Dr. Smith expresses his condolences to Mr. Doe, Mr. Doe knows that this partial apology is indicated and a full apology is not. In this scenario, a partial apology is truthful, and Mr. Doe may value this expression of empathy. In a situation where information is shared asymmetrically, Mr. Doe may not know whether his infection is the result of Dr. Smith’s mistake. If Dr. Smith expresses his condolences about the infection, Mr. Doe may wonder whether a mistake was made but not disclosed. Dr. Smith himself may not know whether a mistake was made and perhaps wishes to wait until the peer-review process has been completed before sharing information. Regardless, the desire for more information could prompt Mr. Doe to pursue legal action.
Partial apologies have been studied and demonstrate effects that differ from full apologies.24,76,77 Compared with full apologies, partial apologies are less likely to reduce anger, prompt forgiveness, or repair a damaged relationship.78 People who give full apologies versus those who give partial apologies are viewed generally as more moral and more likely to be careful in the future.78 Patients who know that harmful errors have occurred but have not received a full apology are considerably more likely to be angry, to change physicians, and to pursue litigation even if they have received a partial apology.24,76 In certain cases, partial apologies may result in worse outcomes than no apology at all.77
Effect of Apology Laws
Evidence regarding whether apology laws have affected malpractice claims and outcomes remains equivocal. To our knowledge, there have been only three extensive analyses of apology laws and their effects on malpractice claims; two were conducted by economists Benjamin Ho and Elaine Liu; the other by Benjamin McMichael and colleagues.79,–,81
The analyses by Ho and Liu79,80 observe that apology laws have increased physician apologies, expedited claim resolution, and decreased the number of and payments for malpractice claims. They used data from the National Practitioner Data Bank’s (NPDB) Public Use Database, a database of all malpractice payments made by or on behalf of health care practitioners in the United States.79,80 This database does not include information about payments made by health care institutions, including those made on behalf of physicians, nor does it include information about malpractice claims that did not result in payment.79,80 Ho and Liu observed an overall decrease in average malpractice payment of 12.8 percent due to decreased settlement amounts of malpractice cases involving severe injuries and a reduced number of malpractice cases involving less severe injuries, although the settlement amounts in cases involving less severe injuries were not reduced.79,80 They also observed expedited settlement time and an increased number of closed claims, which they posit is due to expedited settlement times rather than an increase in malpractice claims.80
The analysis by McMichael et al.,81 published in 2019, examines data from a large malpractice insurer. In contrast to data from the NPDB, this dataset includes unpaid claims.81 This expanded dataset is a strength of the study, particularly given the high emotional and financial costs that malpractice claims incur, regardless of outcome.23,81 The authors examined data from one specialty only, which for confidentiality purposes they did not disclose, although they noted that this specialty includes both surgeons and non-surgeons.81 Examining only one specialty limits confounding effects, but the inclusion of surgeons and non-surgeons enables the comparison of these two distinct types of physicians and their differing risks of malpractice suits.19,21,81 Restricting this analysis to one specialty limits the study’s generalizability, however, particularly when the specialty was not disclosed. Only states with partial apology laws were included in this analysis.81 This exclusion was due to the limited number of states with full apology laws and the argument that partial and full apology laws represent very different legal entities.81
McMichael et al.81 reported that apology laws did not change the overall likelihood of either surgeons or non-surgeons facing malpractice claims but did increase the likelihood of non-surgeons facing malpractice claims that led to litigation. The authors also noted that apology laws have increased total malpractice payments for both claims and lawsuits, and this increase is pronounced particularly for non-surgeons.81 The authors posit that these findings are consistent with an environment of asymmetric information sharing between physician and patients. When information is shared asymmetrically, partial apologies may signal to a patient that malpractice has occurred.37 This effect is more pronounced for non-surgeons compared with surgeons, because non-surgeons have longitudinal patient relationships rather than discrete clinical encounters.81 For example, if Mr. Doe becomes septic after his surgeon removes his gallbladder, he may wonder if the surgery led to his bad outcome. If Mr. Doe becomes septic during a 10-year relationship with his primary care physician, he is less likely to link this adverse event to a specific instance of malpractice, unless his primary care physician partially apologizes. In a system with asymmetric information sharing, partial apologies may increase malpractice risks, perhaps serving as an apparent signal of potential malpractice coming from non-surgeons.81 It is also worth noting that people engaged in longitudinal relationships are perhaps more invested in the relationship itself and more willing to accept an apology from an erring party to restore this relationship.
One caveat to the analysis by McMichael et al. is that the data collection ended in 2011, not long after the Congressional Health Information Technology for Economic and Clinical Health (HITECH) Act took effect in 2009.82 The HITECH Act included an emphasis on greater utilization of electronic health care record systems, with goals including improved quality of health care, reduced rates of medical errors, and mandated patient access to their electronic health care records.82 In theory, this act increased physician and health care system transparency and represents a meaningful move toward a system of symmetric information sharing. As discussed previously, partial apologies may have their intended effects of emotional relief in a transparent system.
Discussion
Overall, apology laws do not appear to reduce malpractice rates and costs. This inefficacy likely is due to most states having partial apology laws, which do not protect statements that have the desired therapeutic benefits necessary to decrease malpractice rates.24,76,–,78,83 The study by McMichael and colleagues,81 which is restricted to partial apology laws, substantiates this theory. Partial apologies are particularly ineffective in a system with asymmetric information sharing, as in much of the U.S. health care system.
McMichael et al.81 opined that even though partial apology laws do not reduce rates of malpractice, they may have larger societal benefits by encouraging more frequent expressions of empathy. As discussed previously, however, malpractice claims have many significant ramifications for physicians. If partial apologies clearly increase physicians’ likelihood of being sued, it seems unrealistic to expect physicians to provide partial apologies, despite broader social benefits.
There may be a way, however, to allow for the therapeutic and societal benefits of apologies while protecting physicians from increasing their malpractice risk, i.e., by encouraging full apologies. The benefits of full apologies to their recipients are clear.1,–,3 Full apologies are a way of forging the transparency that physicians, patients, ethicists, and regulatory bodies desire.10,–,13,77,84 Full apology laws, which are much fewer in number (currently only present in nine states)31,–,39 and therefore are harder to study effectively, may provide the legal protection needed for physicians to apologize fully more often.
While it is unclear why many states have chosen to pass partial apology laws rather than full apology laws, this may be due to the intuitive reasoning that error admission may incite malpractice claims. Much of the evidence for full apology laws and their effect on malpractice suits is theoretical, based on the communication deficits that spur many malpractice claims and the communication benefits of full apologies. Perhaps more time may provide the data needed to demonstrate the impact of full apology laws on malpractice claims and substantiate this theoretical benefit.
In the meantime, hospital-based disclosure programs, with their promising therapeutic and legal outcomes, may be another such solution. This approach may be more effective given its incorporation of communication training, support for providers during the apology process, financial compensation, and more robust efforts to prevent similar errors from occurring.26,–,30,76 These programs also may provide the communication training and institutional support that are needed for physicians to apologize effectively.76
Greater utilization of full apologies could in turn create a more transparent health care system. In a more transparent health care system, i.e., one with more trust between physicians and patients, perhaps even partial apologies could have their intended therapeutic impact rather than arouse suspicion. There are also larger, less quantifiable consequences to a health care system with mistrust on both sides. Repairing this trust will take time and, perhaps, more apologies.
Conclusion
The therapeutic benefits of apologies are well established. Apology laws aim to harness these therapeutic benefits, with the primary objective of reducing medical malpractice rates and costs. Well-formulated apologies can mitigate communication barriers between physicians and patients, as well as disarm emotional responses that may prompt patients to pursue malpractice lawsuits. Most apology laws are partial apology laws, however, which do not protect the type of information sharing that meaningfully improves physician–patient relationships. Existing apology laws have not had their intended impacts of reducing rates and costs of medical malpractice. Full apology laws are much more likely to improve physician communication and transparency meaningfully and to decrease rates and costs of malpractice suits. The impact of the new 2020 Health and Human Services rule permitting patients full access to their electronic health record also needs to be assessed.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2021 American Academy of Psychiatry and the Law
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵





{kind=link}