


Abstract
Managing and treating physicians with professional boundary violations is of paramount importance with vast implications for public safety. Physician Health Programs (PHPs) evaluate and monitor many, if not most, physicians receiving care for these abuses. We conducted a chart review of 120 physicians monitored for boundary violations. We made intergroup and intragroup comparisons (i.e., examining nonpatient, patient nonsexual, and patient sexual offenses). The violator group as a whole differed from the general PHP population, in that more were men between 40 and 49 years of age. More of the violators were mandated for evaluation and reported an abusive history. The rate of psychiatrists exceeded that typically seen by the PHP. Other differences were found according to the type of violation committed. Post hoc analysis revealed that physician-patients with a history of prior boundary violations were more likely to commit violations of a sexual nature. No further incidents were reported for 88 percent of the cohort.
Understanding and maintaining professional boundaries is essential for all physicians. Whether the practice is in a clinical, administrative, or research setting, boundary management is central to maintaining patient safety. Studies show that between four and nine percent of physicians commit boundary violations, but research varies by methodology, operational definitions, and sampling selection, and such behaviors are thought to be grossly underreported.1,–,4 According to Nadelson and Notman,5 a boundary violation refers to the exploitation of power in the professional relationship, suggesting that a violation occurs when doctors use their position of trust and authority for their own pleasure or benefit (or for the benefit of others). Yet, many researchers argue that personal boundaries are idiosyncratic; varying by personal treatment style, professional role, and situation. Therefore, actions should be judged by the type and context of the behavior.6 For example, many individuals distinguish between boundary violations and boundary crossings, the latter consisting of less severe departures from standard medical practice (such as calling to check with patients at home after they have experienced a particularly difficult week). In some situations, boundary crossings may actually facilitate patient care and are more common and appropriately used in some specialties.7,8 For example, psychiatrists and mental health workers generally practice more emotion-oriented care where treatment is inextricably linked to intimate communication and, therefore, personal phone calls may be common practice for many practitioners. However, a personal call from a gastroenterologist, whose practice style is focused on physical ailments, might be judged as uncommon and questionable.
Situational studies also show a lack of definitional consensus in the medical field. For example, investigations that presented physician participants with various scenarios of boundary transgressions found considerable variation in subjects' interpretation of the events.9,10 The imprecise definition of a boundary violation represents a challenge for the medical community, which struggles to establish a clear understanding of appropriate professional behavior and, consequently, appropriate sanctions for situations when those lines have been crossed. While both the American Medical Association (AMA) and the American Psychiatric Association (APA) have published position statements that formally prohibit sexual contact between physicians and current patients,11,–,13 their stance on other types of behavior is less well defined.
Perhaps because we lack consensus for what constitutes a boundary violation, research studies are often narrow in their definition of a violation.14 By and large, researchers examine only actions involving sexual intercourse or activity and many investigators require that these actions occur between doctors and current patients.15 Some researchers suggest that a broader definition and emphasis on personal characteristics are warranted.16,17 Others argue that when we examine only a narrow range of behaviors, we not only fail to comprehend the fully prevalent boundary transgressions, but we also restrict our ability to create evidence-based practice guidelines and meaningful legal advice.15 Consequently, many physicians are left uncertain about appropriate professional behavior (particularly in specialties that practice, by design, more emotionally intimate care) and may be more vulnerable to avoidable lawsuits.17,18 Moreover, by using a limited definition of boundary transgression, we may not show a full understanding of the impact that more subtle behaviors have on the victim.
Medical ethics research is also hampered by the lack of studies examining treatment and outcome data. Typically, doctors who have committed or have been accused of committing boundary violations present to PHPs. Referrals to PHPs can be either voluntary or mandated, although the reason for such referrals has not been systematically studied. PHPs offer evaluation, long-term monitoring, information, support, and advocacy to doctors with boundary concerns but most do not provide direct client care. Another key characteristic of many PHPs is the development of a formal treatment contract that specifies where the client will present for care, what the monitoring requirements and procedures will consist of, and a detailed listing of the consequences of noncompliance.19 Monitoring tasks conducted by PHPs often include, when appropriate, random drug testing, gathering written reports from a worksite monitor, and obtaining attendance records from required treatment sessions.19,–,21 Because of the PHPs' access to and relationship with physician-clients, the programs present a natural choice for examining the process of monitoring individual outcomes for physicians with histories of these transgressions.
The purpose of this investigation was to examine systematically the scope, treatment, and outcome data for boundary violations addressed by a PHP. We examined both intergroup (i.e., all doctors who presented to the PHP for boundary violations versus the general PHP physician-patient population) and intragroup (i.e., variations in violation actions) differences through a retrospective chart review.
The need for this type of data has far-reaching implications for the medical practice, including litigation and policy concerns. It may prove especially useful for forensic psychiatrists who review such data to make legal assessments, recommendations, and provide expert testimony, whereas the absence of this information makes such tasks extremely difficult. First, how do legal specialists define problematic behavior in the courtroom without clear consensus among physicians, empirical research, or professional medical societies? Second, how does one advise others on risk management and malpractice prevention strategies for events that constitute a considerable portion of legal difficulties among clinicians?22 Finally, how do forensic psychiatrists provide treatment recommendations and determine long-term rehabilitation in the absence of such empirical data?
Methods
Participants
As part of an administrative review, we extracted patient charts for PHP clients who presented with boundary violations between1986 and 2005. We identified 120 such clients, who were physicians (n = 115), medical students (n = 1), and other/unknown (n = 4). We gathered data using either hard copies of physician-client records (for intakes before 2000) or examined computerized records (for intakes after 2000). Because our original methodology was undertaken as an administrative task, the chart review did not include a comparative sample. Therefore, when we decided to examine the data systematically, we pulled a reference group of all Colorado PHP intakes that occurred between 1986 and 2005; we removed the physicians with boundary transgressions from the reference group, which totaled 1,133 clients. The reference group (or general physician population) presented to the PHP for a myriad of reasons such as substance abuse, mood disorder, and stress. We obtained Institutional Review Board approval from the University of Colorado Denver for this study; participant consent was waived.
Setting
All clients were monitored by a single PHP in Colorado. The Colorado PHP establishes monitoring requirements for clients on a case-by-case basis, rather than using standardized contracts. The evaluation phase involves the completion of an electronic intake tool that gathers information such as patient history and assesses mental and physical functioning, substance use, and legal history. Clients also meet with a clinician for an in-person evaluation. This information is used to determine the necessity of treatment and, if appropriate, to formulate a treatment and monitoring plan. Often an initial diagnosis is made at this point, although the diagnosis can be modified at any point during the monitoring period. After the Colorado PHP creates a treatment contract, clients are referred to an external facility for treatment, but physicians continue to meet with the PHP to ensure that they are adhering to the terms of their contract. Failure to do so may result in reports to the state medical board and employers.
Type of Transgression
To understand subtle variations in transgressions for intragroup comparisons, we examined the data by three types of violation categories: nonpatient violations, patient nonsexual violations, and patient sexual violations. Nonpatient violations consisted of sexual harassment of coworkers, overinvolvement or romantic relationships with staff, and prescribing for nonpatients. Patient nonsexual violations included misprescribing narcotics to patients, inappropriate behavior during examinations (e.g., having no attendant present, kissing a scar, or being overly interested in the patient), or dual relationships (i.e., multiple roles between a therapist and a client, such as having friends, employees, or students as patients).23 Sexual violations included sexual intercourse with current or former patients or sexual activity, but not intercourse, with current patients. Violation categories were determined by a panel of experts at the health program, all of whom had several years of experience in evaluating such behavior and treating physicians with these types of behavior. A post hoc analysis was conducted to determine whether sexual violations (e.g., sex with a patient or coworker or sexual harassment) differed in frequency from nonsexual violations (e.g., prescribing for nonpatients).
We used both descriptive and inferential statistical techniques to examine the data: chi-square tests for categorical data and t-tests for continuous data. Results were considered to be statistically significant at p ≤ .05. We used SPSS software for all analyses.
Working Definitions
There are several terms in this article that are important to define. Diagnosis refers to a mental health diagnosis as described in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR).24 Client diagnosis was made by an experienced mental health professional at the PHP and was based on patient history, standardized assessment tools, and an in-person interview. Because the diagnosis could be altered during the course of monitoring, we used the most current judgment at the time of analysis. Further violation refers to any behavior that constitutes a boundary violation (see Type of Transgression). A further violation would occur during the monitoring period but after the initial infraction that prompted presentation to the PHP. We had access to this information only during the monitoring period, which averaged 713 days. Further violation incidents were based on several sources, including medical board, workplace, and self-reports. Intergroup comparisons refer to contrasts between the violator group and the reference group, whereas intragroup comparisons refer to contrasts between the types of violations (nonpatient, patient nonsexual, or patient sexual) engaged in by physicians who presented with boundary violations.
Results
General Descriptive and Intergroup Comparisons
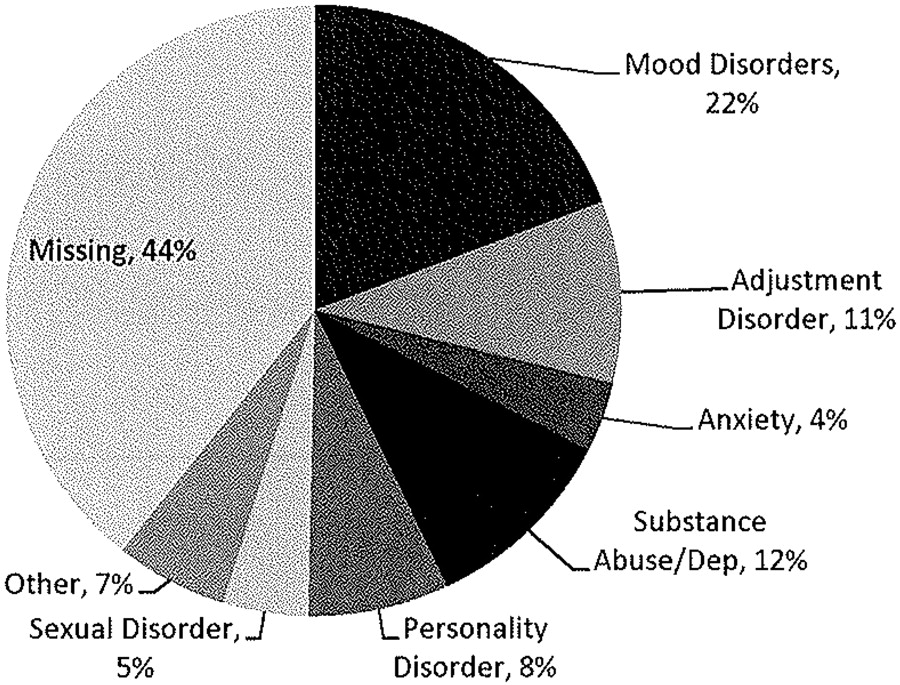
Compared with the general Colorado health program population, those presenting with boundary violations differed in several demographic areas. Of the 120 with boundary violations, 93 percent were men. This proportion differs significantly from our typical client base, in that far fewer (69 percent) were men (χ2 = 27.619; df = 1; p < .000). Most violators were between the ages of 40 and 49 years (48% of the sample), higher than the health program's general population, in which 33 percent fell into the 40- to 49-year-old age range (χ2 = 9.778; df = 4; p < .002). Approximately 63 percent of the offenders were married, a similar number between groups. Boundary violations varied by specialty, with psychiatrists representing the greatest percentage of violators, followed by family practice and internal medicine doctors (18% and 15%, respectively). The psychiatrists represented a higher percentage than we normally see at the health program (22% versus 7%; χ2 = 32.401; df = 1; p < .000). More physicians presenting with boundary violations were mandated for evaluation (χ2 = 5.422; df = 1; p = .020) and reported a history of childhood abuse (sexual or physical; χ2 = 4.039; df = 1; p = .044) (Table 1). Diagnoses varied considerably among physicians with boundary violations, although problems with mood disorders, adjustment disorder, and substance dependence/abuse were most common (see Fig. 1 for a breakdown of diagnoses). Because of data inconsistencies between files, we could not make statistical comparisons of diagnostic frequencies; however, the aforementioned disorders were also the most frequently recorded in our general client population.
Participant Characteristics

Violator diagnoses. (Note that diagnostic frequency is greater than 100 percent due to multiple diagnoses.)
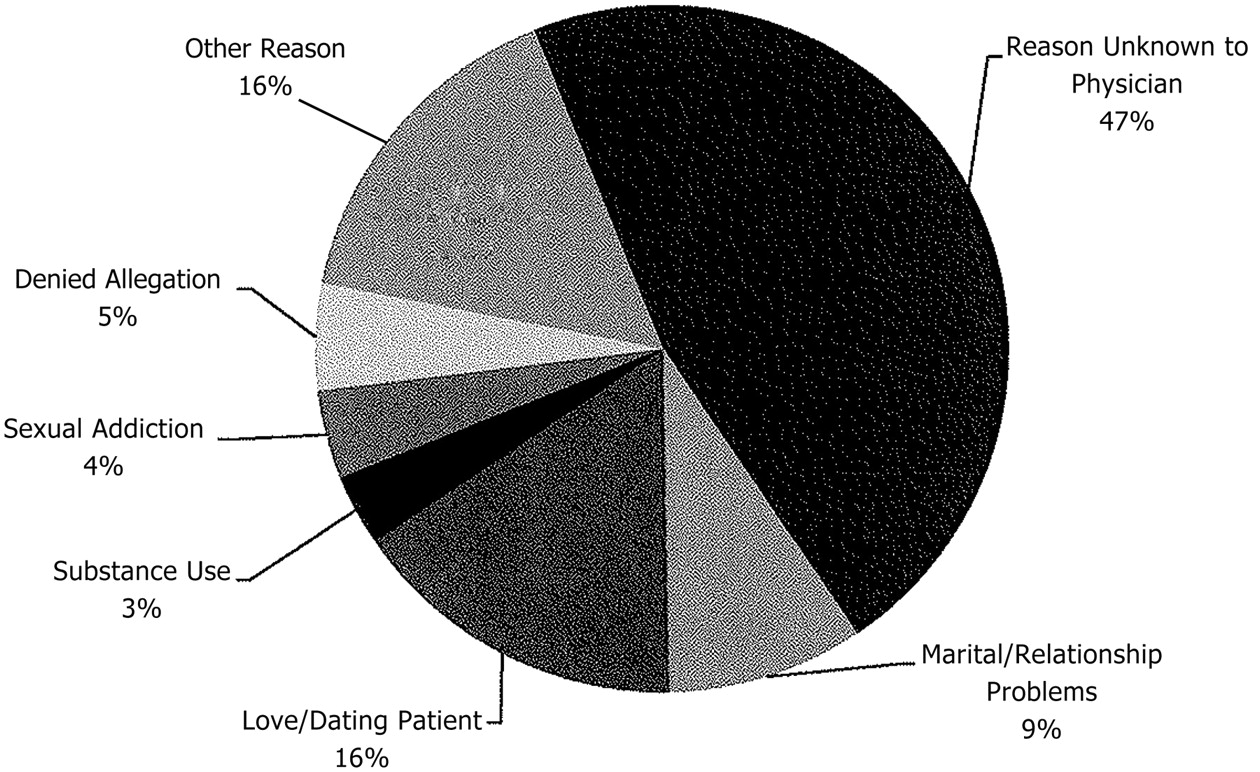
To understand circumstances that potentially contribute to boundary violations, we reviewed self-reports of previous transgressions (i.e., before the current episode) among the group of violators, and approximately 18 percent had reported some type of prior incident. Table 2 shows the distribution of different types of current violations. We found that prescribing violations constituted the most frequent type of transgression (25%), followed by sexual intercourse with a former patient (14%) and sexual intercourse with a current patient (11%). In addition, we examined the reasons that clients cited as the causative agent. Many physicians reported that they did not know why the transgression occurred, and about 16 percent said that they were in love with or dating the patient (Fig. 2).
Violation Categories
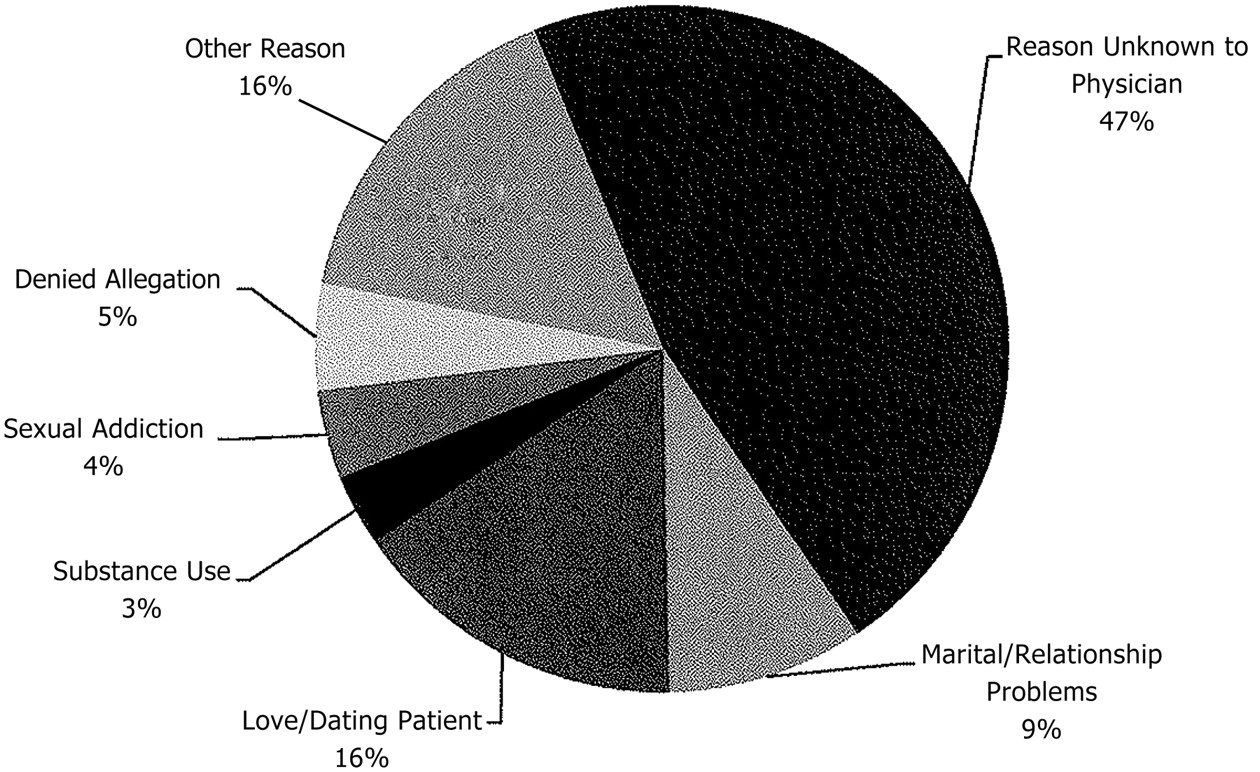
Physicians' explanations for violation.
Intragroup Differences: Violation Categories
As previously described, we were interested in determining differences among the violators by examining the types of violations committed: nonpatient, patient nonsexual, and patient sexual. We found that nonpatient violations were the most commonly reported type, followed by patient sexual and patient nonsexual violations (38%, 34%, and 28% respectively). Within each of these categories, the specific nature of the boundary violation varied widely. Among nonpatient violations, most physicians presented for prescribing offenses, followed by sexual harassment and other miscellaneous complaints. Among patient nonsexual violations, most complaints were due to inappropriate behavior during an examination, followed by dual relationships and nonsexual romantic relationships. Sexual intercourse with a former patient, followed by sexual intercourse with a current patient, included the majority of cases in the patient sexual violation category (Table 2).
There are several sources of referrals to PHP evaluations. Physicians who had engaged in patient sexual violations were often referred for evaluation by the state medical board, peers, or attorneys, and some were self-referrals. Nonpatient offenders tended to be referred for evaluation by the state medical board, administration, peers, and hospitals (Fig. 3). There were no significant differences between voluntary and mandatory referrals by violation category.
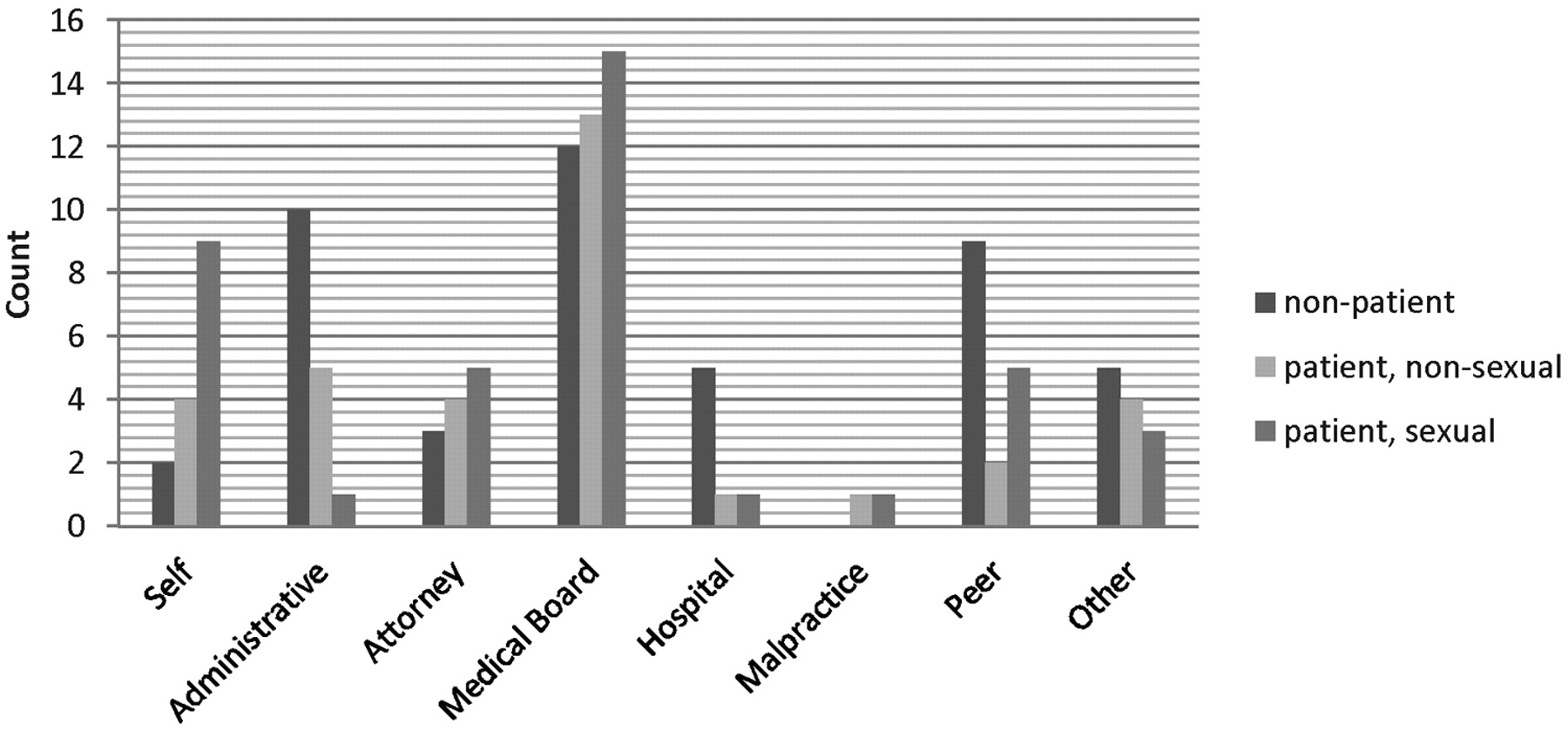
Sources of referral to the PHP program.
Significantly more legal actions were taken against physicians who presented for patient sexual violations (χ2 = 20.744; df = 2, p = .000) than for nonpatient or patient nonsexual violations. Between 83 and 90 percent of physicians reported no further violations (according to the physician or external monitoring sources) at follow-up. Current license status (e.g., clear, probation or revocation, and lapsed) did not differ between groups, and a large majority (85% or more) had an active and unrestricted license at the time of intake (Table 3). There was no difference in license status between clients who were mandated for evaluation and those who presented voluntarily. The average length of monitoring by the PHP was nonpatient, 658 days; patient nonsexual, 547 days; and patient sexual, 950 days); however, for patients with either a sexual disorder or substance use disorder, the duration of monitoring spanned up to 4 years. (Because of the low number of patients in these categories, we did not run significance tests.) Monitoring duration did not differ significantly between groups, perhaps because of the high degree of data variability, and was unrelated to mandatory versus voluntary referrals.
Violation Consequences
Post Hoc Analysis: Sexual Violations
We conducted a post hoc analysis to determine whether the frequency of sexual violations differed from that of nonsexual offenses. We found that most violations (59%) were sexual, although they did not necessarily consist of intercourse (e.g., sexual harassment, sexual comments, or sexually explicit discussions with coworkers or patients). However, it is worth noting that 41 percent of violations were not sexual. We found that physicians who reported a history of any type of prior boundary violations were more likely to present for sexual violations as the current offense (χ2 = 4.604; df = 1; p < .032). Offenders who committed a sexual offense were no more likely to report further violations and did not have more restrictions on their medical license than did those who committed a nonsexual violation.
Discussion
This is the first longitudinal and most diverse examination of boundary violations committed by physicians who presented to a PHP and offers insights not previously published. One key finding is the existence of several demographic differences between the group of physicians presenting for boundary violations and the general PHP clientele. Boundary violators tended to be older men who were mandated for evaluation. More violators also reported a history of childhood abuse. This and other studies found that psychiatrists are more likely to present for a boundary violation than physicians in other specialties.3 Because of the nature of the therapeutic relationship, it is predicted that psychiatrists will have relationships with their patients that are more personal or intimate and that may, in turn, leave them more vulnerable to the blurring or crossing of a variety of boundaries, either as a result of that intimacy or in the name of less traditional treatment. For many psychiatrists, there is a wide range of behaviors for which appropriateness is unclear.25 Because of this uncertainty, careful professional consideration should be exercised when defining boundary crossings, specifically, and boundary violations in general. Some authors suggest that sexual violations follow a predictable progression of behavior among physicians.15,26 We saw evidence that partially supported this theory, finding that doctors who committed a sexual violation reported significantly more previous violations of other types. Epstein and Simon27 created a self-assessment questionnaire that allows therapists to gauge their own potential for violating patient boundaries. Although this measure has not been widely adapted or reviewed, it is interesting to ponder whether such a tool can determine a physician's risk of violations before an offense or enhance treatment and monitoring by PHPs.
Too often, boundary violations are thought of as largely sexual offenses, at least by the lay public.28,–,31 A second result of this investigation was the identification of a wide variety of boundary violations, ranging from prescribing offenses to dual relationships with various degrees of sexual misconduct. We believe that this demonstrates the importance of exploring the diversity of boundary violations and potential differences in evaluation, contracts, and monitoring by the PHPs. Because this study was initially conducted as an administrative task, we did not gather information about differences in PHP care between violation categories. Further study should incorporate this information to understand and apply appropriate monitoring standards to PHP clients, as well as to inform medical professional policy.
A final result that stood out in this investigation was that outcomes for physicians presenting for boundary violations are generally good, with 88 percent of doctors (and supplemental reports) reporting no further boundary violations. This absence of relapse is true of sexual violations as well as the other categories. The idea that physicians can complete treatment without further incident has been argued by other authors, who note that rehabilitation is more common for physicians accused of sexual boundary violations than not.32 Although it is possible that physicians underreport additional violations for fear of further legal and professional retribution, our monitoring program incorporates long-term follow-up reports from multiple agencies and corroborations by different sources and thus is generally thought to be accurate. This conclusion should be viewed with caution, however, as further violations could occur after the physician completes monitoring at the PHP and therefore may not be recorded in the medical record.
There is information presented here about long-term monitoring of physicians who are currently or have been accused of committing boundary violations. Across violation categories, the duration of monitoring did not vary significantly, although monitoring appeared to be longer for physicians diagnosed with sexual or substance use disorders. This finding should be further explored with a larger sample.
It is important to note that our study utilized retrospective data with a relatively low sample size. This limited our ability to examine the results in more detail, and several statistical comparisons were not possible due to the low number of participants in each category. Moreover, the amount of missing data in the physician diagnostic category was high, about 44 percent. Although outcomes were good across violation groups, the high risk that boundary violations pose to patients and the general medical profession warrants caution and further study.
Conclusions
The information presented in this report is helpful for better understanding of boundary violations, boundary crossings, and appropriate professional behavior and can be used to facilitate further discussion. The results provide more evidence-based understanding about the nature and scope of boundary transgressions, information that is particularly important as the medical community struggles to formulate clear definitions and guidelines in this murky and controversial area. As we improve our awareness of boundary violations, we are better able to develop a professional consensus on such behaviors and thus, create appropriate policy, legislation, and risk management advice on the basis of sound research data.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2012 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}
{kind=link}