


Abstract
Ethanol abuse can lead to negative consequences that oftentimes result in criminal charges and civil lawsuits. When an individual is suspected of driving under the influence, law enforcement agents can determine the extent of intoxication by measuring the blood alcohol concentration (BAC) and performing a standardized field sobriety test. The BAC is dependent on rates of absorption, distribution, and elimination, which are influenced mostly by the dose of ethanol ingested and rate of consumption. Other factors contributing to BAC are gender, body mass and composition, food effects, type of alcohol, and chronic alcohol exposure. Because of individual variability in ethanol pharmacology and toxicology, careful extrapolation and interpretation of the BAC is needed, to justify an arrest and assignment of criminal liability. This review provides a summary of the pharmacokinetic properties of ethanol and the clinical effects of acute intoxication as they relate to common forensic questions. Concerns regarding the extrapolation of BAC and the implications of impaired memory caused by alcohol-induced blackouts are discussed.
Without question, ethanol is the most common psychoactive drug used by children, adolescents, and adults in the United States and is one of the most abused drugs in the world.1 Its use has long been associated with criminal and civil litigations.2,–,4 Alcohol abuse can lead to a wide range of adverse health outcomes, economic burdens, and social consequences.5,–,9 Alcohol consumption continues to be a public health concern because of its association with adverse social impact including domestic violence, child abuse, fires, accidental injury, and traffic deaths.10,–,14 Other crimes against individuals such as robbery, assault, and rape are commonly associated with the misuse of alcohol.15 Over the past century in the United States, the laws and policies implemented to promote the moderate and safe use of alcohol also carry with them a large number of legal consequences. From a forensic standpoint, the measurement of blood alcohol concentration (BAC) is primarily used to determine the extent of intoxication. Thus, understanding the pharmacokinetic properties of ethanol is crucial in determining its role in criminal litigation. In this article, we review the pharmacology of ethanol in adults that has relevance to the common forensic questions that arise during depositions and trials.
Measurement
BAC is measured according to various metrics, leading to confusion. The percentage or gram percent alcohol measurement actually indicates grams per 100 mL of a body fluid, usually the blood (i.e., the BAC). Thus a BAC of 0.08%, the most common BAC indicator for driving under the influence (DUI) of ethanol, is equivalent to 0.08 gm%, 0.08 gm/100 mL, 0.08 gm/dL, 80 mg%, 80 mg/dL, and 17.4 mmol/L (800 mg/L divided by 46.06844). The conversion to 17.4 mmol/L is made because 1 mol of ethanol is equivalent to 46.06844 g. The chemical formula for ethanol is CH3CH2OH, and the molar mass of the carbon, oxygen, and hydrogen is 12.0107 g/mol, 15.9994 g/mol, and 1.00794 g/mol, respectively.
Pharmacokinetics
Absorption, distribution, metabolism, and elimination are the common pharmacokinetic parameters used to characterize drug bioavailability in the body.
Absorption
Ethanol is effectively absorbed through the gastrointestinal (GI) tract. Factors that influence absorption include the presence of food, the rate of gastric emptying, ethanol concentration, the type of alcoholic beverage consumed, and changes in GI motility and blood flow.16,–,27 Because of the high water solubility and low molecular weight (MW = 46) of ethanol, ∼20 percent is absorbed from the stomach into the blood by passive diffusion, whereas the remainder is absorbed primarily in the proximal portion of the small intestine.28 Ethanol is absorbed slowly in the stomach and rapidly in the small intestine because the absorbing surface area of the stomach is small relative to the jejunum, such that the rate of gastric emptying functions as the gatekeeper for the rate of absorption.16,29 Logically, it follows that the presence of food in the stomach can delay gastric emptying and decrease the rate of ethanol absorption. Caloric density and composition of a meal influence the rate of gastric emptying.20 Food or fluid in the gastric lumen dilutes ethanol concentrations and reduces the efficiency of absorption.18 A U.S. Food and Drug Administration (FDA)–defined light breakfast of 4 oz orange juice, a slice of buttered toast, and a cup of coffee decreased the average area under the blood alcohol time curve by 36 percent, whereas a heavy breakfast of 4 oz orange juice, 2 fried eggs, 2 strips of bacon, 2 pieces of buttered toast, and 2 cups of coffee resulted in a 63 percent reduction. The decrease was estimated to be equally a function of slowed absorption.21 A later study demonstrated that in nonfasted individuals, protein meals decreased alcohol absorption by 77 percent, whereas fatty meals decreased absorption by 90 percent and carbohydrate by 96 percent.22 Solid meals delay gastric emptying more than liquid meals; therefore, the rate of absorption with solid foods is slower than with liquid foods.23 Ethanol concentration and the type of alcohol consumed also affect the rate of GI absorption and peak BAC. In the fasting state, dilute alcoholic beverages such as beer or wine are absorbed more slowly than higher concentration beverages such as whiskey or vodka and tonic.17,26 The caloric content and nonalcoholic ingredients of beer and wine contribute to delay in gastric emptying and can influence the rate of GI absorption.27
Distribution
Ethanol is completely miscible in water and insoluble in fat. The volume of distribution (Vd) for alcohol in an individual is an expression of total body water.30 The Vd for alcohol is proportional to the lean body mass because the adipose tissue contains little water. On average, women have more adipose tissue than men, and therefore, they have a smaller Vd.31 Thus it is not surprising that the Vd of alcohol in the body is approximated to that of total body water (TBW). Because ethanol distributes almost entirely in the TBW compartment, the Vd of ethanol is influenced by the proportion of fat versus lean body mass. Mean values for Vd of 0.7 L/kg for males and 0.6 L/kg for females were determined by Widmark in the 1930s.29,32,33 These values are often used in legal BAC calculations (i.e., the Widmark BAC estimation equation (see equation 1)), but BMI and body composition have changed considerably over the years. Increasing BMI results in decreased Vd of ethanol, therefore the original Widmark mean values may not be appropriate estimates of ethanol distribution for the current population and may not be suitable for calculating BAC in obese patients.34 Methods to individualize measures of ethanol distribution involve calculating TBW based on gender, height, and weight.33 In adult males, the average TBW is estimated at 61 percent of total body weight while in adult females, the best average estimate of TBW is 50 percent.35 Postmortem samples are often obtained from tissue other than whole blood and thus require adjustment to standardize the ethanol concentration into BAC units. Table 1 presents the distribution ratios of ethanol in body fluids and tissues relative to whole blood.36
Distribution of Ethanol in Body Tissue and Fluid Compared With Blood
In the United States, one “standard” drink contains ∼14 g pure alcohol.37 Examples of a standard drink are: 12 ounces of regular beer (usually ∼5% alcohol), 5 ounces of wine (typically ∼12% alcohol), and 1.5 ounces of distilled spirits (∼40% alcohol).37 An important caveat about generalization is that most microbreweries have lagers and ales with labeled alcohol percent concentrations that exceed these percentages. The potency of distilled spirits is characterized in terms of proof. For instance, 86 proof whiskey contains 43 percent (volume percent) absolute ethanol, whereas 100 proof vodka is 50 percent ethanol.
Blood Alcohol Calculations
Generally, it is estimated that one drink will produce a BAC of 0.02 percent for a 200-lb male and 0.04 percent for a 125-lb female, whereas two and three drinks double and triple the BAC, respectively. Thus, it should be assumed that the number of drinks and the BAC they produce increase linearly, as commonly presented in drink–BAC tables available on the Internet.
To estimate expected BACs from drinking histories, the Widmark and Watson equations are commonly used.32,33 The Widmark formula is shown in Equation 1:
 where A equals the amount of ethanol consumed in milliliters, W equals the weight of the subject in kilograms, and r is the Widmark factor, a constant relating the distribution of water in the body in liters per kilogram. Table 2 lists the Widmark factors for men and women by height and weight, calculated according to the Forrest method.38,39 The procedure proposed in Forrest's paper for calculating the Widmark factor is labor intensive if performed manually, and the BASIC computer program offered by the author is no longer available.38 The Widmark Factor can also be calculated by taking the TBW and dividing by the percentage of water in the blood (80%).
where A equals the amount of ethanol consumed in milliliters, W equals the weight of the subject in kilograms, and r is the Widmark factor, a constant relating the distribution of water in the body in liters per kilogram. Table 2 lists the Widmark factors for men and women by height and weight, calculated according to the Forrest method.38,39 The procedure proposed in Forrest's paper for calculating the Widmark factor is labor intensive if performed manually, and the BASIC computer program offered by the author is no longer available.38 The Widmark Factor can also be calculated by taking the TBW and dividing by the percentage of water in the blood (80%).
Widmark ‘r’ Values by the Method of Forrest
For example, in the case of a 32-year-old man (height 195 cm, weight 100 kg) who drinks one beer (14 g alcohol, 12 fluid ounces), the BAC can be calculated by first determining the Widmark factor from Table 2 and then using Equation 1. A typical bottle of beer contains 12 ounces of liquid and is 5 percent alcohol, so it contains 0.6 liquid ounces of alcohol (A = 17.74 mL). The Widmark factor according to Table 2 for this individual is 0.7 L/kg.

Hence, the estimated BAC from the Widmark formula for this example is 0.0203 percent.
The Watson formula requires an estimate of the subject's total body water (TBW). The formulas for TBW in males and females, respectively, are presented in Equations 2 and 3, where TBW is in liters, height is in centimeters, and weight is in kilograms. Equation 4 presents the Watson formula where A is the amount (in grams) of ethanol ingested and 0.8 is the fraction of water in the blood.



Calculating BAC using the Watson formula for the same individual (a 32-year-old man, 100 kg, 195 cm) requires determination of TBW from Equation 2 first. Then, the TBW can be used in the Watson formula.

The TBW for this example is 54.86. The approximate BAC, therefore, using the Watson equation is 0.0259 percent.
Elimination
Ethanol absorption and distribution throughout the body are not instantaneous. However, once absorbed, elimination begins. About 95 to 98 percent of ingested ethanol is metabolized.29 It is metabolized in the liver first by the enzyme alcohol dehydrogenase to acetaldehyde and then by the enzyme aldehyde dehydrogenase to acetic acid, which dissociates to carbon dioxide and water.30,40 The initial analyses to determine the rate at which ethanol is eliminated from the body assumed the drug followed the laws of capacity-limited elimination (Michaelis-Menten model). These analyses typically determine a maximum ethanol metabolic capacity (Vmax) of approximately 8,500 mg/hour per 70 kg.40 Thus, the expected blood ethanol disappearance rate (BEDR) is 8,500 mg/70 L per hour or 121 mg/L per hour (0.012%/hour). Taking into account the results of 8 studies with 425 subjects, the BEDR weighted average and standard deviation were calculated as 0.0155 percent ± 0.0029 percent/hour.40 For 95 percent of the population, the BEDR ranges from 0.010 to 0.022 percent/hour. Thus although ethanol is eliminated from the body at a fixed rate, it does not appear to obey the classic Michaelis-Menton pharmacokinetic rules of capacity-limited elimination.
Despite conflicting evidence, one controlled study of 8 ethanol-abstinent individuals found that daily administration of ethanol for one month increased their rate of elimination by as much as 72 percent. This effect appears to be related to activation of ethanol-metabolizing liver enzymes by chronic ethanol exposure.41 Studies have also found that women metabolize ethanol 13–22 percent faster than men. However, women have a 9–14 percent smaller volume of distribution, which cancels out the faster metabolism effect, such that men and women have similar BEDRs.30
Several studies have investigated the effect of food on alcohol elimination rates and found that consuming a meal increases first-pass metabolism and the disappearance rate.42,43 Because these studies used oral alcohol administration, the effects of food on alcohol absorption confounded the effect of food on the elimination rate. Intravenous infusion of ethanol with breath alcohol clamping has been used as a method of direct measurement of BEDR. Ramchandani et al.19 used this method to study the effects of food and food composition on BEDR and found that the rates of elimination increased by 25 to 45 percent in the fed state compared with the fasted state. There was no observed difference in BEDR among different types of food, suggesting that intake of food was sufficient to increase the elimination rate of alcohol, made possible by the increase in hepatic blood flow or activation of ethanol-metabolizing enzymes.
Probability Estimates
The extrapolation of BACs involves a degree of uncertainty. For example, the clearance rate used in BAC calculations is 0.0155 percent ± 0.0029 percent (average value ± standard deviation, i.e., degree of uncertainty). The best estimated BAC at the time of a crime is based on the mean value, and there is a certain amount of error based on the confidence interval. It would be helpful to know, given a particular degree of uncertainty in estimating, with what degree of confidence the individual could be said to be above the threshold of 0.08 percent. If the calculations demonstrated a 95 percent probability (±2 SD) versus a 68 percent probability (±1 SD), clearly the former presents a stronger argument for legal intoxication. Normal distribution, the cornerstone of modern statistics, can be used to estimate these probabilities and provide perspective on BAC calculations. Since threshold concentrations of BAC have legal implications, the use of probabilistic statements is often appropriate. For example, after a motor vehicle accident the Breathalyzer measurement of BAC at the police station, taken 2 hours after the accident, is 0.07 percent. The obvious information a jury needs to know is what the BAC was estimated to be at the time of the accident. Thus, the expert at trial can testify that there is a 50 percent probability that the BAC at the time of the accident was 0.101 percent (0.07% + [0.0155% · 2 hour]); a 68% probability (±1 SD) that the BAC ranged from 0.0952 percent to 0.1068 percent (0.07% + [0.0155%–0.0029%] · 2 hours to [0.0155% + 0.0029%] · 2 hours); and a 95 percent probability (±2 SD) that the BAC ranged from 0.0894 percent to 0.1126 percent (0.07% + [0.0155%–0.0029%] · 2 hours to [0.0155% + 0.0029%] · 2 hours).
In 2009, the National Academy of Sciences released a report aimed at addressing improvements in forensic science and acknowledged the need for measures of certainty when determining levels of BAC in an individual.44 Reporting single numerical values of BAC without recognition of the variability in pharmacokinetic parameters or of the error associated with calculations could be considered an obstruction of truth and justice. After the release of the report, the courts ruled that breath and blood test results without determined confidence intervals were not admissible under Evidence Rule (ER) 702. The courts also found that introduction of a single test value as evidence, without stating a confidence interval, would be a violation of ER 403 and therefore inadmissible in such cases.45
To extrapolate BAC with certainty, a range of physiological parameters that affect the ethanol rate of absorption, distribution, and elimination have to be identified. Uemura et al.,46 found individual differences in absorption rate constants (Ka) to range from 1 (slow absorption) to 8 (fast absorption).46 Distribution in terms of TBW can be calculated by using a range of methods.33,39,47,48 Elimination rates of alcohol from blood were found to range from 0.010 g/dL per hour to 0.035 g/dL per hour (0.01–0.03%/hour).49 Equation 5 presents the modified Widmark formula where A is the amount of ethanol (in grams), 0.80 is the fraction of water in the blood, TBW is the volume in liters, β is the ethanol elimination rate per hour, and t is the time since start of drinking (in hours).33,50 By incorporating the physiological range of values into the modified Widmark formula, extrapolation and interpretation of BAC values can be determined with greater certainty51:

Thus, based on the above calculation for a 170-lb, 68-in, 30-year-old man who ingested three 12-fl-oz beers containing 5 percent ethanol and whose BAC at time zero was estimated to be 0.074 percent, it can be said with 95 percent (i.e., ±2 SD) certainty that his BAC two hours after he stopped drinking would range from [(0.074%) − (0.03% · 2 hours)] = 0.014 percent (lower limit) to [(0.074%) − (0.01% · 2 hours)] = 0.054 percent (upper limit).
“One-for-the-Road” Estimations
One question occasionally arises in back-extrapolation of alcohol concentrations in the one-for-the-road situation. That is, an individual consumes a quantity of alcohol immediately before leaving a drinking situation and has an accident shortly thereafter. If absorption of the last drink was not complete at the time of the accident, but is considered in the BAC calculated sometime later, extrapolation to the time of the accident is artificially elevated. As described by Jones52:
If circumstances suggest that the BAC was rising at the time of offense, e.g., if an accident occurred within about 15 min after the end of bolus dose consumption, back extrapolation is not possible. One solution to this problem is to make an allowance for the maximum expected BAC increment from the time of the traffic incident to reach the peak.
The time to peak after the ingestion of beer on an empty stomach has been described in several studies, providing a reasonable estimate of 40 minutes.17,52,53 Alternatively, the time to peak for beer with co-ingestion of food is shorter and estimated to be ∼16 minutes.52,54 If the accident occurred between the time the last drink was consumed and the estimated time of peak BAC, back-extrapolation should stop at the time of peak BAC. This percentage would represent the maximum estimation of the BAC at the time of the accident.
Clinical Effects
Ethanol is an odorless liquid. However, there is an odor that is commonly associated with ethanol ingestion. The smell results from the fruity aroma of the fermented original material used to produce the ethanol such as malt, hops, or grapes. The odor persists in the body tissue, on the breath, and in sweat for several hours after the ethanol has been metabolized. Thus, in a person, the odor is not necessarily a proxy for intoxication. Before the onset of liver damage, the BEDR in alcoholics is calculated to be 0.0249 percent ± 0.0049 percent.55 When asked to estimate BAC at the time the crime was committed, it is important to assess in the alcohol-intoxicated subject whether the person is a social drinker or an alcoholic with normal liver function. However, once liver damage is obvious, patients with a diagnosis of alcoholism become less tolerant of the effects of ethanol as the number of years of heavy drinking increases, because the liver has declining metabolic capacity.
Social drinkers are classified as unimpaired, impaired, or intoxicated.56 A drinker is defined as unimpaired when he or she has shown little or no loss of ability. There is minimal risk of accidents or injury under this classification. BACs are usually less than 0.04 percent, and no clinical signs are observed. Drinkers with impaired function may exhibit some loss of functional ability. They can be legally served ethanol and can perform activities that involve potential risk. Impaired BACs range from 0.04 to 0.08 percent. Clinical signs of impairment include the following: skin warm to touch, flushed face, bloodshot eyes, sweating, loosened clothing, relaxed demeanor, slow movement, poor coordination, exaggerated gestures, out-of-the-ordinary behavioral symptoms (flustered, forgetful, giddy, clumsy, overly friendly, mild profanity, and speaking loudly and dominating conversation), difficulty articulating speech, miscalculating distance or depth, and making physical contact when talking. Intoxicated individuals exhibit greater loss of functional ability, are at risk of injury, and should not perform activities that involve potential risk. While intoxicated, the individuals cannot be legally served alcohol. BACs associated with being intoxicated are usually more than 0.08 percent. Clinical signs include slurred or incoherent speech, fumbling, extreme lack of dexterity, sloppiness, loss of balance, stumbling, antisocial speech or behavior, and shouting or cursing at people and other hostile behavior. Table 3 correlates BACs with signs of impairment or intoxication.
Correlations of BAC to Intoxication
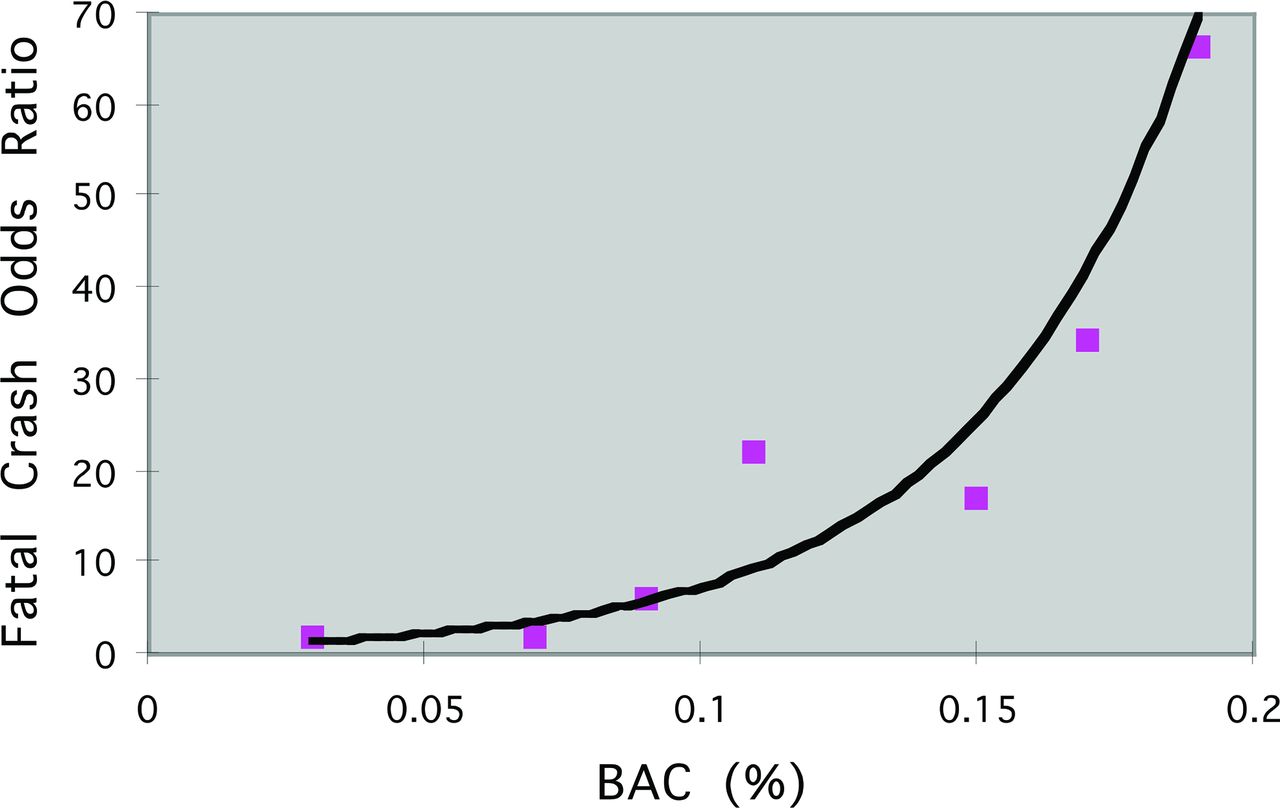
The probability of being responsible for a fatal crash increases exponentially with a rising BAC. Figure 1 presents this relationship. At a BAC of 0.07 percent, the risk of being involved in a fatal crash is ∼1.5 times greater than normal, whereas at a BAC of 0.09 percent the risk increases significantly to about 6 times greater than normal. In addition, the odds ratio for being involved in a crash increases significantly at a BAC of ∼0.05 percent.57 Currently, all U.S. states specify a BAC of 0.08 percent as the cutoff for operating a motor vehicle under the influence of ethanol.58 Because of the rising concern about alcohol-related motor vehicle crashes involving people under the age of 21, all states have adopted zero-tolerance laws for underage drinking that make it a criminal offense if drivers under the age of 21 are found to have a BAC between 0.00 and 0.02 percent.59,60 While legislation has helped to establish BAC limits over the past 30 years, nearly 31 percent of all traffic-related deaths (10,076) in 2013 involved an alcohol-impaired driver with a BAC of 0.08 percent or more.61
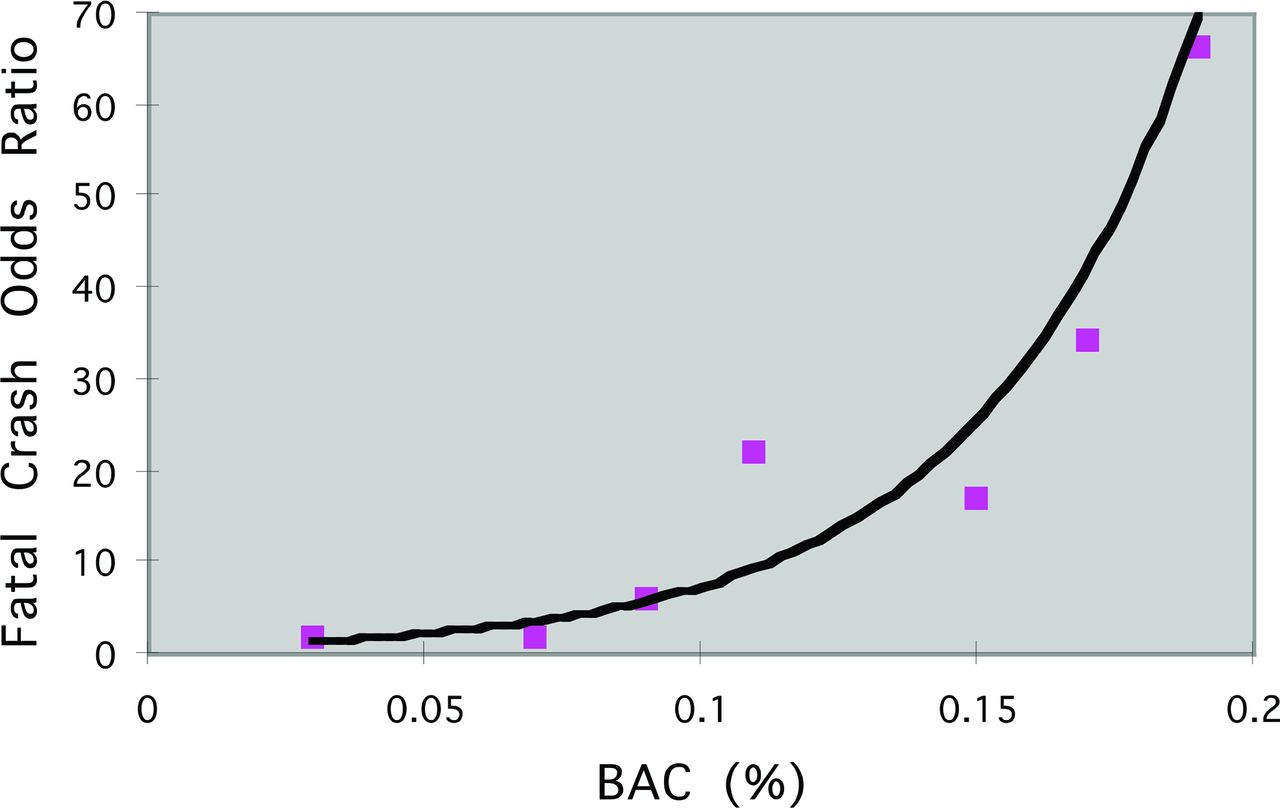
Relative probability of being responsible for a fatal automobile crash increases with rising BAC.
Assessment of Intoxication
The alcohol field sobriety test originated from the work of Goldberg.28 He found that the results of six neurologic and mental status examination tests linearly correlated with subjects' steady-state BACs. These included the critical flicker fusion, the corneal reflex test, the modified Romberg test, the finger-to-finger test, the serial subtraction test, and the selective-attention task test.
Sensory Perception
The critical flicker fusion (CFF) determination test has a subject observe a flashing light. The frequency of flashes is increased or the intensity of the light is decreased until the subject reaches the “blur point” and is unable to perceive discrete flashes. The CFF is lowered after drinking a moderate dose of alcohol.62 The corneal reflex test provokes the closure of the eyelids by touching the conjunctiva. The required intensity of the stimulus, a puff of air to precipitate the corneal reflex, increases with rising BAC.28
Motor Coordination
The standing-steadiness test is a modified Romberg test. The subject stands with the feet together and eyes closed. The amount of body sway increases with rising BAC. In the original finger-to-finger test, a cardboard disk is attached to one finger and a pointed thimble attached to the opposite finger. With arms extended, the subject brings the forefingers together repeatedly producing dots on the disk. The area of dots increases proportionally with rising BAC.28
Intellectual Functioning
The serial subtraction test asks the subject is to subtract 7 from 100 without the benefit of pencil or paper and then subtract 7 from the subsequent result for a total of five problems. The accuracy of this test of immediate or acquisition memory and concentration diminishes with increasing BAC. Finally, performance on a selective-attention test (e.g., subject is asked to read a paragraph and circle each occurrence of the letter R) is adversely affected by rising BAC. For both of the intellectual-functioning tests, the variables of test speed (decrease) and number of errors (increase) vary directly with an increase in BAC.28
These tests constitute the origin of the field sobriety test employed by law enforcement agencies across the United States. Table 4 provides a description of 14 objective and subjective parameters used by law enforcement officers to estimate sobriety in the field.63 Of these 14 assessments, 3 are currently included as assessment tools for the Standardized Field Sobriety Test (SFST) used by law officers to evaluate a subject's level of alcohol intoxication. The three tests are horizontal gaze nystagmus, walk and turn, and the one-leg stand. The original research demonstrated a high correlation between failure of the SFST and a BAC >0.08 percent. However, the researchers did not use a control group to validate that failure in performing the SFST differentiates alcohol-intoxicated subjects from sober individuals. Yoshizuka et al.64 administered the SFST to 185 sober subjects and determined that 26 percent of the drug-naïve subjects failed the test. Because the SFST is used as evidence of probable cause to justify an arrest for driving under the influence of alcohol and of other central nervous system–affecting drugs, as well, its validity for accurate identification of subjects driving under the influence of drugs such as cannabis, barbiturates, benzodiazepines, cocaine, amphetamines, and opiates remains to be established.64
Parameters Associated With a Typical Field Sobriety test
Alcohol-Induced Blackouts
Several types of memory loss can accompany the use of alcohol. A true alcoholic blackout has a starting point, is temporary, and has a vague ending point. Loss of memory during this period is clearly anterograde rather than retrograde, since the ability to form long-term memory is completely blocked.65 It has been stated that “[an alcoholic blackout] is not forgetting, rather it is not remembering,” implying that, at a high BAC, new memories cannot be formed.66 The individual may or may not appear intoxicated, but will still be able to maintain a coherent and interactive conversation (short-term memory), recall past events (recall from long-term memory), and perform normal activities (procedural memory). This is a critically important problem from a legal standpoint, because, during a blackout, individuals with intact immediate and short-term memory have the ability to form the specific intent needed to commit crimes that require this ability, despite their inability to retain their involvement in the crime in their long-term memory. The occurrence of an alcoholic blackout is most often recognized only in hindsight as a complete absence of memory during a specific period. Memory loss as a result of an alcoholic blackout should be differentiated from simply becoming unconscious or “passing out.” In addition, many individuals experience partial memory losses or “grayouts” during alcohol consumption. The possibility of alcohol-induced blackouts in individuals testifying at trial becomes a contentious point for juries to consider in assessing the credibility of witnesses who were under the influence at the time of the crime.
Relationship to BAC
It is generally accepted that a high level of blood alcohol is necessary, but not sufficient, to produce an alcoholic blackout. One small study found a mean BAC of 0.279 percent during blackouts; therefore, a value of 0.25 percent was suggested as a reasonable estimate of a threshold BAC for producing an alcoholic blackout.65 Perry et al.67 found a strong linear relationship between BAC and the predicted probability of a blackout as a function of BAC, described by Equation 6:
 Their finding clinically concluded that subjects with a BAC of 0.308 g/dL or greater have a 0.50 or greater probability of having experienced an alcoholic blackout.
Their finding clinically concluded that subjects with a BAC of 0.308 g/dL or greater have a 0.50 or greater probability of having experienced an alcoholic blackout.
Legal Implications
A person's criminal liability for actions taking place after alcohol intoxication depends on whether the intoxication was involuntary or voluntary. Involuntary intoxication implies that the defendant either did not know that the substance was intoxicating or was forced to ingest it. As such, involuntary intoxication may be a complete defense. However, voluntary intoxication is never a defense. A sober individual is free to choose whether to drink, and the person knows beforehand the potential adverse consequences of excessive drinking. If one voluntarily chooses to become intoxicated, one willfully increases the risk of harm to others by reducing one's mental capacity for evaluating danger and controlling one's actions.
Voluntary intoxication may be used sometimes to prove lack of mens rea, the mental state a person must possess while taking part in a crime. Under some jurisdictions, voluntary intoxication can negate some culpable mental states, such as specific intent. An example of a situation in which specific intent is a requirement is burglary, defined as the illegal breaking and entering of a dwelling with the intent to commit a further felony. To prove a charge of burglary, the prosecution must show that the defendant intended to commit a felony subsequent to breaking and entering. However, voluntary intoxication may not be used effectively as a defense to crimes of general intent (e.g., assault, battery, or rape).
The following example from Watterson68 provides an excellent description of how people experiencing an alcoholic blackout can act and illustrates the legal implications: A defendant was charged with stealing a car. A charge of auto theft requires that the defendant intended to deprive the owner of the car permanently. A defendant who does not have this intent cannot be convicted of theft. The defendant contended that he had a blackout from drinking and did not have the specific intent required for the crime. The court however concluded that the alleged blackout did not prevent the defendant from starting the car by substituting a beer can opener for an ignition key, nor from driving the automobile in city traffic with normal ability, nor from fabricating a story in an attempt to protect himself from questioning by a police officer.
Conclusion
Alcohol intoxication can lead to a range of clinical manifestations and dangerous, unlawful activity that result in injury or death. In forensic investigations involving DUI cases and alcohol-related traffic deaths, extrapolation and interpretation of blood alcohol levels is important in determining criminal liability. Knowledge of basic pharmacological properties of alcohol and the inter- and intra-individual variations in alcohol absorption and elimination is essential for determining the role alcohol plays in modifying behavior and contributing to criminal behavior.
Acknowledgment
The authors thank Keith Yoshizuka, PharmD, MBA, JD (Assistant Dean for Administration and Chair, Social Behavioral and Administrative Sciences, Touro University California College of Pharmacy), for consultation and advice on law and liability in the development of this manuscript.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2017 American Academy of Psychiatry and the Law





{kind=link}