


Abstract
Correctional systems, already struggling to meet the basic and functional requirements of older prisoners, will be further challenged by the increasing medical and psychiatric needs of this population. Mental health and general medical care for older adults requires specific on-site or consultation expertise in geriatric medicine and psychiatry, as well as potential changes in infrastructure, both of which may be prohibitively expensive. However, compassionate and effective treatment of older prisoners requires that prison and legal systems facilitate this expert care. To address this situation, strategic revisions of the criminal justice system are needed to alleviate prison overcrowding and consequent inadequate medical care for inmates, especially the elder ones. The unique, age-related demands of this older population predict an increased need for forensic psychiatrists with a thorough knowledge and expertise in geriatrics, as more forensic psychiatric evaluations will be needed before trial in both civil and criminal cases, during incarceration, and at the time of parole. In this article, we review the current state of elder inmates in correctional institutions and advocate for increased geriatric training for forensic psychiatrists in anticipation of this growing need.
By 2029, the “baby boomers” and post baby-boom generations will all be of advanced age (55 or older).1,–,3 A report published by the Institutes of Medicine (IOM) in 2012 asserted that, by 2030, the population of adults over the age of 65 will reach 72.1 million, far surpassing the 42.3 million in 2010. Of particular concern, the report also estimated that 14 to 20 percent of the elder population, or approximately one in five older adults, has a mental health or substance abuse disorder, such as depression, dementia, or related psychiatric and behavioral symptoms.4
In the community, age 50 or 55 would not be considered advanced age, but incarcerated men and women typically have physiological and mental health conditions that are associated with people at least a decade older. Thus, the health of a 50-year-old prisoner is more akin to that of a 65-year-old living in the community. This process, known as accelerated aging,5,–,7 is caused by inadequate access to medical care before incarceration,8 substance abuse,8 the stress of incarceration,5,8,9 and a lack of appropriate health care during incarceration.9 These factors contribute to the discrepancy in the prison population between chronologic and physiologic age.10,11 As a result, the National Institute of Corrections classifies prisoners over the age of 50 as “aging,”9,12 with previous work by the Bureau of Justice Statistics using 55 years as their definition of “old age.”13,14 Thus, there is no clear consensus on the definition of “older” in the prisoner population.10 However, given that the trend in the literature is also to define old age in the prison population as beginning at age 55,13,14 advanced age will be defined in this article as 55 and older.
Older aged inmates are the fastest growing group of prisoners in the United States and Canada, with the growth rates projected to rise.11 Between 1995 and 2010, the number of prisoners in the United States grew by 42 percent, while the U.S. prison population aged 55 and older grew at 282 percent, six times the overall rate.6,15,16 Similarly, from 2000 through 2009, the overall prison population increased by 16.3 percent, but the number of older prisoners increased by 79 percent.17,18 Even more striking is the number of persons aged 65 and older who received prison sentences, which increased by 63 percent; in contrast, the general population sentenced to prison increased by only 0.7 percent during the same period (2007–2010). The rate of incarceration of elder persons exceeds the incarceration rate of all persons in most countries.15 Moreover, this crisis is not limited to a handful of states with so-called “poor sentencing policies” (Ref. 17, p 2). In 2009, it was determined that more than 28 states had greater than 1,000 older prisoners, compared with 2 states in 1990.19 By 2014, both the Pew Research Center and the American Civil Liberties Union found that older inmates accounted for more than 16 percent of the prison population, an estimated 246,600 prisoners nationwide.16 At this rate, it is projected that by 2030, older prisoners will account for one-third of all incarcerated persons in the United States, with upward of 400,000 older prisoners, a 4,400 percent increase in 50 years.6,16 This sustained mass incarceration of older individuals has major economic, social, ethics-related, and health implications.16
Methods
Potential studies for inclusion were identified by querying Pubmed, PsychInfo, Ovid, Medline, and Westlaw Database up to June 2015, for various combinations of these terms: “geriatric,” “older,” “elderly,” “arrest,” “incarceration,” “prisoner,” “inmate,” “forensic,” “psychiatry,” “forensic psychiatry,” “geriatric psychiatry,” and “trial.” Duplicate studies and legal reports were not included. Articles reporting descriptive, observational, analytical, and experimental studies were considered for establishing current conditions and the number of individuals over the age of 55 within the criminal justice system, particularly within the U. S. Department of Corrections. Analysis revealed that most of the studies were projective in nature, reflecting the general lack of data and research in the field. The search yielded 107 publications that fulfilled our requirements. Categories and the number of articles found included: medical articles, 43 (40%), legal cases/articles, 22 (21%), new articles, 20 (19%), government papers, 10 (9%), and other types of literature, including publications by interest groups and books, 12 (11%). Given the lack of research in this field, international journals were included. Notable sources included Department of Justice publications; the journals Medicine, Science and the Law; Elder Law Journal; Journal of Aging and Social Policy; and International Journal of Geriatric Psychiatry; forensic science and psychology journals; and the interest groups Agency on Aging and American Civil Liberties Union. Given the limited number of both scientific and legal cases directly speaking about older inmates, all studies were considered for inclusion. Articles were excluded if they did not directly address the main subject or causality, were about the wrong setting or age group, measured outcomes that were not relevant to the study question, or lacked outcome data or adequate analyses. Most of the medical articles addressed age-related diseases (e.g., dementia) or substance abuse in the geriatric population interacting with the legal system. The Sourcebook of Criminal Justice Statistics, a free online report of nationwide arrests by category of crime and age by decade, was the best definitive source for establishing trends between older individuals and increased interaction with the legal system. The data were consistent with those reported in the queried studies.
Results
Causes of Incarceration
The reasons for the increase in the older prison population are multifactorial. Stringent mandatory sentences, three-strike laws, and the so-called war on drugs have resulted in longer sentences.11,16 The combination of limited parole opportunities, underuse of compassionate early release, and truth-in-sentencing laws has caused a bottleneck effect, wherein a greater number of individuals are serving longer, inflexible prison sentences.11,16 Indeed, the majority, up to 65 percent, of older inmates are serving time for nonviolent offenses (e.g., fraud, larceny, burglary, breaking and entering, and traffic and public order violations) and drug charges, many of which were committed much earlier in their lives.6,20 It is unclear how recent changes in laws and attitudes toward marijuana may affect these rates in the future.
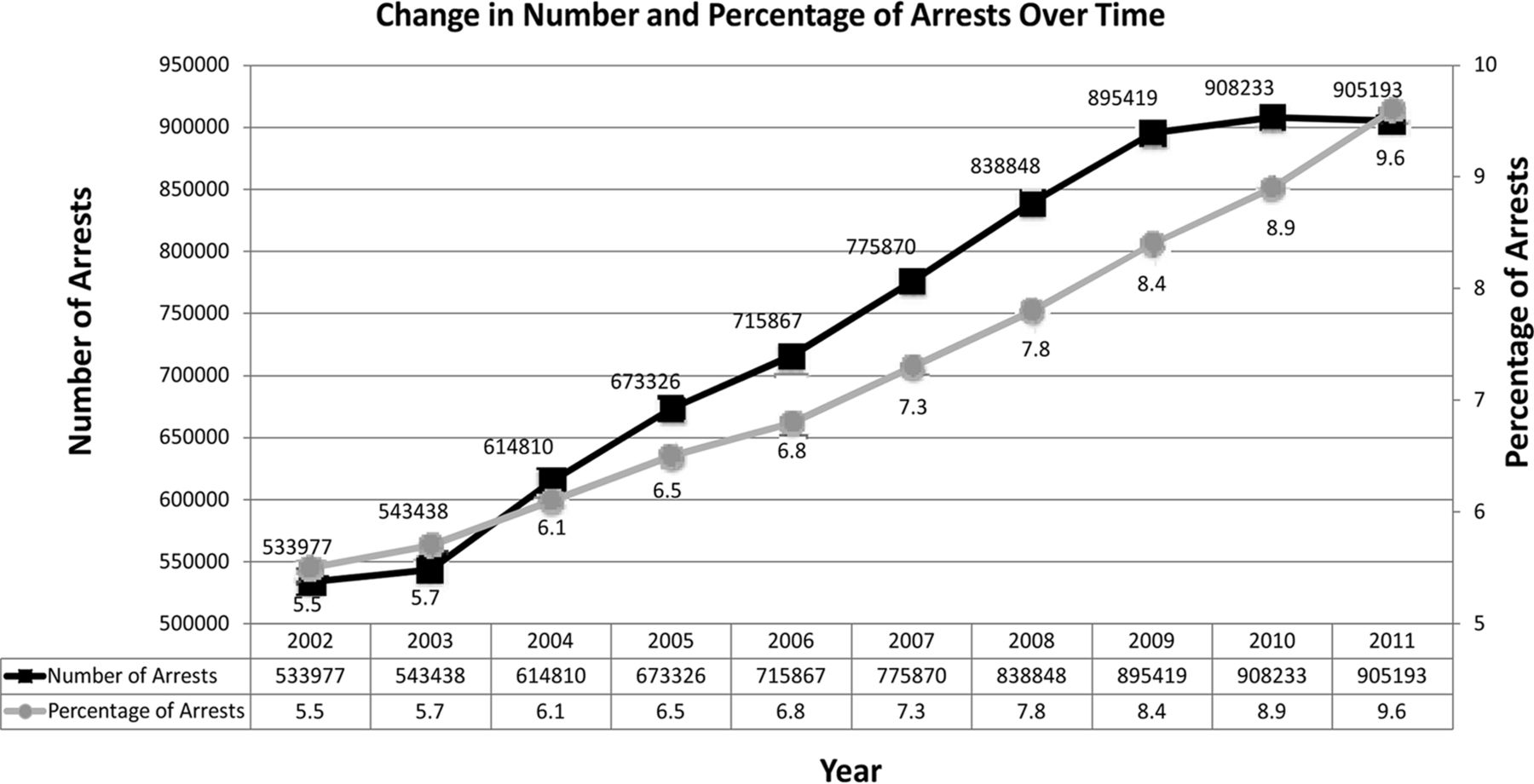
In parallel, older individuals are also committing more crimes21 and are being arrested with increased frequency.22 In 2002, older persons accounted for 533,977 arrests, representing 5.5 percent of the total.23 By 2010, this number had risen to 908,233, comprising 8.9 percent of all arrests,24 and had increased again to 9.6 percent in 201125 (Fig. 1). Some have suggested that the increasing number of arrests is a natural result of the aging demographics of the U.S. population.15 However, the statistics do not support this hypothesis: in 2000, 27.9 percent of the U.S. population was over age 50, but accounted for only 5 percent of arrests; by 2011, 32.7 percent of the U.S. population was over age 50, and accounted for 9.6 percent of all arrests.25 Concomitant population-wide changes in factors such as race, gender, and immigration status over time have not been fully explored, and a breakdown of these factors in arrested individuals is not currently available. Thus, it is possible that these factors may help explain, at least in part, the trends in arrest patterns. Alternatively, novel traits of the baby-boomer cohort could account for the increase in arrests. The baby boomers led the social upheavals of the 1960s and 1970s (e.g., the civil rights, gay rights, and feminist movements; the Vietnam protests; and the sexual revolution), and pioneered changing attitudes about, and rates of, substance use, with dramatic increases in the use of illicit drugs.2,26,27 Some baby boomers also have tended to maintain these habits and histories of drug use in later life, often continuing to engage in drug misuse or abuse.28,–,31 With the changes in attitudes, socially acceptable behavior, and at times, habits (such as illegal drug use) of the baby-boomer generation, came increased risk of interaction with the legal system, compared with that of older cohorts.32,–,35 Today, older men and women in increasing numbers are entering prison for the first time in their later years. Between 1995 and 2009, the number of new commitments in persons 55 and older grew by 109 percent, whereas the overall rate (inclusive of all ages) increased by only 9.7 percent.15
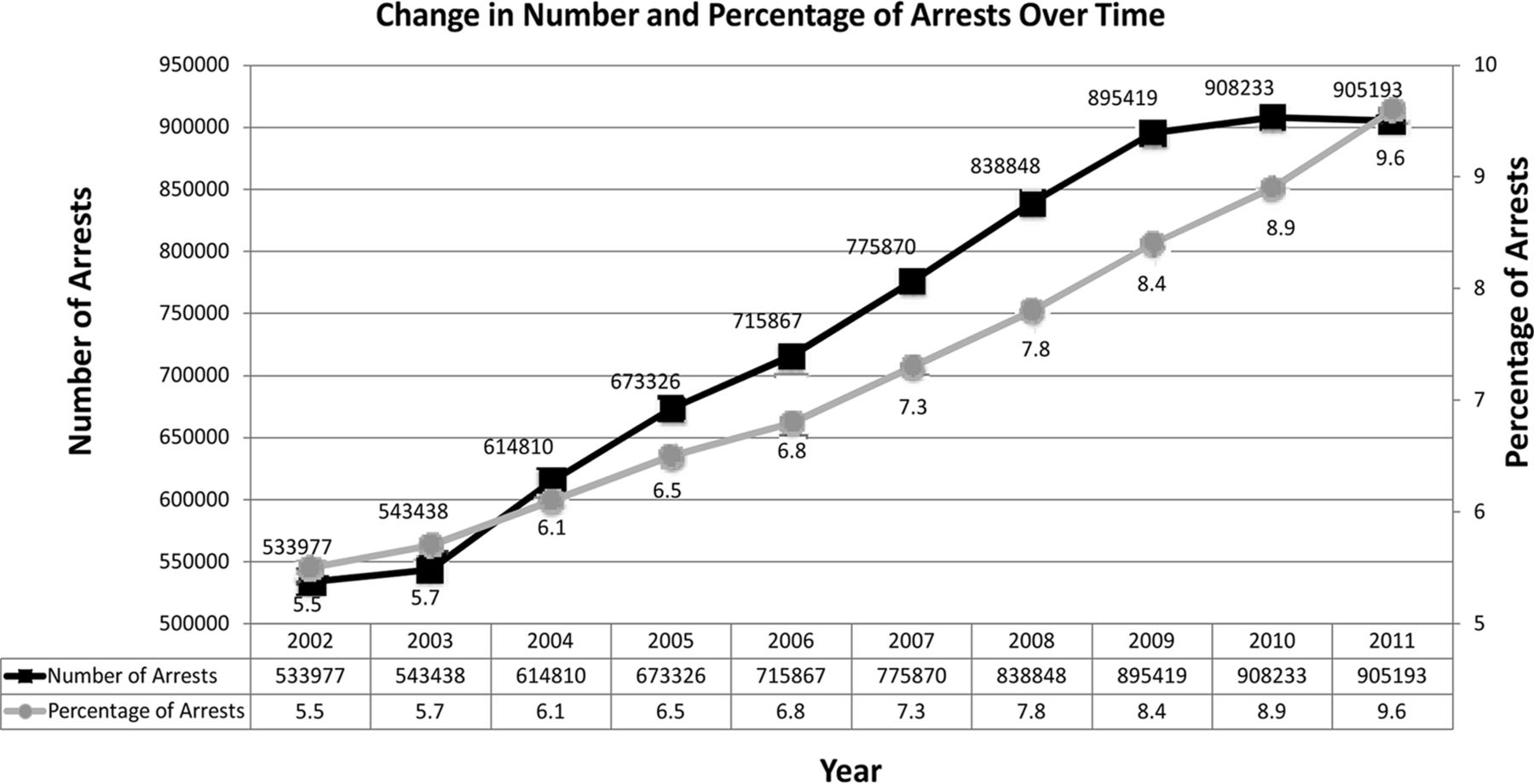
Change in number of arrests and percentage of arrests for persons aged 55 and over from 2002 through 2011. Graphical representation of numbers of arrests of older individuals and the overall percentage of arrests that this number represents compared with all age classes over time. An increasing trend in both number and percentage of arrests is demonstrated.23,–,25
Violent Crimes Perpetrated by the Elderly
The number of violent crimes committed by older persons is increasing. Charges for violent offenses (such as murder, aggravated assault, and sex crimes) accounted for approximately 15 percent of arrests of older individuals in 2002 but rose to greater than 25 percent by 2011.23,25 In 2009, 25.8 percent of persons over 55 entering prison had been convicted of violent crimes.15 A significant number of these late-life offenders are now serving life sentences handed down because of the violent nature of their offenses.23,–,25
More older persons with violent tendencies are accumulating within the prison system. Studies have shown that older offenders are often treated more leniently (e.g., community rehabilitation over prison), especially if their health is failing.36,–,38 However, this leniency has not extended to those who have committed violent crimes.36 As a result, older individuals who ultimately enter prison later in their life are more likely to have been responsible for violent offenses.11 In addition, persons convicted of violent crimes when they were younger were more likely to receive long or life sentences, often without parole, such that they remain in the system, whereas those convicted of less violent offenses are often paroled.15 These factors contribute to a stacking effect, wherein a disproportionate number of older individuals are convicted of violent crimes compared with younger ones,15 resulting in a situation in which older individuals are less likely to be paroled or released and are among the most expensive for whom to provide care.16
Discussion
Economics of Incarceration of Older Persons
Older prisoners are the most expensive inmates to care for, costing two to five times more (a mean of $68,270 per individual) than younger inmates (a mean of $34,135 per individual).6 The United States spends more than $16 billion annually on the incarceration of older persons,6 which may be an important reason that state corrections budgets have increased 674 percent in the past 25 years.6 It may also explain why incarceration has become a potent political debate for state legislatures who fear that incarceration of older individuals will prove unsustainable if meaningful action is not taken.16
Health Effects of Aging in Prison
Prison often leads to a rapid decline in an older person's health. Before entering prison, many individuals have declining health that is the result of lifestyle and substance abuse.16,39 Accelerated aging in prison exposes and exacerbates these underlying medical and psychiatric conditions.5,7,12 The stressful conditions of prison confinement, such as prolonged exposure to overcrowding, social deprivation, and violence,40,–,42 further increase the risk of early onset of serious physical and mental illness, including dementia.43 There is also a higher prevalence of communicable and chronic diseases in older inmates, compared with both the general population and overall prison population; these include hepatitis, HIV, tuberculosis, arthritis, hypertension, gastric ulcer, prostate disease, pulmonary disease, cardiovascular disease, cerebrovascular accidents, Alzheimer's dementia, chronic pain, and cancer.11,44,45 Indeed, central nervous system disorders are among the most common in older incarcerated individuals,46 with high rates of depression, anxiety, trauma history, stress, and cognitive impairment.47,48 There is some degree of cognitive impairment in 40 to 60 percent of older prisoners, a rate that far exceeds that of the general population.49,50 Elderly sex offenders, in particular, have higher rates of dementia,51,–,53 but cognitive impairment as a whole, as in the general population, is very likely underreported and, as a result, undertreated.10,54 Despite these numbers, many do not have access to treatment,50 and overcrowding and underfunding contribute to inadequate treatment of incarcerated individuals.55,56 Given the prevalence of neuropsychiatric conditions, forensic psychiatrists should be aware of these trends and make a point of screening older incarcerated individuals for these conditions, as recognition can lead to less morbidity and cost through earlier treatment.57,58 Thus, forensic psychiatrists should be adept at recognizing and treating the somatic and cognitive presentations of these age-related disease processes.
Specialized Geriatric Treatment
Older prisoners benefit from specialized facilities. Prisons were not designed to be long-term care facilities, and the infrastructure of prisons can be problematic for older inmates (stairs, lack of wheelchair access, lack of hand rails, narrow doorways, long halls, for example). The Americans with Disabilities Act requires that newer prison facilities be handicap accessible, but there is no mandate that older facilities be retrofitted architecturally to accommodate the needs of older persons.59 Moreover, there is a general lack of geriatric specific programming within prisons with only 4% of correctional facilities providing this specialized level of care.60 Geriatric-specific prison programs have been implemented in correctional systems in a few states such as: New York, Ohio, Nevada, Louisiana, and California.61,–,63 These programs typically focus on inmate peer support, advocacy for prison and community reintegration, and incorporating interdisciplinary collaboration among social workers, doctors, nurses, law enforcement, and lawyers.43 In these paradigms, older patients are provided with age- and ability-appropriate activities and training that may ultimately help inmates learn the skills needed for navigating old age. One current limitation to expanding such programs is lack of specialists trained in geriatric conditions, including forensic psychiatrists.
Practical Solutions
A multifactorial approach to addressing the various needs of the incarcerated elderly is needed and should be established. Rethinking the healthcare needs of older prisoners requires acknowledgment of the problems that they face and a creative vision to provide solutions for the overcrowding and fiscal crises in prison systems nationwide. Suggested reforms include early release programs, medical parole, and compassionate release; creation of specialized housing units; and modification or repeal of the current sentencing laws.64 Further, clinicians and providers must be better trained to manage the growing number of geriatric inmates. Each of these approaches introduces positive and negative aspects that warrant further discussion.
Early-Release Programs
Many states have early-release programs, but they are largely underused because of overly restrictive qualifications. Inmates of advanced age, whether convicted in younger years or in later life, have recidivism rates close to zero.65 Given the low risk of recidivism and high cost of incarceration for older inmates, many have called for increased usage of these programs. Studies have indicated that states could save $66,294 annually per older inmate released,6 and the parole of older inmates would cost states significantly less than incarceration, inclusive of social services used.6,66 However, although this strategy may remove the financial burden from the state correctional budget,6,67,68 it does not necessarily decrease the overall cost to taxpayers. Upon release, most older individuals will need multiple federal programs, including Medicare, social security, subsidized housing, and food stamps.6,15,64 Thus, despite saving money overall (primarily from the state's budget), the financial burden would be transferred from state to federal budgets, in turn placing additional strain on existing federal systems, many of which are projected to be bankrupt by 2026.69,70 The potential influx of released older prisoners with complex and expensive health needs, worse overall health, more meager financial resources, and fewer options for employment could be terminal for government-run health programs, such as Medicare and Medicaid.70,71
To balance the financial need to release inmates with society's concern for safety, some have suggested the implementation of a review of all inmates starting at age 50.57,58 These reviews, envisioned as similar to board of parole hearings, would examine a set of identifiable markers, such as rehabilitation efforts, prior disciplinary actions, and history of substance abuse to determine an inmate's status.58 A classification system (low, medium, and high risk) would be developed to determine an inmate's likelihood of release,57,58 with estimations suggesting that release of as few as 500 low- to moderate-risk inmates could save states $15 to 20 million every year.57 If the appeals were modeled after petitions for writ of habeas corpus, the courts could adjudicate them on a case-by-case basis.58 Appeals of this nature would require a full assessment of a prisoner's current degree of functioning. Given that age is inherent in this paradigm, a forensic psychiatrist trained to identify and treat the neurocognitive disorders associated with aging would be best suited to such evaluations. Moreover, enacting such hearings and appeals would further increase the need for geriatrically trained forensic psychiatrists.
Compassionate Release
Some have suggested earlier release of individuals with severe medical conditions. Release would occur regardless of the length of the sentence served or the age of the inmate, as health-compromised individuals are the most expensive cohort because of exorbitant medical costs.72 Medical parole or compassionate release, as it is typically called, is designed for an inmate who is physically incapacitated, terminally ill, or actively dying.11 Texas has the most aggressive definition, including anyone who is elderly, is physically disabled, has mental or terminal illness or developmental delay, or has a condition requiring long-term care.64 Despite this broad definition, less than 10 percent of applicants have been approved for the program.73 The difficulty comes in the overly restrictive practice11 parole boards use in defining those who are sick enough to be considered.74 Parole boards, notoriously overworked and under-resourced, are ill-prepared, financially or logistically, to monitor these early-release cases.75,76 As an example, while recidivism rates are generally low within this population, certain crimes, such as sexual offenses, have higher rates and require a higher level of monitoring53; thus, this option may not be ideal for those incarcerated for these sorts of crimes.53
The decision for compassionate release relies on recognition of qualifying conditions, many of which are more common in advanced age and can be facilitated by advocacy for the inmate. Forensically trained psychiatrists are best suited for these tasks. However, to do so optimally requires a solid knowledge base in age-related and terminal conditions, suggesting again that geriatric training would be helpful. Further, geriatrically trained forensic psychiatrists, as medical doctors, would also be helpful in advocating for and advising on placement options, given that ex-felon status and inherent severity of medical conditions can make placement and housing of these individuals particularly difficult.11,15
Need for Age-Specific Rehabilitation Training
Released inmates need transferable skills and financial options consistent with their stage of life if early or compassionate release programs are to succeed. Traditional rehabilitation and skills-training programs may not provide the necessary skills for older individuals.58 Despite overall low recidivism of older inmates, it was found in California that failure to provide skills essential for them to transition from prison to outside life resulted in recidivism rates as high as 45 percent in individuals aged 60 and above.57 As a result, some have suggested focusing educational programming for older individuals toward comprehensive transitional skills: help with obtaining food, housing, and employment to underpin a basic routine for daily life.57 Such specialized programs require that persons involved be knowledgeable in age-related challenges and call for further geriatric training of medical and support staff alike, including forensic psychiatrists.
Establishment of residential re-entry centers (analogous to half-way houses) could assist older inmates with the transition and help them acquire jobs, social contacts, and the federal resources necessary for subsistence in the outside community.58 Without such resources, it is projected that upward of two-thirds of all released individuals could be re-arrested and ultimately returned to jail within three years.66 Again, given the age-related nature of these centers and the commonality of neurocognitive conditions in this population, training in age-related conditions and interventions for both staff and treating psychiatrists would be essential.
Specialized Inmate Housing
High-risk elderly inmates or those unable to be released for other reasons may require the development of specialized housing units within the prison. Such specialized housing units could focus on the particular medical and neuropsychiatric needs of elderly and infirm inmates.15,58 Early recognition and treatment of medical and psychiatric conditions (preventive medicine) would be likely to result in healthier prison populations, better control of chronic disease, and a decrease in the costs of transferring inmates to external hospitals for specialized care.57,58 These prison units would address functional and medico-psychiatric needs linked to aging, including specialized diets, wheelchair access, handrails, fewer or no stairs, decreased distances for walking, and safety showers, among other needs,58,64 as well as assuring that all constitutional rights are met as set out by the Americans with Disabilities Act.64,77,78 Such facilities require the presence of medical and support staff trained in both legal and age-related disease processes, arguing again for more geriatric training of forensic psychiatrists and medical staff.
Inmates may benefit socially from age-stratified housing. Studies have suggested that elderly male inmates prefer such specialized housing units because they feel less hasseled and victimized, and benefit from the quieter environment.78,–,80 Grouping older inmates in this manner would allow activity planning, educational programming, and social skills training targeted to the needs of this population.58,78 As discussed earlier, such training paradigms benefit from staff knowledge of neurocognitive and medical processes of aging inclusive of geriatrically trained forensic psychiatrists.
Sentencing Reform
Legal reform is necessary to fully address this crisis. Decreasing the length of prison terms and substituting other rehabilitation programs for elderly offenders would significantly reduce the number of elderly individuals entering prison.71 The use of specialty courts could reduce the number of incarcerated older individuals81 and increase the use of home detention and community-based programs.70,82,83 In addition, reforming sentencing guidelines would afford judges greater discretion in determining sentences and allow for alternatives, such as drug and alcohol rehabilitation programs.84 Community-based solutions are more cost effective and lead to lower recidivism rates, as resources can be used to help individuals find jobs and integrate into the community rather than face an expensive perpetual incarceration.84 Re-examination and reform of the legislation and policies that resulted in the mass incarceration of older persons is also warranted.85 The type of change needed would take time to work through the system, but would ultimately reduce the overall prison population, including older inmates, thereby decreasing medical and assistive costs.64 Such reform would also allow inmates previously sentenced under excessive sentencing laws to apply for resentencing, which could be reviewed on a case-by-case basis to determine whether more time is needed.86 Taken together, these three steps could result in significant reduction in the rates of incarceration of the elderly in tandem with a significant reduction in costs;86 all three also produce a need for forensic evaluations, best performed by forensic psychiatrists with expertise in geriatric conditions.
Need for Geriatrically Minded Forensic Psychiatrists
Older individuals who become entangled with the legal system may need a competency or capacity evaluation before even appearing in court.21,87,88 The prevalence of psychiatric disorders among first-time offenders aged 60 or more referred for forensic psychiatry evaluation ranged between 50 and 97 percent, with the most common diagnoses (in descending order of frequency) being dementia, psychosis, personality disorders, alcohol use disorder, organic lesions/postcerebrovascular injury, and mild learning disability.89,–,91 Given the replicable, high rates of dementia found in older first-time offenders interacting with the legal system, some have suggested that a thorough cognitive evaluation of any older adult presenting to the legal system may be warranted.8
Geriatrically informed forensic psychiatrists also have a role after sentencing. Studies have shown that some inmates with advanced dementia are unable to recall their crimes or even to understand that they were incarcerated. Although reminded of their crimes before a parole hearing, they may not remember their offenses and therefore are incapable of showing remorse. Thus, the possibility of parole is significantly limited,92,93 and the fairness of a parole denial at such a hearing is questionable. In these situations, geriatrically informed treating or forensic psychiatrists, could review an individual's case to help determine appropriate outcome and placement. These providers could also help ensure that appropriate medical and behavioral techniques are used in the treatment of these inmates.
The need for geriatrically trained forensic psychiatrists will only grow in the future. The aging prison population mirrors the general population while the American Psychiatric Association predicts that the ratio of geriatric psychiatrists will fall from 1 for 23,000 to 1 for 27,000 individuals 65 and older by 2030.94 Moreover, the projected increase in the number of older individuals interacting with the legal system and the under-recognition and undertreatment of psychiatric morbidities in this group suggests a need for age-sensitive service advancements and warrants whole-scale revisions in the provision of medical care and facility restructuring in prisons to care for older inmates.89 However, the complex neuropsychiatric and forensic needs of older, mentally impaired individuals falls into the domains of both geriatric and forensic psychiatry, introducing the possibility that neither service can manage these individuals in isolation.38,95,96 Compassionate care of aging prisoners requires the expertise of both disciplines, and collaboration between both subspecialties is essential. With this in mind, some have suggested a need for the establishment of specialist tertiary forensic (with the inclusion of geriatric) psychiatric services.38,96,97 Another possible solution involves embedding geriatric training modules into existing forensic psychiatry fellowship curricula and adding forensic training to geriatric psychiatry fellowships. Despite this, a group is likely to remain for whom specialized training beyond the basics will be necessary. Double board certification in both geriatric and forensic psychiatry would provide in-depth expertise in complex neuropsychiatric and forensic aspects of aging in inmates. Development and establishment of a formalized Geriatric Forensic Psychiatry Track, as has been established in Child and Adolescent Forensic Psychiatry,98 may also warrant consideration. Such a track could extend the current forensic training through the addition of specialized seminars addressing in more detail each of the sections described above (early release, compassionate release, and so forth), evaluation and treatment of neuropsychiatric conditions associated with aging, behavioral interventions for dementia, special needs of older sex offenders, community referrals and rehabilitation efforts for elderly inmates, and study of landmark forensic cases involving elderly individuals and the growing need for this specialized level of care in the civil courts.
Forensic psychiatric expertise is needed in noncriminal cases, as well. As the number of older individuals in our general population expands, questions of capacity to make major legal and personal decisions regarding the transfer of wealth and assets, or even questions of undue influence regarding changes or initiation of a will, are of utmost importance. Current conditions in the United States have fostered a situation in which there is an aging population with a disproportionate amount of wealth. Increased means combined with complex family dynamics created from higher divorce rates and remarriages, predict contestations of asset distribution, and challenges related to testamentary capacity and questions of undue influence can be expected with increasing frequency.99,–,101 Concomitant increases in recognition of psychiatric, neurologic, or medical disorders that affect cognition similarly create an apt environment for estate litigation.99,102 Given this, psychiatrists will be called on with increasing frequency to advise the courts regarding capacity to make or change a will, as well as susceptibility to undue influence.103 To best fulfill this role, forensic psychiatrists need knowledge regarding common neuropsychiatric conditions presenting in later life.
Conclusion
The aging inmate population is a major problem in social, economic, and medical terms. A combination of release programs, specialized housing, and sentencing reform is needed to address concerns about recidivism,15 public safety,16 finances, and questions of ethics.64 These efforts should be paired with improved training and education aimed at inmate re-entry into society, with a concentration on community resources and availability of federal benefits.11 Community and family70,72 resources, combined with federal benefits, will be necessary to provide compassionate care to the inmate while in prison and to provide parolees the resources they need to make a successful transition to life outside of prison. Current sentencing laws must be reformed to prevent further bottlenecks within the prison system.
While awaiting these measures, the medical and mental health community must prepare itself to manage this ever-increasing population. More forensic psychiatrists with additional expertise in geriatrics are needed to attend to older adults before trial, during incarceration, and at the time of parole. Evolving social dynamics and aging demographics of the general population increase the likelihood of testamentary and estate challenges and argue a clear need for forensic psychiatrists with knowledge and expertise in aging-associated problems, especially neurocognitive disorders. Given this need, it is time to implement increased training related to geriatric subjects within forensic psychiatry curricula, develop a reciprocal concentration within geriatric psychiatry, and possibly even create geriatric forensic tracks or pursue dual boarding in geriatric and forensic psychiatry.
Acknowledgments
The authors thank Brian Mac Grory, MD, Karsten Heil, MD, and Catherine Coughlin for assistance with the preparation of this manuscript.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2017 American Academy of Psychiatry and the Law
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵





{kind=link}