


Abstract
This study examined whether lawyers' attributions of responsibility for mental illnesses affect their decisions about involuntary treatment. A survey that was mailed in 2003 to Illinois lawyers involved in involuntary commitment elicited recommendations for involuntary treatment for characters presented in vignettes. The survey also sought respondents' attributions of personal responsibility for the onset and recurrence of mental illnesses. A total of 89 lawyers responded to the survey, a response rate of 48 percent. Decisions to hospitalize persons with mental illness involuntarily increased significantly with the level of risk of harm and were significantly related to attributions of responsibility for the recurrence of mental illness. Decisions to recommend involuntary medication were not related to attributions of responsibility.
In practice, lawyers as well as psychiatrists are influential in making decisions about the commitment of persons with mental illnesses. Although both groups of professionals participate in involuntary hospitalization processes, psychiatrists and lawyers may hold different views on the topic. For instance, in a previous study, 78 percent of psychiatrists surveyed viewed involuntary hospitalization as an indispensable treatment modality, while only 27 percent of attorneys who worked closely with clients in involuntary hospitalization cases held a similar opinion.1 The available data suggest that lawyers are reluctant to endorse involuntary hospitalization. In one study, attorneys who had participated in civil commitment proceedings tended to disagree that “a person has the best chance of recovery if s/he is hospitalized at the first sign of mental illness,” and agreed that “only as a last alternative should a person who needs help be sent to a mental hospital” (Ref. 2, p 325).
These studies, however, were conducted more than 20 years ago. Since that time, significant shifts in laws and attitudes have compelled us to revive research into attorneys' attitudes toward involuntary psychiatric treatment. In the present study, we sought lawyers' attitudes toward involuntary hospitalization and compared their views with those of psychiatrists (previously published3). We also explored lawyers' attitudes toward involuntary psychiatric medication administered in community settings, a legal and effective, if relatively underutilized, treatment option.4
The involuntary hospitalization of persons with mental illness is permitted when individuals are expected to inflict serious physical harm on themselves or others in the near future or are unable to provide for their basic physical needs. In studies of public attitudes, perceived dangerousness strongly predicted support for involuntary psychiatric treatment.5,6 Perceived dangerousness also determines psychiatrists' commitment decisions.3,7–9 In the present study, we looked at lawyers' perceptions of dangerousness in relation to their recommendation of involuntary hospitalization.
Further, among members of the general public, support for mandated treatment is related to viewing persons as responsible for their conditions.5,10 This finding has been explained in terms of attribution theory, a sociopsychological theory about the relationship between cognitive, affective, and behavioral responses to particular individuals or groups of people.4 Attribution theory predicts that if we view individuals with mental illness as not responsible for their illnesses, we will endorse sympathetic and helping gestures for these individuals. Conversely, the theory suggests that when people are viewed as responsible for the onset or recurrence of a mental illness, we may withhold help and/or endorse segregation and/or coercion of these individuals. Mental health researchers using attribution theory tend to interpret involuntary psychiatric treatment as a punitive gesture of segregation and coercion that the public justifies for persons it views as responsible for their own mental illnesses.10 From the perspective of the ethics of medical decision‐making, involuntary commitment would not be viewed as punitive, but as a necessary exercise of concern for the individual's well‐being, or beneficence.11,12
A survey of psychiatrists did not reveal any relationship between their attributions of personal responsibility and recommendations for involuntary hospitalization of survey characters presented in vignettes.3 In the present study, we replicated this survey with attorneys, to investigate whether the relationship between their attributions and involuntary treatment endorsements follows a pattern that more resembles that of the psychiatrists or that of the general public.
Methods
A structured survey was mailed to 191 lawyers in Illinois selected for their involvement in commitment (100 state's attorneys and 91 other publicly and privately funded lawyers involved in mental health law). The instrument was based on a survey created to assess psychiatrists' attitudes toward involuntary hospitalization.3 The first page described Illinois' legal requirements for psychiatric commitment (which includes a reasonable expectation of endangerment of self or others13). Informed consent was waived with approval from the University of Chicago's institutional review board.
The survey presented three vignettes about men with chronic mental illness. The first two concerned involuntary inpatient hospitalization. Of these two, one vignette character was increasingly unable to meet his basic needs, whereas the other was increasingly aggressive toward his mother. Respondents rated the appropriateness of committing each vignette character to inpatient hospitalization in four scenarios of escalating risk of harm: (1) not yet begun to deteriorate; (2) showing deficits but no damage; (3) in danger, but not at imminent risk; and (4) at imminent risk of harm.
The survey also elicited respondents' recommendation to initiate an involuntary outpatient psychotropic medication hearing for a third vignette character who demonstrated aggressive behavior toward his mother when not taking medication. For all three vignettes, at each stage at which respondents judged the appropriateness of involuntary treatment, they were also asked whether the likelihood that a mental health professional or a judge would support the involuntary treatment of the vignette character as depicted affected their judgments (see Appendix for vignettes).
Attributions of personal responsibility for the onset and recurrence of mental illness were assessed. Respondents were asked: “Overall, on the basis of your experience working with mentally ill clients, what percent of people with serious and persistent mental illness can be seen as being responsible for the onset (or recurrence) of the illness?”
The survey also presented concerns regarding involuntary hospitalization, such as, “Psychiatrists cannot predict the future so it is important to wait for actual harm before considering involuntary hospitalization.” Respondents indicated to what extent such concerns played a role in their judgments about hospitalization in the vignettes (1, played no role in my judgment, to 7, played significant role in my judgment). The survey also elicited the respondents' level of agreement with ideas about beneficence and autonomy, such as “lawyers have an obligation to encourage clients to get treatment ” and “lawyers should respect clients' expressed interests” even if the lawyer thinks the client may be “harmful to the client or others.” Demographic and professional practice information was also collected.
Inpatient commitment recommendations by type of threat of harm (harm to self or to others) were collapsed at each level of harm. The sum of these variables formed an aggregate score for recommending inpatient hospitalization, which served as the dependent variable in the bivariate analyses of demographics, attributions of responsibility, and views toward providing care. Multivariate analyses were used to examine differences in recommendations to hospitalize across levels of risk of harm.
Results
There were 89 respondents, a response rate of 48 percent. Most were men (60 percent, n = 51), with a mean age of 49 (SD = 11) years. Nearly 50 percent of respondents were state's attorneys (n = 42), nearly 30 percent were publicly funded lawyers (n = 24), and about 20 percent were attorneys in private practice (n = 19). One‐fourth of all respondents identified themselves as “regularly involved in commitment” (n = 22). Over the past five years, 15 percent of respondents had been involved in more than 40 commitment cases per year (n = 13), whereas 70 percent had been involved in fewer than 2 such cases per year (n = 62).
Involuntary Hospitalization Vignettes
In the vignettes, recommendations for involuntary inpatient hospitalization became stronger as the level of risk of harm increased (Fig. 1). At the lowest level of risk of harm, when individuals had not yet begun to deteriorate, respondents judged involuntary hospitalization to be inappropriate (mean score = 1.5, SD = 1). At the highest level of risk of harm, when individuals were at imminent risk of harm to themselves or others, respondents judged involuntary hospitalization to be close to “absolutely essential” (mean score = 5.7, SD = 1.4).
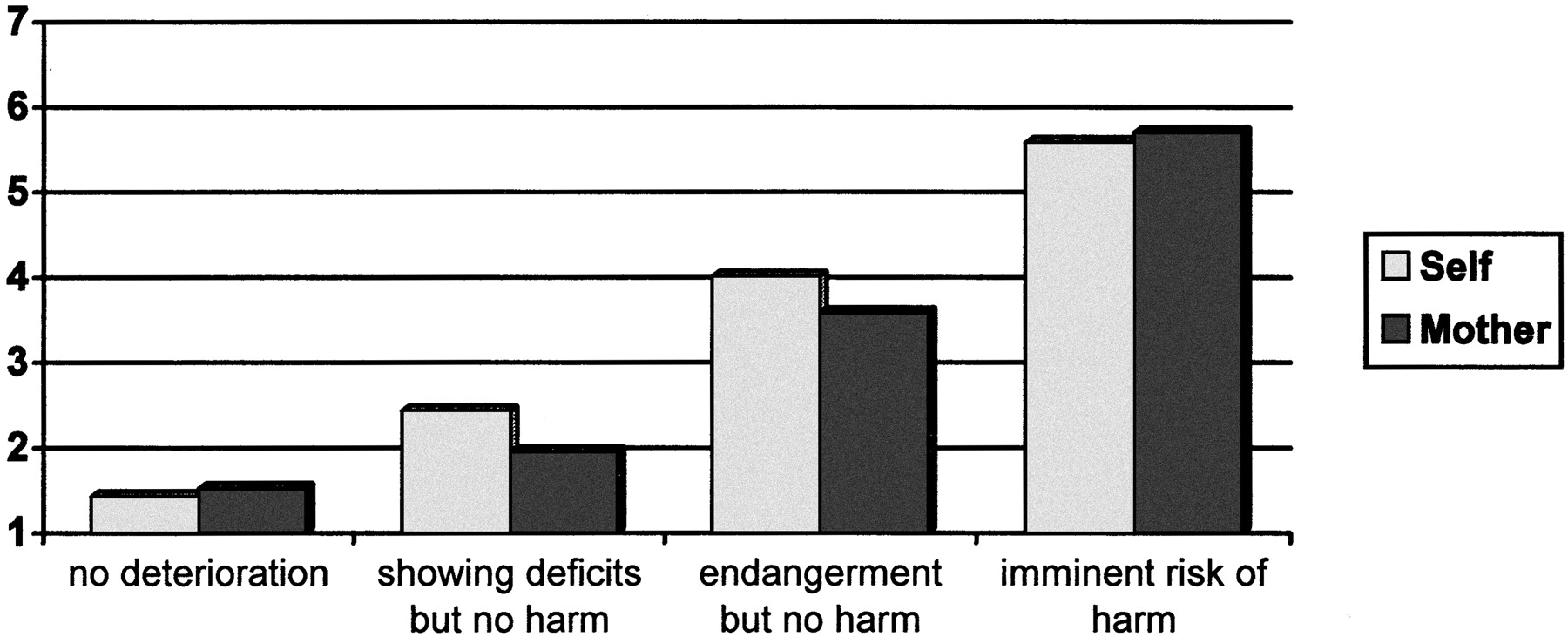
Vignette recommendations for involuntary hospitalization (N = 84). Scale on the y‐axis: involuntary hospitalization: 1, not at all appropriate, to 7, absolutely essential.
Recommendations for involuntary hospitalization for the self‐harm and harm‐to‐mother vignettes were not significantly different at any level of risk of harm. Therefore, response data from the two scenarios were collapsed for all subsequent analyses. There were, however, significant differences between commitment recommendations at different levels of risk of harm (p < .001; Table 1).
Recommendations for Involuntary Hospitalization in Scenerios Depicting Escalating Risk of Harm to Self or Others*
When asked whether a mental health professional's or a judge's likelihood of supporting involuntary hospitalization played a role in decisions about vignette characters, responses all fell below the midpoint of a scale in which 1 represented no role and 7 a significant role. Thus, respondents' vignette decisions were not strongly motivated by considerations about what mental health professionals or judges would do in response to the same scenarios.
In terms of attributions of personal responsibility, respondents considered 15 percent of all people with mental illness responsible for the onset of illness and 31 percent responsible for its recurrence (Table 2). Twice as many people were viewed as personally responsible for the recurrence of mental illness as for onset (paired means t test = −4.91, df = 62, p < .001). On average, respondents attributed responsibility for the recurrence of illness to less than one third of all persons with mental illness.
Persons Responsible for Onset and Recurrences of Mental Illness
We also investigated respondents' concerns about involuntary hospitalization. The respondents said that such concerns played a role in their vignette commitment decisions, but not a strong role (estimated by mean scores near the midpoint of a scale in which 1 signified no role and 7 a significant role). For example, the mean response for “involuntary hospitalization will interfere with the therapeutic process” was 2.7 (SD = 1.9), and for “involuntary hospitalization will deter people from seeking treatment,” 2.8 (SD = 2).
We asked respondents whether they agreed or disagreed with statements that supported beneficence toward the patient or respect for the patient's autonomy. More than 70 percent of respondents agreed that lawyers have an obligation to encourage clients to get treatment (71.9%, n = 64) and to act in the best interest of their clients (73%, n = 65). Less than half of the lawyers surveyed, however, agreed that lawyers should respect the client's preferences even if those preferences may be harmful to self or others (46.1%, n = 41).
Vignette commitment recommendations were related to attributions of responsibility for the onset and recurrence of mental illness (Pearson's r = 0.31, p < .05; r = 0.41, p < .01 for onset and recurrence attributions, respectively). The more respondents viewed persons as responsible for their mental illnesses, the more they endorsed involuntary hospitalization for the vignette characters.
Professional practice orientation was related to both hospital recommendations and attributions about mental illness. Respondents who identified themselves as state's attorneys endorsed involuntary hospitalization more strongly than did respondents who identified themselves as publicly funded lawyers at all four vignette levels of harm (see Table 1; repeated‐measures ANOVA, F = 8.96, df = 2, 78, p < .001, Tukey's honest significant difference [HSD] p < .001). In addition, state's attorneys opined that a greater percentage of those with mental illness were personally responsible for the recurrence of their mental illnesses than did publicly and privately funded lawyers (Table 2; one‐way ANOVA, F = 3.2, df = 2, 62, p < .05).
In these types of studies, often respondents' demographic characteristics are related to their survey responses. In the present study, attorneys' age was related to their vignette hospitalization decisions. The older the respondent, the less strong the endorsement of involuntary hospitalization (Pearson's r = −0.22, p < .05). Neither attorneys' gender nor level of involvement in involuntary commitment was related to their vignette hospitalization decisions.
After multivariate analysis, two variables remained significant predictors of respondents' vignette judgments about involuntary hospitalization (Table 3). Agreement that lawyers are obliged to respect their clients' interests, even if those interests are harmful, was inversely related to respondents' endorsement of involuntary hospitalization in the vignettes. In addition, the greater percentage of responsibility attributed to individuals for the recurrence of mental illness, the stronger were respondents' recommendations for involuntary hospitalization. Marginally related variables included age, the view that lawyers are obliged to encourage treatment, and concerns about the difficulty of predicting harm.
Influences on Recommending Hospitalization
Involuntary Outpatient Medication Vignette
Another vignette elicited respondents' recommendations that an involuntary outpatient medication hearing be initiated for a person who, without medication, acts increasingly aggressive toward his mother. The vignette states that when taking medication, the individual recovers quickly and has no side effects (Appendix). Respondents' average recommendation to initiate an involuntary medication hearing was 5.2 (SD = 1.8) on a seven‐point scale (1, not at all appropriate; 7, absolutely essential), a fairly strong endorsement for involuntary medication in the community (Table 4). Both state's attorneys' and private practice lawyers' involuntary medication recommendations were significantly stronger than those of publicly funded lawyers (Table 4; one‐way ANOVA, F = 7.24, df = 2, 78, p < .001; Tukey's HSD p < .05).
Vignette Involuntary Medication Recommendations
No relationship existed between attributions of responsibility and involuntary outpatient medication recommendations. Two issues that were related to recommending involuntary hospitalization were also significantly related to recommending involuntary medication. A stepwise multiple regression revealed significant influences of three variables on involuntary medication recommendations (Table 5). A concern that psychiatrists cannot predict the future and must wait for harm before recommending involuntary medication was inversely related to respondents' recommendations for involuntary medication. In addition, respondents who agreed that lawyers are obliged to encourage treatment also were more likely to recommend involuntary medication. Those respondents who self‐identified as publicly funded lawyers were significantly less likely to recommend involuntary medication than were privately funded lawyers and state's attorneys.
Influences on Recommending Involuntary Medication
Discussion
Perceptions of dangerousness strongly predict lawyers' recommendations for involuntary hospitalization. In addition, for the lawyers surveyed, attributions of responsibility are related to their recommendations for involuntary hospitalization. Respondents' practice orientation was related to their involuntary treatment recommendations and to attributions about mental illness. Concerns about beneficence and client autonomy also played a role in the recommendations.
Illinois lawyers' recommendations to hospitalize at levels of escalating risk of harm closely reflect those of Illinois psychiatrists surveyed.3 Neither lawyers nor psychiatrists consider involuntary commitment to be “absolutely essential” unless the risk of harm to the patient or others is imminent. However, the statute governing involuntary commitment specifies that the harm be “reasonably expected…in the near future (italics added).” That the phrase “near future” is not synonymous with “imminent” is demonstrated by the fact that the word “imminent” is used in another section of the Mental Health and Developmental Disabilities Code to define when patients confined in a hospital may be subjected to the involuntary administration of medication in an emergency. The choice of the legislature to use two different phrases relating to the temporal element for future dangerousness demonstrates that these phrases are not intended to be interchangeable. Nor are there any court decisions interpreting the phrase “near future” in Illinois' commitment standard to be synonymous with imminent. Similarly, the United States Supreme Court decision in O'Connor v. Donaldson14 is commonly viewed as the definitive statement on the due process limitation on the substantive standards for involuntary civil commitment. In Donaldson, while limiting involuntary commitment to those who are “not capable of surviving safely in the community”, the Court does not state or suggest any temporal limitation on the states' judgments about that capability.
In terms of attributions of personal responsibility for mental illnesses, Illinois lawyers attribute responsibility to individuals for the recurrence of their mental illness twice as much as for the onset of the illness. Illinois psychiatrists, in turn, rated individuals to be about seven times more responsible for the recurrence of schizophrenia and bipolar disorder than for their onset.6 The difference may be explained by the fact that lawyers attribute responsibility for the onset of mental illness at a higher rate than do psychiatrists. It may also reflect differences between lawyers' and psychiatrists' clinical experience of mental illness and its recurrence.
The study found that for the lawyers surveyed, attributions of responsibility are related to vignette recommendations for involuntary hospitalization. The more lawyers viewed individuals as responsible for the onset and recurrence of mental illness, the more strongly they endorsed involuntary hospitalization for the vignette characters. Attributions of responsibility remained a significant predictor of hospitalization recommendations, even after multivariate analysis. Among psychiatrists surveyed with an almost identical questionnaire, however, there was no relationship between attributions of responsibility and recommendations for involuntary hospitalization.3
The relationship between attributions of responsibility and willingness to recommend involuntary commitment may reflect a perception on the part of lawyers that commitment should be used primarily to vindicate the state's “police power” interest in protecting the public from those persons with mental illnesses who endanger the public. If such persons are responsible for their illnesses, then it is not unfair to deprive them of their liberty. It may also reflect the view of lawyers that hospitalization is unpleasant and at least partially punitive. The more we hold people accountable for their illnesses, the less unfair it may seem to “punish” them with involuntary hospitalization.
This interpretation is supported by the finding that state's attorneys are more apt to hold patients responsible for their illnesses and more apt to support involuntary hospitalization. The primary job of state's attorneys is to prosecute alleged criminals, and the criminal justice system is based on individual responsibility for behavior. It would not be surprising for attitudes related to the core of one's job to spill over into activities, such as involuntary treatment hearings for persons with mental illnesses, which constitute a small fraction of that job.
In addition to attributions of responsibility for mental illness, other attitudes and concerns were found to play a role in lawyers' recommendations for involuntary hospitalization. The more strongly lawyers agreed that they are obligated to encourage treatment (beneficence), the more strongly they recommended involuntary hospitalization in the vignettes. Also, the respondents agreed that lawyers should respect clients' interests (autonomy) and that the potential for harm is difficult to predict.
The present study also investigated the lawyers' attitudes toward involuntary outpatient medication by using a survey vignette. An Illinois statute permits a court to order psychotropic medication (and electroconvulsive therapy) if, following a hearing, it finds that a person with a serious mental illness “lacks the capacity to make a reasoned decision about the treatment” and meets the rest of the statutory criteria. To facilitate treatment in the least restrictive environment and to avoid unnecessary hospitalizations, involuntary medication may be ordered for persons who are being treated in the community as well as on an inpatient basis. (It is important to note that this is not outpatient commitment, since release from a hospital is not conditioned on the patient's agreeing to community treatment, and the failure to comply with court‐ordered community treatment under the Illinois statute cannot be the basis for involuntary hospitalization or rehospitalization. In addition, it avoids the concerns expressed by courts reviewing the constitutionality of outpatient commitment laws, in that there must be a specific finding of incompetence for medication to be imposed [see Urcuyo v. James D.15]). Lawyers recommended involuntary outpatient medication proceedings against the vignette character at levels comparable with endorsement of involuntary hospitalization for a client at imminent risk of harm. This relatively high support for involuntary outpatient medication is not reflective of actual practice in Illinois, where it is rarely used.16 The precise reasons for this rarity are difficult to untangle since an involuntary medication petition will not be filed unless thought advisable by both a lawyer and a physician willing to testify in favor of the petition. That involuntary outpatient medication orders are not sought by physicians may reflect feedback given them by lawyers or the physicians' own views. This topic may warrant further study of physicians and lawyers.
The findings represent a purposive sample of lawyers involved in involuntary commitment. While the findings may not generalize to all lawyers in Illinois, the sampling strategy was intended to produce responses that would speak to the experiences and attitudes of lawyers involved in the actual practice of involuntary commitment. Also, because subjects responded to hypothetical commitment scenarios, practical factors that may impinge on actual decision‐making (such as availability of resources and patients' gender) were not considered in the present study. The response rate of 48 percent (n = 89) reflects another limitation that is common in mail surveys of professionals. Further, only one‐fourth of respondents identified themselves as regularly involved in commitment proceedings.
Conclusions
In the absence of imminent risk of harm, lawyers were reluctant to hospitalize. This mirrors psychiatrists' judgments in similar vignettes (previously published3). Among lawyers, attributions of personal responsibility for mental illness were related to willingness to commit persons with mental illness. In this respect, lawyers resemble the general public more than psychiatrists, for whom no relationship was detected between attributions of responsibility and willingness to commit. Lawyers' practice orientation was related to their hospitalization and medication decisions and to attributions about mental illness.
Further research is needed to explore the meaning of the relationship between attributions of responsibility for mental illness and lawyers' willingness to hospitalize persons with mental illness. Those lawyers regularly involved in commitment proceedings should be oversampled in future studies to gain a better understanding of the attitudes of those attorneys whose actions have the most impact on the real lives of individuals living with severe mental illness. Finally, findings from this and further research should be employed in future education and training of attorneys involved in mental health law.
Appendix Survey Vignettes
Vignette 1: Self‐Harm Scenario
There may be different interpretations of when a person meets the criteria for involuntary hospitalization. Please read each of the situations below and rate how appropriate you think initiating involuntary commitment proceedings would be for the person described, by circling a number from 1 to 7. Also, for each situation, indicate to what degree different legal considerations played a role in your judgment about involuntary hospitalization by circling a number on the scale following each statement.
Fred is a 35‐year‐old man with serious and persistent mental illness. He has a long history of hospitalizations and, despite doing well in the hospital, he deteriorates quickly after he leaves the hospital. This pattern has repeated itself three times in the last year and each time Fred had to be rehospitalized within one month of discharge because he could not meet his basic physical needs.
Situation 1. Fred left the hospital about a month ago but has not yet begun to deteriorate in self‐care. How appropriate would it be at this time to initiate involuntary commitment proceedings for Fred?
Situation 2. Fred left the hospital about a month ago and is now showing obvious deficits in his ability to meet his basic needs, but these deficits do not yet endanger him. How appropriate would it be at this time to initiate involuntary commitment proceedings for Fred?
Situation 3. Fred left the hospital about a month ago and is showing obvious deficits in his ability to meet his basic needs and these deficits are beginning to endanger him but he is not yet at imminent risk of serious harm. How appropriate would it be at this time to initiate involuntary commitment proceedings for Fred?
Situation 4. Fred left the hospital about a month ago and is showing obvious deficits in his ability to meet his basic needs and these deficits are beginning to endanger him. He is at imminent risk of serious harm but he is not yet seriously harmed. How appropriate would it be at this time to initiate involuntary commitment proceedings for Fred?
1.......2......3......4......5.......6.......7
Involuntary Hospitalization
Involuntary Hospitalization
Not at All Appropriate
Absolutely Essential
Consideration 1. There is a good chance that I will be unable to find a mental health professional willing to testify in favor of the involuntary commitment of this person.
Consideration 2. Judges are unwilling to commit such a person.
1.......2......3......4......5.......6.......7
Played no role in my judgment
Played a significant role in my
about involuntary
judgment about involuntary
hospitalization
hospitalization
Vignette 2: Harm to Others
Bob is a 35‐year‐old man with serious and persistent mental illness. He has a long history of hospitalizations and, despite doing well in the hospital, he becomes aggressive and attacks his 70‐year‐old mother after he leaves the hospital. This pattern has repeated itself three times in the last year and, each time, Bob had to be rehospitalized within one month of discharge because of his violent behavior toward his mother.
Situation 1. Bob left the hospital about a month ago and has not yet begun to show increased irritability. How appropriate would it be at this time to initiate involuntary commitment proceedings for Bob?
Situation 2. Bob left the hospital about a month ago and is showing obvious increases in irritability, but has not yet been verbally abusive. How appropriate would it be at this time to initiate involuntary commitment proceedings for Bob?
Situation 3. Bob left the hospital about a month ago and is showing obvious increases in irritability. He has become verbally threatening but not physically abusive. How appropriate would it be at this time to initiate involuntary commitment proceedings for Bob?
Situation 4. Bob left the hospital about a month ago and is showing obvious increases in irritability. He has become verbally threatening and has begun to push and shove his mother but has not yet seriously injured her. How appropriate would it be at this time to initiate involuntary commitment proceedings for Bob?
1.......2......3......4......5.......6.......7
Involuntary Hospitalization
Involuntary Hospitalization
Not at All Appropriate
Absolutely Essential
Consideration 1. There is a good chance that I will be unable to find a mental health professional willing to testify in favor of the involuntary commitment of this person.
Consideration 2. Judges are unwilling to commit such a person.
1.......2......3......4......5.......6.......7
Played no role in my judgment
Played a significant role in my
about involuntary
judgment about involuntary
hospitalization
hospitalization
Vignette 3: Involuntary Medication
Illinois law permits a person with a serious mental illness to be subjected to court‐ordered involuntary treatment with psychotropic medications if:
The person exhibits deterioration of his or her ability to function, suffering, or threatening behavior due to a serious mental illness.
The illness has existed for a period marked by the continuing presence of the symptoms described in Paragraph 1 above or the repeated episodic occurrence of these symptoms.
The benefits of the medication outweigh the harm.
The person lacks the capacity to make a reasoned decision about the treatment.
Other less restrictive services have been explored and found inappropriate.
Please read the situation described below and rate how appropriate you think initiating court‐ordered medication, to be administered in the community, would be for the person described, by circling a number from 1 to 7. Also indicate to what degree different considerations played a role in your judgment about involuntary medication.
Chris is a 35‐year‐old man with serious and persistent mental illness. He has a long history of hospitalizations and, despite doing well in the hospital, he deteriorates quickly after he leaves the hospital, primarily because he stops taking his medication. He becomes aggressive and attacks his 70‐year‐old mother. This pattern has repeated itself three times in the last year and each time Chris had to be rehospitalized within one month of discharge because of his violent behavior toward his mother. Once hospitalized and given medication, Chris recovers quickly and the medications have caused no reported side effects. Chris is otherwise in good physical health. Chris left the hospital about a month ago, stopped taking his medication one week later, and has begun having delusions that his mother is poisoning him, the usual prelude to an attack against her. The main reason he stopped taking his medication is that he also believes that all medicines are poison. How appropriate would it beto initiate an involuntary medication hearing for Chris?
1.......2......3......4......5.......6.......7
Involuntary Medication
Involuntary Medication
Not at All Appropriate
Absolutely Essential
2. Consideration 1. There is a good chance that I will be unable to find a mental health professional willing to testify in favor of the involuntary commitment for this person.
3. Consideration 2. Judges are unwilling to order medication for such a person.
4. Consideration 3. There is a good chance that I will be unable to find a mental health professional willing to treat such a person under court order.
5. Consideration 4. It may be difficult to enforce an order for involuntary treatment.
1.......2......3......4......5.......6.......7
Played no role in my judgment
Played a significant role in my
about involuntary
judgment about involuntary
hospitalization
hospitalization
Footnotes
-
Supported in part by an NIH‐NIMH Research Infrastructure Support Program Grant MH‐62198, Principal Investigator, Patrick Corrigan.
- American Academy of Psychiatry and the Law





{kind=link}