


Abstract
The defense of involuntary intoxication has long been an exception to the general notion that intoxication is not a defense to criminal liability. The consumption of medications prescribed by a physician can form the basis of an involuntary-intoxication defense. In this article, I review cases where defendants relied on the use of prescribed medications for an involuntary-intoxication defense. The medications most frequently implicated by defendants are listed by name and by class. From the case law, I provide a summary of the defense and a review of the pitfalls of the defense to serve as practice pointers for forensic evaluators.
That if a person by the unskilfulness of his physician, or by the contrivance of his enemies, eat or drink such a thing as causeth such a temporary or permanent phrenzy, as aconitum or nux vomica, this puts him into the same condition, in reference to crimes, as any other phrenzy, and equally excuseth him.1
In most jurisdictions, a criminal defendant may be excused from responsibility if he commits a wrongful act because of involuntary intoxication. Although relatively rare a quarter century ago, the defense of involuntary intoxication has steadily gained momentum among criminal defendants.2 The defense is based on the common-law premise that someone who ingests an intoxicant unknowingly or without awareness of its possible effects is not blameworthy. A defendant may become involuntarily intoxicated through the fault of another, by accident or inadvertence, or because of a physiological or psychological condition beyond his control. Although the term intoxication is generally associated with the ingestion of alcohol, the law recognizes that it could include any drug or substance with adverse effects, including prescribed medications. The Model Penal Code, for example, explicitly recognizes the involuntary-intoxication defense in the context of use of prescription medication.3
In this article, I review the legal aspects of the involuntary-intoxication defense for defendants who assert that their criminal acts were caused by intoxication with prescription medications. I review the United States criminal federal and state appellate case law on this topic. Identified are the medications most claimed by defendants who assert involuntary intoxication as identified in the appellate case law. Based on the legal cases, I also summarize the key aspects that negate a defense of involuntary intoxication and use legal case examples to highlight principles relevant to the forensic evaluator.
Methods
A legal search of all state and federal criminal cases was performed by using the following search terms to query LexisNexis for cases involving prescription medications (with one of the listed terms having to occur at least five times in the cases): medication, prescription, psychotropic, drug, substance, and chemical. The search instruction used was “atleast5(medication!);” derivatives were used for the related search words mentioned. I combined these search terms (using connector “AND”) with decisions pertaining to involuntary intoxication. Again, the search required one of any of the following words to occur at least five times (using an instruction, as above): involuntary intoxication, criminal responsibility, temporary insanity, and insanity. This method was selected to identify cases in which the involuntary-intoxication defense was a main topic of the opinion. Appellate cases often have headnotes (included in the database search of terms) and often address multiple matters, and this method was used to target relevant case law. This search method has been used by other researchers seeking published legal opinions.4 The search included all cases through December 2012.
The LexisNexis database includes federal district court, circuit court of appeals, and Supreme Court opinions, as well as state appellate and supreme court opinions. The database Federal and State Cases Combined was selected, because it has the most complete listing of published cases. State trial court cases were not included in the database. Because case law is based on published legal opinions, the material largely included contested points of law regarding the applicability of the involuntary intoxication defense. Pretrial motions and trial-level verdicts are generally not published unless they are appealed. It is noteworthy that many of the cases reviewed preferentially involved defendants whose defense of involuntary intoxication was initially excluded or for which the court did not include a jury instruction on the point. Cases in which the criminal defendant was successful in the claim of involuntary intoxication at trial were infrequent.
Results
The LexisNexis database search generated 219 cases. Figure 1 illustrates the number of appellate cases by decade: 5 cases before 1960, 3 cases from 1960 through 1969, 16 cases from 1970 through 1979, 32 cases from 1980 through 1989, 35 cases from 1990 through 1999, 83 cases from 2000 through 2009, and 45 cases since 2010. Because appellate cases lag behind trial court cases and only a percentage of trial-level cases are appealed, the numbers of appellate cases do not mirror exactly the total number of cases where a defense of involuntary intoxication has been used. Statistics in federal criminal appeals5 and from the California State Court Statistics Reports6 generally support an overall increase in the number of criminal cases appealed. The trend of increasing appellate cases identified by the LexisNexis search supports the literature stating that there is an increase in cases in which defendants raise the involuntary-intoxication defense at trial.2
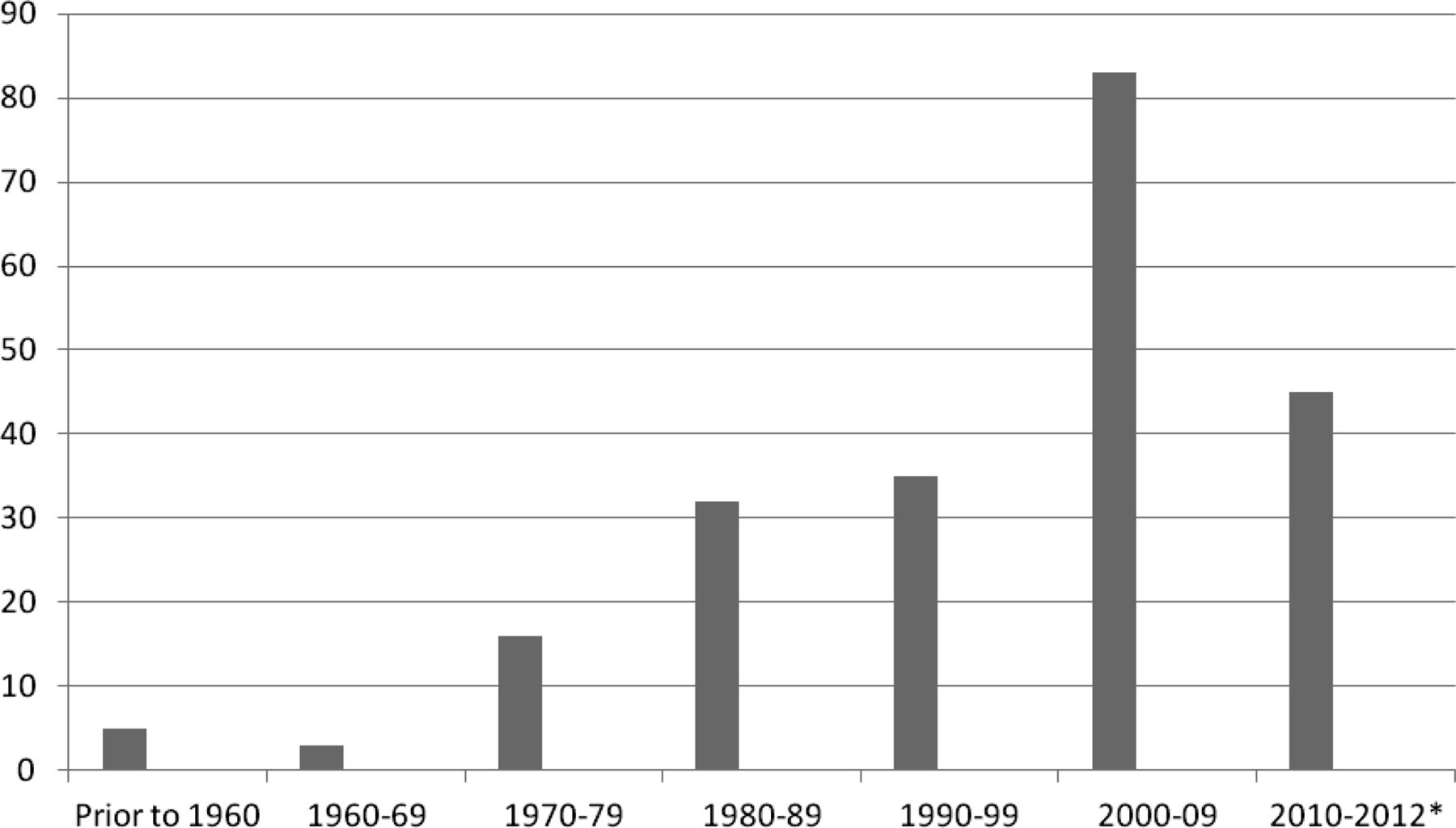
Number of appellate cases by decade. *The search included cases through December 2012.
Several cases were excluded from further review, includes 39 because they were unpublished opinions. I elected to exclude the unpublished opinions to focus on those cases that could provide precedent for future cases and be informative for forensic practitioners. The term drug was used as an initial search term because some courts used drug synonymously with medication. As expected, this method yielded numerous cases involving illicit substances. Sixty cases were excluded because they advanced a defense based solely on intoxication by an illicit substance. Twenty-two cases solely involving a criminal defendant's use of medication to show voluntary intoxication or diminished capacity or as a mitigation of sentence were excluded from this review.
The LexisNexis search produced 98 relevant legal cases. Of those, the cases involved the following criminal offenses: 50 violent crimes, 22 driving-related charges, 17 theft-related offenses, 3 criminal threats, and 6 other charges (such as fraternization and forgery). A review of the cases by state revealed that two-thirds of the states (33 states) had at least 1 state appellate case involving the defense of involuntary intoxication. Only one state, Florida, had more than 10 appellate cases where a defendant had claimed the defense.
Table 1 illustrates the criminal cases by intoxicating agent included: 45 sedative hypnotics and narcotics, 18 antidepressants, 6 stimulants (including dietary aids), 3 steroids, 2 physician-instructed over-the-counter remedies, 1 antipsychotic, and 9 miscellaneous agents (e.g., insulin, folic acid, and antihypertensives). In nine cases, the defendant asserted a defense based on the combined effects of psychotropic medications from more than one class of drug. Finally, in seven cases, the medication was not clearly identified, but rather referred to generally as a psychotropic drug or as medication. The hypnotics and narcotics were grouped together because of the large percentage of cases in which the defendant used a combination of those medications.
Cases by Intoxicating Agent
As stated earlier, the legal cases reviewed for this article preferentially involved defendants whose assertion of involuntary intoxication was unsuccessful at trial. By way of illustration, the LexisNexis search yielded 18 cases where the defendant alleged that an antidepressant medication caused his criminal behavior. In each of these, at the trial level, the defendant either failed to meet his burden to warrant a jury instruction on the defense, or the trier of fact rejected the defense of involuntary intoxication. In the 18 cases, defendants reported that the following medications caused their conduct: sertraline (Zoloft), 7 cases; fluoxetine (Prozac), 4; paroxetine (Paxil), 3; perphenazine and amitriptyline (Triavil), 2; and venlafaxine (Effexor), 1; 1 case listed antidepressants generically. The Triavil cases were included in the antidepressant category because the cases focused on the antidepressant properties of the medication. Of the 18 appellate cases, only 2 were reversed and remanded for further proceedings on the question of involuntary intoxication.7,8 In both cases, the court held that there was sufficient evidence in the record to warrant a jury instruction on the topic.
Of the remaining 16 cases, in 12 the courts upheld the trial court proceeding because the defendant offered insufficient proof or there was direct evidence that negated the involuntary-intoxication defense (see, e.g., Ref. 9). In two cases higher courts addressed as a matter of law the legal standard for the defense in their jurisdiction.10,11 Finding that the trial courts had properly instructed the jury on the defense, they upheld the defendants' criminal convictions. Finally, in two cases rulings on the question were superseded by cases already taken into account in this discussion.
A review of the involuntary-intoxication defense follows, with practice pointers for the forensic evaluator.
The Excuse of Involuntary Intoxication
In common law, voluntary intoxication was never a defense to criminal liability. The defense of involuntary intoxication, in contrast, was a complete defense to liability if the intoxicant caused the defendant to become temporarily insane.12 To be successful, the defendant had to establish that he did not know that he had consumed an intoxicating substance or that he had not been aware of its intoxicating properties when he ingested it. The common law generally recognized involuntary intoxication when any of the following conditions was met: the intoxication was coerced or the result of duress, was pathological, was caused by a substance taken pursuant to a physician's advice, or was the result of an innocent mistake by the accused as to the intoxicating effects of the substance.13 This review is limited to medically prescribed intoxicants.
Today, jurisdictions vary in their approach to involuntary intoxication. Some states have adopted the affirmative defense in their criminal codes. Others rely on judicial opinion. There are some jurisdictions that have yet to recognize the defense explicitly. In general, however, courts have upheld the defense when three elements are proved: that the defendant was intoxicated; that the intoxication was involuntary; and that, as a result of the involuntary intoxication, the defendant's mental state met the jurisdiction's test for insanity (Ref. 13, p 638). It is an affirmative defense, meaning that the defendant admits to the criminal act and is seeking to be excused from liability.
Where a defendant claims intoxication from prescribed medications, courts generally allow the trier of fact to assume that an intoxicating dose would not be prescribed or administered by a physician. In one of the earliest cases on the topic, Perkins v. United States,14 the Supreme Court stated that if a defendant commits an offense while in a mental state amounting to insanity that was induced by a drug prescribed by a doctor, taken in good faith and in accordance with the prescription, then he is not guilty of the offense. In Perkins, a federal appellate court reversed a conviction of manslaughter when the defendant put forth evidence of delirium caused by chloral hydrate prescribed for nervousness.
In Minneapolis v. Altimus,12 a case cited as initiating the modern defense of involuntary intoxication, the defendant argued that he was not criminally responsible for driving under the influence of diazepam (Valium) because he was not aware of the side effects of intoxication. The Minnesota Supreme Court outlined three requirements for involuntary intoxication with prescribed medications: that the defendant did not know, or have reason to know, of the intoxicating effects of the medication; that the prescribed medication, not an alternate substance, caused the criminal behavior; and that the defendant can establish that insanity was induced by the medication (Ref. 12, p 857).
Of note, jurisdictions vary in whether the defense of involuntary intoxication may be applied to strict-liability offenses. Criminal offenses are generally classified into general, specific-intent, or strict-liability, crimes. To prove a defendant liable for specific intent, the prosecution must prove mens rea. Involuntary intoxication is generally a complete defense to any crime of intent. In contrast to Minneapolis v. Altimus, other courts have held that the defense is not applicable to strict-liability offenses (where proof of a culpable mental state is not required), such as driving under the influence (see, e.g., Refs. 15, 16).
The defense of involuntary intoxication is attractive to defendants because it is a complete defense. As described by Daley et al.,17 a criminal defendant may raise his use of medications to show voluntary intoxication or mitigation of penalty. The comments and practice pointers that follow are specific to the defense of involuntary intoxication.
Practice Pointers
The major challenge to defendants relying on the defense is one of proof. Because it requires the defendant to establish intoxication, involuntariness, and legal insanity, defendants seldom meet their burden (Ref. 12, p 858). The following summarizes key pitfalls in the defense, as obtained through the appellate case review, and provides recommendations to assist the forensic evaluator who is consulted on such cases. As already stated, there are jurisdictional differences regarding the applicability of this defense, and, accordingly, evaluators should familiarize themselves with the laws of the appropriate jurisdiction.
Ingestion
Whether a defendant's criminal conduct should be excused by reason of involuntary intoxication is ultimately a question for the trier of fact. A necessary predicate to this defense is actual ingestion of the claimed substance or medication. As with any forensic evaluation, the examiner is cautioned about relying on the word of the defendant as to whether he ingested the medication before the criminal offense. In some of the cases reviewed for this article, psychiatric experts opined that a defendant's behavior was due to involuntary intoxication, only to have the opinion ultimately rejected because of evidence that the defendant did not take the claimed substance before the offense. For example, in Corp v. Sec. Fla. Dept. of Corr.,18 the defendant failed to show a reasonable probability of involuntary intoxication, because evidence showed that he was not compliant with the prescription at the time of murder.
Similarly, Illinois v. Bartgen19 involved a case where a defendant had claimed involuntary intoxication by a prescription antidepressant, paroxetine, but was convicted of two counts of attempted murder. In upholding the trial verdict, the appellate court relied in part on the fact that the only evidence showing that the defendant ingested paroxetine was jail records that had been made after the defendant's arrest.
Collateral sources may corroborate or fail to confirm the defendant's assertion. For ingestion, helpful information may include: toxicology reports, witness statements, evidence that the medication prescribed was filled, whether the number of pills remaining is consistent with the defendant's account, and the defendant's statements about substance and medication use near the time of the offense.
Medication Misuse
When the intoxication is caused by an overdose or misuse of the medication, courts are inclined to hold the defendant culpable. A case commonly discussed in law schools, People v. Chaffey,20 is illustrative. In Chaffey, the defendant took 120 alprazolam (Xanax) tablets in an attempted suicide and then drove recklessly while in an intoxicated state. She had been prescribed one to two tablets daily for anxiety and insomnia, and the medication label had warned her of possible drowsiness. The court held that the defendant voluntarily ingested the medications (in contrast to involuntary administration), and the defendant was convicted of the driving offense.
In contrast, in Perkins v. United States, the defendant killed a passenger on a steamship after consuming excessive chloral hydrate. The court stated that the defendant is “bound to take notice of the warning appearing on the prescription,” but is nevertheless not culpable if he had no reason to anticipate the side effects (Ref. 14, pp 415–16). In People v. Turner,21 a defendant appealed his conviction for robbery on the basis that he had consumed approximately 25 butalbital/aspirin/caffeine (Fiorinal) tablets for a headache before the offense. The defendant argued that he had mistakenly consumed an overdose because the medication had been prescribed “as needed”; he had taken multiple tablets before without adverse effect; and he had never been warned about an excessive dose. The appellate court noted that the evidence against culpability was meager; nevertheless it reversed to allow an instruction on involuntary intoxication to go to the jury. Some would argue, in contrast, that the mere fact that a medication requires a prescription puts the defendant on notice that an excessive dose could have ill effects.22
Concomitant Use of Medication With Alcohol or Illicit Drugs
It is not uncommon for a defendant relying on the involuntary-intoxication defense to have consumed both medication and alcohol or illegal drugs. For example, the LexisNexis search for this review produced 45 cases in which the defendants claimed that a sedative hypnotic or narcotic caused their aberrant behavior. In 20 of the 45 cases, the defendants had ingested alcohol, illicit substances, or both, in addition to medication.
In contrast to the widely held belief that voluntary ingestion of alcohol or other illicit substances negates an involuntary-intoxication defense, courts are not uniform in their approach to involuntary intoxication where the intoxication is caused by a combination of medication and alcohol or recreational drugs. In many cases, intoxication resulting from a combination of medication and alcohol or recreational drugs is treated as a voluntary ingestion, thus negating a defense of involuntary intoxication. In State v. Bunn,23 where the defendant shot two persons after consuming alcohol and diazepam, the court stated that only when alcohol is introduced into a person's system by force majeure will the intoxication be considered involuntary. Courts presume that a defendant who consumes alcohol or illegal drugs knows or should know the potential to cause intoxication (Ref. 17, p 538). Similarly, the appellate court held in People v. Gerrior24 that a defendant who knew about the nature of the prescribed medication he was taking and had been told of the potential extreme reaction if taken with alcohol was voluntarily, not involuntarily, intoxicated when he, in fact, consumed both the medication and alcohol.
People v. McMillen25 involved a defendant who claimed involuntary intoxication due to the combined effects of “a mixture of psychotropic prescribed medications along with an illegal substance” (Ref. 25, p 412). On the date of the offense (murder), the defendant and victim had consumed more than an “eight ball” of cocaine (3.5 g, or one-eighth ounce) together. The court stated that the knowing, or voluntary, ingestion of cocaine or other illicit drugs precludes the use of the defense of involuntary intoxication. The court added:
Here, we take as true … the defendant's claim that he was not warned by a physician of the adverse side effects that my result from taking four prescription medications and ingesting an “eight ball” of cocaine. Any potential adverse effects that resulted, however, may not be considered unknown and, in fact, are so obvious that a warning need not be made by a physician [Ref. 25, at 417].
On the other hand, when an individual takes a prescribed medication and has no reason to anticipate that intoxication will result when the medication is taken with alcohol or another drug, the intoxication may be considered involuntary by some courts. In People v, Murray,26 the defendant ingested “goof balls” (thioridazine) with alcohol before escaping from a state institution. The court stated that an involuntary-intoxication defense may go forward where a defendant, if believed, did not customarily consume alcohol and had never previously ingested the substances together or was unfamiliar with the combined effects.
Prior Experience
Along similar lines, the involuntary intoxication defense is generally not available for defendants who knew or should have known, based on warnings or prior experience, of the consequences of taking the prescribed medication.12 This scenario can occur when an individual continues to take a prescribed medication after a physician warns of the medication's side effects and the person begins to experience those effects. Similarly, defendants are presumed to have knowledge if they had a prior adverse reaction to the prescribed medication.
A case from the Court of Appeals for the Armed Forces, United States v. Hensler,27 is illustrative. The accused was charged with engaging in misconduct with enlisted personnel on six occasions. She claimed that, among other triggers, a combination of prescribed medications and alcohol caused her behavior. She was given a general instruction about criminal responsibility at trial, but was not given a specific instruction about involuntary intoxication. The court held that failure to give a specific instruction was an error as to the accused's first instance of misconduct, but not as to subsequent acts. The “defense was not raised as to the remaining five episodes because [after the first episode] the appellate was on notice that she reacted inappropriately to consumption of alcohol” in this setting (Ref. 27, p 196).
Although I did not identify any specific legal case that addressed prior knowledge of a defendant's drug or alcohol abuse, it is foreseeable that the defendant would be expected to have knowledge of the effect of medication in a class of medications that had had an intoxicating effect on him, if adequately warned. Outside the scope of this article is a detailed discussion of the physician's responsibility to inform patients about their medications, but certainly the adequacy of any warning would bear on what the defendant knew about the ingested medication.
Central to these last three categories, medication misuse, concomitant use of medication with alcohol or illicit drugs, and prior experience, is the concept of foreseeability. In other words, courts consider what the defendant should have reasonably been expected to know about the effects of the ingested medication. The forensic evaluator may be in a unique position to assess the foreseeability of ingestion and subsequent behavior. For the expert evaluator, items to consider may include whether the defendant consumed the medication (or combination of substances) for its intoxicating effect, whether there were adequate warnings on medication labels or product inserts, whether there had been sufficient warnings from a physician or other medical provider, whether the defendant had received warnings from others who had experience with the medication, whether the medication was obtained legally or illegally, whether the medication was taken against the advice of a physician, and whether the defendant had prior experiences with the medication or similar substances.
Expert Understanding of the Claimed Medication
Although it is reflected in only a small number of appellate cases, the expert has a key role in educating the trier of fact about the medication, mechanism of action, and behavior occurrences associated with the medication. The appellate literature suggests that psychotropic medications are commonly cited by criminal defendants using this defense (Table 1), and forensic psychiatrists will be called to explain the role of many medications. It is beyond the scope of this article to outline all claimed medications and discuss their pharmacologic properties. In United States v. Hensler 27 (discussed earlier), the expert put forth the combined effects of the accused's medications, alcohol, and the role of her hepatitis diagnosis (with impaired drug metabolism) as important factors in her defense of involuntary intoxication. In some cases, the expert witness can explain subsequence versus causative effects of a medication.
The expert will want to be aware of the claimed medication's indications and other common uses, known side effects, onset of action and half-life, and any label (black-box) warnings. Useful in some cases is toxicology information from blood samples that can verify last dose or time of medication of some substances. Additional helpful resources may include the prescribing information from the U.S. Food and Drug Administration (FDA), information on the drug–drug interactions, medical literature on the medication, and consultation with pharmacologists and toxicologists.
Insanity
As stated earlier, the defendant must prove that the involuntary intoxication resulted in a mental state amounting to insanity at the time of the criminal act. Most jurisdictions use a traditional test for insanity for involuntary intoxication. The difference between insanity and involuntary intoxication lies in the cause of the mental state. “For the former, a mental disease or defect is required, for the latter, involuntarily caused intoxication” (Ref. 28, p 254).
It is not uncommon for defendants to present sufficient evidence of ingestion and involuntary consumption of a medication, but fail in their defense on the insanity prong. For example, in Brancaccio v. State,29 the court stated that the defendant presented evidence that he was experiencing negative effects from having ingested sertraline (Zoloft) at the time of the murder. The court specifically found, however, that, at the time of the offense, the defendant knew the wrongfulness of his actions and took measures to avoid detection, negating the prong of insanity. As with traditional insanity cases, it is important that the forensic evaluator not equate intoxication with insanity. The psychiatric expert should become familiar with the insanity standard as it relates to involuntary intoxication in the applicable jurisdiction.
Limitations
As mentioned in the Results section, appellate cases reflect a percentage of trial level cases. However, the percentage of cases appealed in this context is not readily available, as courts do not generally break down trial court cases by type in their statistical databases, and case filings do not equate with case dispositions, because they include procedures such as dismissals and plea bargains.
Further, because of the nature of criminal appeals, those cases most likely appealed in this context involve those in which the criminal defendant was not successful in his defense of involuntary intoxication at the trial level. Few of the cases included in this study involved a situation where the prosecution appealed a decision. Given the limited number of appellate cases identified, trends within local jurisdictions were not observable.
Highlighted are principles obtained from reviewing the published appellate cases. Forensic psychiatrists and other evaluators should note that the medications identified in this review are those that have been represented in appellate-level cases, but this list should not be considered exhaustive of the types of medications that defendants may use in claiming the defense of involuntary intoxication. Additional research is needed to assess the frequency of the use of the defense, rates, and types of medications used in the defense and forensic evaluator experience with the defense. The addition of the chapter, “Medication-Induced Movement Disorders and Other Adverse Effects of Medication,” to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition,30 raises the possibility of increased interest by defendants and lawyers in mounting medication-related defenses.
Conclusion
Knowledgeable legal counsel increasingly use the defense of involuntary intoxication. It is not surprising, then, that forensic evaluators are called on to act as expert witnesses and to opine about the defendant's criminal responsibility in such cases. When an examinee asserts the defense or announces a history of having taken prescribed medications near the time of the offense, the expert has a key role in assessing whether such medications affected the defendant's mental state at the time of the offense. As identified in the appellate cases reviewed for this article, psychotropic medications are most commonly used by defendants in claims of involuntary intoxication.
I have reviewed some of the common pitfalls of the defense related to prescribed medications, to guide evaluators asked to consult on such cases: proof of ingestion; misuse of the claimed medication; concomitant use of the medication with alcohol or illicit drugs; defendant's prior experience with the medication; evidence of pharmacologic properties of the claimed medication; and meeting the requirements for legal insanity. A key concept central to several of these pitfalls is that of foreseeability. An expert may be particularly helpful in addressing this concept by reviewing the defendant's previous behavior, his experience with the medication, known warnings about the medication, and any discussion the defendant had with a physician about the potential risks of the medication. Not only do psychiatrists have expertise in psychotropic medications and their anticipated effects, forensic psychiatric evaluators are in a unique position to assist the courts because of their experience in assessing mental state at the time of the crime.
Footnotes
Disclosure of financial or other conflicts of interest: None.
- © 2015 American Academy of Psychiatry and the Law





{kind=link}