


Abstract
Competency to stand trial (CST) assessment of juvenile offenders is a relatively recent phenomenon, as are juvenile mental health courts. Factors associated with youths' ability to participate in legal proceedings are not well understood, regardless of the court venue. Using a sample of 324 juveniles participating in the Los Angeles County Juvenile Mental Health Court (LAJMHC), we sought to explore the relationships of age, mental health diagnosis, and history of mental health treatment to CST status. Results suggest youths under the age of 15 were significantly more likely to have been found incompetent to stand trial (IST) when compared with older youths (p = .007). Youths with a diagnosis of a pervasive developmental disorder or intellectual disability were also more likely to be found IST than those without these diagnoses (p = .02 and p = .0001, respectively). Conversely, participants aged 16 or 17 years and diagnosed with a mood, substance abuse, or psychotic disorder were more likely to be found CST than those without these diagnoses (p < .0001, p = .035, and p = .0064, respectively). Participants with a history of psychotherapy or psychotropic medication were more likely to be found CST than were those without any treatment history (p < .0001). Further research on factors that affect CST status in juveniles who participate in mental health courts may be particularly salient to improve understanding of specific treatment and rehabilitative needs of youthful offenders, and to inform approaches to competency attainment and recidivism prevention services, both within these specialty courts and in juvenile proceedings in general.
The impact of mental disorders, developmental disabilities, and developmental immaturity on competency to stand trial (CST) status in young offenders has increasingly gained national attention over the past decade. In part, the interest in juvenile CST can be explained by the large number of youths in whom various factors may impair competency to proceed and the unique nature of these impairments relative to adult defendants. Like adults, many juveniles possess significant cognitive and psychiatric impairments that may render them incompetent to stand trial (IST).1 Prevalence estimates of psychiatric illness in the juvenile justice population have been found to range from 66 to 75 percent,2 and estimates of youths who meet the criteria for a developmental disability or intellectual impairment range from 30 to 70 percent.3 Although conservative estimates of the rate of serious mental illness among juvenile offenders range from 15 to 20 percent, many studies have indicated that this number is probably higher.4
As in adults, intellectual impairments, learning disabilities, and certain mental illnesses have been correlated with impaired adjudicative competency in youths.5,–,7 A large multisite study of youths aged 11 to 24 showed that, in terms of general intelligence, 40 percent of those with a full-scale IQ score between 60 and 74, and 25 percent of those with an IQ score between 75 and 89, showed significant impairment in CST capabilities.5 Similarly, in a sample of psychiatric patients aged 10 to 17 years, a learning disorder or intellectual disability diagnosis correlated with low scores on the Understanding and Reasoning sections of the MacArthur Competence Assessment Tool–Criminal Adjudication, a standardized means of assessing CST.6 A significant association between intellectual deficits and an IST designation has also been reported in a population of detained youths aged 9 to 18 years.8 A history of mental health treatment has also been significantly associated with IST status among 12- to 16-year-old, preadjudicatory defendants who were found to be IST.7 Other studies have suggested that psychopathology, including communication deficits associated with attention deficit hyperactivity disorder and suicidality may affect CST status in youth.6,9,10
Research also suggests that some youths will manifest deficits in legally relevant abilities for reasons of age alone (i.e., developmental immaturity).5,11 In their often cited large multisite study investigating correlates of CST in detained and nondetained participants aged 11 to 24 years, Grisso et al.5 found that approximately one-third of 11- to 13-year-olds and one-fifth of 14- to 15-year-olds were impaired in capacities relevant to adjudicative competence, much like seriously mentally ill adults who most likely would be judged IST; those aged 16 to 17 years did not differ significantly from young adults in terms of CST status. Other studies of detained youths have found that close to 35 percent of 11- to 13-year-olds and 22 percent of 14- to 15-year-olds were impaired in the areas of understanding and reasoning of trial-related matters, and youths aged 11 to 13 years demonstrated less ability to focus on the long-term consequences of their decisions.8,12
The extant literature indicates that a wide variety of techniques are used in evaluations of a juvenile's CST status and that many juveniles with potential psychiatric and developmental disorders may be overlooked in evaluations of competency.13 The evaluative process of determining a youth's CST status may reveal important data about treatment needs of highly vulnerable youths who may not otherwise be formally assessed or have had prior access to mental health treatment. This lack of treatment may uniquely affect youths who identify as racial and ethnic minorities who, compared with their nonminority peers, are more likely to be referred to the juvenile justice system and are less likely to have received mental health services.14,15 Findings regarding the relationship between age, social factors, and mental illness may be particularly useful in informing recommendations for youths who are currently considered IST for reasons of developmental immaturity and for whom other unidentified factors may also influence these deficits.
Juvenile Mental Health Court and Competency to Stand Trial
Juvenile mental health courts represent an emerging judicial approach that provide a unique diversionary context in which to evaluate factors associated with competency status in juveniles. Participants of these courts are typically justice-involved youths who have been identified as having significant psychiatric, cognitive, and behavioral symptoms and diagnoses that warrant specialized intervention and services.16 In particular, this population is an important group to study, as their diagnoses may confer additional vulnerabilities that increase their risk of impairments in adjudicative competence. Moreover, to the extent that mental illness and intellectual and developmental disabilities increase the risk for a legal determination of IST, analysis of young offenders participating in juvenile mental health courts may be particularly useful given the prevalence of these diagnoses in specialty courts.
We wanted to describe sample characteristics and examine the relationships of age, mental health and developmental disability diagnoses and history of mental health treatment to competency status in youths whose cases were accepted by the Los Angeles County Juvenile Mental Health Court (LAJMHC) between 2005 and 2009.
Methods
Study Sample and Selection Criteria
The study sample comprised 324 male and female youthful offenders, aged 8 to 22 years, who were participants in the LAJMHC from 2005 through 2009. The original sample included all 422 juveniles who were screened for eligibility and suitability to participate in the LAJMHC during this period. Ninety-eight youths were excluded from the current study after being determined unsuitable for participation in the LAJMHC by the multidisciplinary court team. Permission to conduct the study was granted by the UCLA Institutional Review Board, Office of the Human Research Protection Program and through the Los Angeles County Dependency and Delinquency court system.
The LAJMHC is a postadjudication full-time specialty court and functions as a multidisciplinary team that includes a judge, district attorney, public defender, alternate public defender, psychologist, psychiatrist, educational advocate, probation officers, and a psychiatric social worker.17 Youths with mental or developmental conditions who may benefit from the multidisciplinary services provided by the LAJHMC can be referred by defense attorneys or judges within the Los Angeles County Juvenile Delinquency court system. Juveniles are always presumed to be competent unless there is a doubt raised by counsel or the judge. For juveniles referred to the LAJMHC, if the question of competency to stand trial has been raised at all, the evaluation and determination of the minor's CST status has been made by the court of origin before referral to the LAJMHC. The LAJMHC will accept juveniles regardless of their CST status, however, and accordingly, the population includes both youths previously found CST who enter the program after adjudication and those found IST who enter the program with proceedings suspended.
Although most participants have received a diagnosis of a major mental illness or developmental disability, the multidisciplinary court team has allowed juveniles without a formal diagnosis to participate in the LAJMHC because of the belief that they may benefit from court-offered services. Often, the child is deemed IST by the court of origin by virtue of being exceptionally young (i.e., for reasons of developmental immaturity) and possessing subthreshold emotional or behavioral problems. Conversely, juveniles with mental illness who are explicitly not amenable to participate in potential treatment recommendations made by LAJMHC are excluded from participation.
The process by which a juvenile may be referred to, deemed eligible for, and participate in LAJMHC is further delineated in Figure 1.
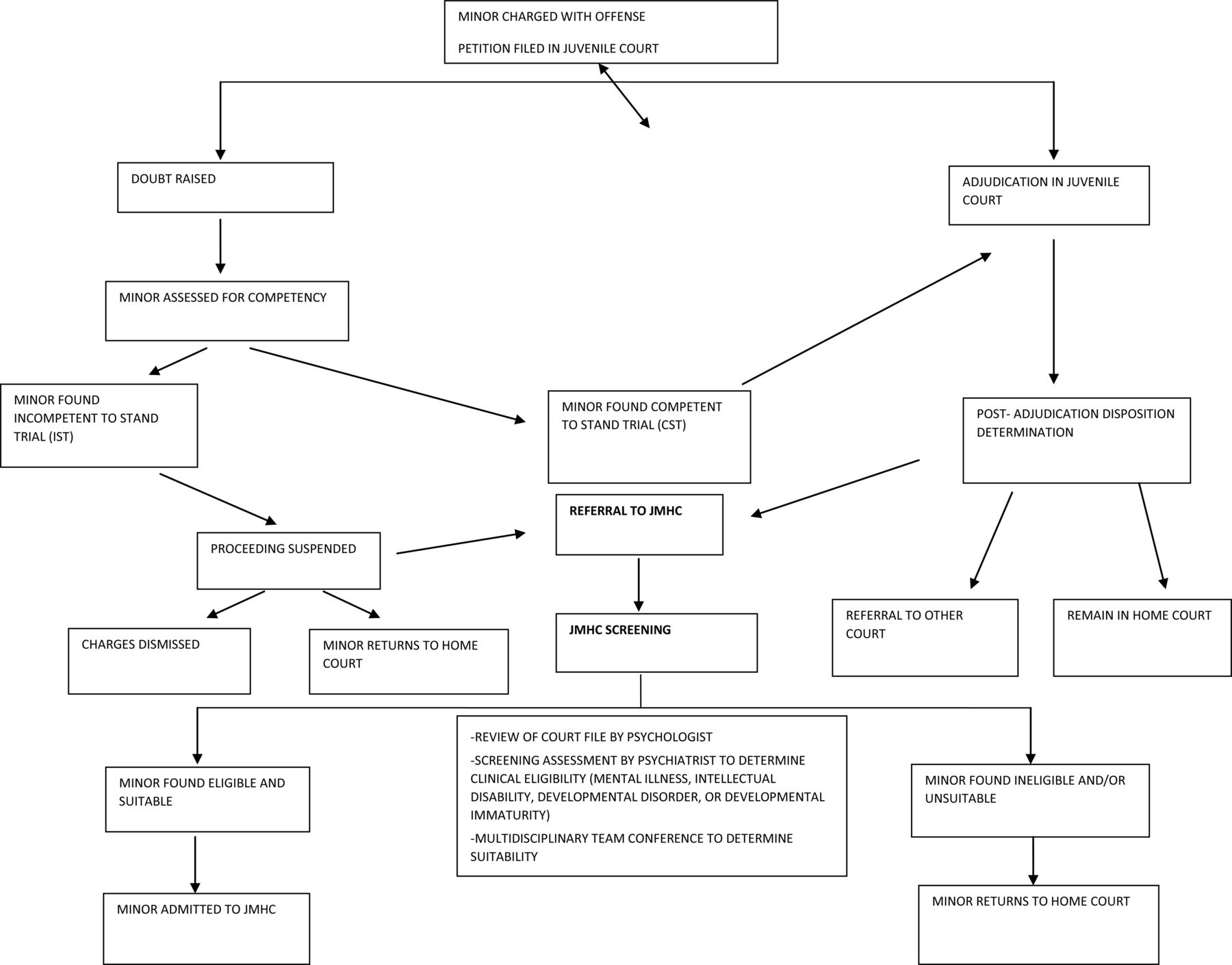
Process by which a youth is found eligible for the LAJMHC.
Inclusion criteria for our study mirrored those used to determine eligibility for participation by the LAJMHC court: the presence of a diagnosis of a mental illness or developmental disability and the youth's willingness to participate in treatment and other educational services recommended by the court's multidisciplinary team. Although the LAJMHC does not have formal bright-line, exclusionary criteria, as noted above, because the multidisciplinary team has some discretionary leeway in determining eligibility, exceptions were made to inclusion criteria when including youths in our study. Accordingly, the study sample included six participants who did not meet criteria for a mental disorder or developmental disability.
In the current study, the primary source of information was archival data collected from each youth's court and clinical records, obtained by the LAJMHC when the youths were referred for intake. For every minor referred to the LAJMHC, the consulting psychologist reviews the legal file and health and school records and prepares a brief data summary report. CST status, legal charges, and demographic data, including age, racial and ethnic identity, and gender, were obtained from these data summaries. In addition, supplemental data were gathered from Probation Officer Investigation Reports. Data regarding the minor's mental health diagnoses, associated treatment, and social history were also extracted from the aforementioned sources. As noted above, CST status was predetermined by the court of origin before referral to the LAJMHC, and minors had to be in the postadjudication phase of their case to be referred, unless they were designated IST and proceedings were suspended.
Each of the aforementioned variables was documented on a data collection form that was then used for data entry. To ensure the accuracy of the data entered, double data entry was performed for a randomly selected group of 20 participants across all variables. Entries were then reviewed by two of the coauthors, who also completed a file review on each participant. Data entry was found to be consistent between analysts.
Statistical Analysis
The goals of this study were to describe the distribution of demographic characteristics, the prevalence of diagnoses of mental illness and treatment history, and the relationships between these variables and CST status. Quantitative and qualitative descriptive statistics were used. Missing data or impossible values were examined by performing range and value checks. Central locations (mean, median, and quartiles) and dispersion were calculated for continuous measures, and frequency and mode were obtained for categorical measures. We compared sociodemographic characteristics across CST status and conducted bivariate analyses between CST status and predictors, using chi-square, Fisher's exact, or two-group t tests. Mantel-Haenszel chi-square tests were used for comparison of ordered variables (e.g., CST status versus age groups). We also conducted stratified (e.g., by age) bivariate analysis between CST status and predictor variables. The Cochran-Mantel-Haenszel test18 was used to determine whether the factors found to be associated with CST status remained significant after controlling for confounding factors (e.g., age group and intellectual disability). To assess for bias, the Breslow-Day test was used to examine the homogeneity of odds ratios.
We examined percentage distributions for CST and all other outcome variables by age and racial/ethnic identity. To ensure a sufficiently large sample size across racial/ethnic identity variable categories, the few participants who identified as American Indian/native Alaskan (AI/NA), native Hawaiian/Pacific islander (NH/PI), and Asian were combined into one category: other. The racial distribution of the study sample was consistent with recent reports from Los Angeles County, where it is estimated that racial minorities are disproportionately represented in the juvenile justice system: 61 percent Latino and 27 percent African-American.19
To address potential sample bias, we examined differences between study participants (i.e., 324 youths referred and selected) and nonparticipants (i. e., 98 youths referred but ineligible) on key variables. Of note, we found significant differences in CST status between participants and nonparticipants, with nonparticipants being more likely to be found CST than participants (59% and 46%, respectively; p = .025). No significant difference in age, gender, and racial/ethnic identity emerged between participants and nonparticipants.
Results
Of the 324 juveniles participating in the LAJMHC, 54 percent had been found IST by their court of origin, whereas 46 percent had been found CST. The average age of the sample was 16.0 years (SD 2.59), and 85 percent of the youths were aged 14 years and older. The mean age was similar across male and female participants: 16.0 (SD 2.6) and 15.9 (SD 2.4) years, respectively (p = .89). Of youths who were found IST, 61 percent were of Hispanic/Latino descent, 31 percent were of African-American descent, 4 percent were white non-Hispanic/Latino, and 4 percent were other (p = .09) (Table 1).
Age and Demographic Characteristics by Competency Status
Males and females significantly differed in competency status (p = .002), with 42 percent of males and 64 percent of females found CST. This finding was not significant after adjustment for age, but remained significant after adjustment for racial/ethnic identity (p = .005). Specifically, among juveniles of Hispanic/Latino descent, the females were significantly more likely to have been found CST than were the males (χ21 = 5.38, p = .02). Of the 28 Hispanic females in the sample, 61 percent were found CST, whereas, of the 146 Hispanic male participants, 37 percent were found CST. However, within other identified cultural groups, no significant differences in CST status emerged by gender.
Competency Status and Age
CST status significantly differed by mean age. The mean age of participants who had been found IST was 15.6 years and of those found CST, 16.5 years (F(1,322) = 10.5; p = .0013). CST status also differed significantly across all age groups (χ21,4 = 12.4; p = .014). Whereas the youths aged 14 to 15 years and younger were more likely to have been found IST than CST, participants aged 16 and older were more likely to have been found CST. No significant differences in CST status emerged between the 16- to 17- and 18-year-old and older age groups (p = .64). Despite the findings that youths aged 16 years or older were more likely to be CST than those aged 15 years and younger, in the 16 to 17 and the 18 and older groups, significance within group differences did not emerge (Table 1).
Competency Status and Mental Illness
Among the variety of psychiatric and developmental disorders in the sample, mood disorders (52%), intellectual disability (38%), attention deficit hyperactivity disorder (32%), and psychotic disorders (28%) were the most frequently occurring (Table 2). Juveniles with a diagnosis of intellectual disability (p < .0001) or a pervasive developmental disorder (PDD) were more likely to be found IST than those without diagnoses of these disorders (p = .02). Conversely, those with a diagnosis of a substance use disorder (p = .02), mood disorder (p < .0001), or psychotic disorder (p < .0001) were more likely to be found CST. In Table 2, the Breslow-Day test for homogeneity of the odds ratios is significant (p = .03) for adjustment of disorder, but nonsignificant for all other variables. For intellectual disability, the Breslow-Day test statistic is only .52; therefore, we have a common relative risk of 7.35 (95% CI = 4.28–12.6). The odds of being IST is 7.35 times higher for those who were in the intellectual deficiency group than for those who were not.
Psychiatric Diagnosis by Competency Status
Highly characteristic of justice-involved youth, 55 percent of participants had co-occurring disorders, whereas 43 percent were diagnosed with one disorder, and 2 percent had no mental health diagnosis. Of note, all youths without a mental health diagnosis were 15 years of age or younger and had been found IST by the court. Across age groups (<11; 11–13; 14–15; 16–17; and ≥18), the youths who had more than one disorder amounted to 27, 58, 66, 54, and 48 percent of the total, respectively.
Competency Status, Age, and Mental Illnesses
Juveniles with a diagnosis of a mood, substance abuse, or psychotic disorder were more likely to have been found CST than those without diagnoses of these disorders (p < .0001; p = .02; p < .0001, respectively). However, there was not a statistically significant difference in the odds ratios across age groups (Breslow-Day, p = .21,.33; and .64, respectively). The relationship between CST status and mood disorders was significant for each age group (p < .0001). However, for substance use disorders and psychotic disorders, the relationship between CST status and disorder type remained significant only for those in the 16- to 17-year age group (p = .035, and p = .0064, respectively).
Competency Status, Age, Intellectual Disability, and Pervasive Developmental Disorders
The significant association between CST status and age remained after adjustment for an intellectual disability diagnosis (p = .0027). However, there was no significant difference in the ORs across age groups (Breslow-Day p = .52). Juveniles with a diagnosis of intellectual disability were more likely to have been found IST than those without such a diagnosis (p < .0001), and this association remained statistically significant after adjustment for age (p < .0001). Juveniles with an intellectual disability diagnosis in the 11- to 13-year (p = .014), 14- to 15-year (p = .001), 16- to 17-year (p < .0001), and 18-year and older (p < .0001) age groups were each significantly more likely to have been found IST than their peers who did not have this diagnosis.
Similarly, a significant association between CST status and age remained after adjustment for a PDD diagnosis (p = .029), and no significant age differences emerged in examining the ORs across age groups (Breslow-Day p = .27). Juveniles with a diagnosis of PDD were more likely to have been found IST than those without a diagnosis of this disorder (p = .018), and this association remained statistically significant after adjustment for age (p = .022).
Competency Status and Mental Health Treatment History
Sixty-six percent of LAJMHC youths had a lifetime history of receiving some form of mental health treatment. Twenty percent of the sample had been prescribed psychiatric medication in the past, whereas 37 percent had a lifetime history of receiving psychotherapy. In addition, 54 percent of juveniles were receiving psychiatric medications at the time of their initial evaluation for entry into LAJMHC (Table 3.) There was a significant difference in CST status based on any history of mental health treatment. Of those who had received any type of treatment, 55 percent were found CST, whereas 30 percent of those who never received treatment were found CST (p < .0001).
Mental Health Treatment and Competency Status
Discussion
Overall, demographic characteristics of juveniles participating in the LAJMHC were consistent with youths involved in the juvenile justice system in Los Angeles County: young males of predominantly Hispanic/Latino or African-American descent born in the United States.20 No significant differences in CST status emerged by racial/ethnic identity; however, males were more likely to be found IST than females. Although this finding cannot be explained by age (e.g., participants were very similar in age across gender), the relationship between CST status and gender was significant with adjustment for racial/ethnic identity. Specifically, females who identified as Hispanic/Latina were more likely to be found CST than were males with a similar cultural identity. As myriad social, psychological, or linguistic factors could explain this relationship, future studies will use a multivariate model to consider this association relative to available measured variables.
Of note, in preliminary analyses, significant differences in competency status also emerged between juveniles accepted to participate in the LAJMHC versus those deemed ineligible to participate, with nonparticipants significantly more likely to be found CST. It is possible that this difference occurs because the criteria determining court participation generally require diagnosis of a mental health or developmental disorder, as well as amenability to treatment services recommended by the court. Accordingly, youths who had been found CST and referred by their court of origin to the LAJMHC because of the possible presence of a mental condition may have had less severe impairments than their counterparts who were found IST. In addition, these youths may be less interested or agreeable to receiving services offered by the court, possibly because they had less severe impairments. Moreover, differences between participants and nonparticipants may be affected by factors including the legal charge or the scope of services offered by LAJMHC. Future analyses are warranted for further examination of variables that influence LAJMHC participation and inclusion, as well as the process by which juveniles are referred to LAJHMC. Further study may be particularly important in increasing understanding and in developing effective approaches to identifying justice-involved youths in need of mental health services and in tailoring available services and incentives for participation.
Consistent with previous studies occurring in juvenile justice settings, we found that younger age was highly associated with a legal designation of IST for those participating in the juvenile mental health court. Similarly, our findings suggested a step-wise relationship between CST status and age, consistent with previous findings that juveniles aged 16 to 17 do not differ significantly from adults in CST status.5 Accordingly, developmental immaturity should be regarded as a salient factor that may affect the likelihood of an IST finding in juvenile mental health courts. However, we found that, even among juveniles aged 16 years and older, approximately half were designated IST. Although normative developmental maturity may continue to be relevant in this older population, the rate of IST findings may also be related to the fact that by virtue of LAJMHC participation, these youths were likely to have received a diagnosis of at least one major Axis I psychiatric or developmental disorder that could affect their adjudicative competency capabilities.
As might be expected, the presence of developmental disorders conferred additional vulnerability to deficits in adjudicative competence. Also as anticipated, juveniles with intellectual disability or PDD were more likely to be designated IST than those without these disorders, further underscoring the importance of intelligence and level of adaptive and cognitive functioning in determination of adjudicative competence abilities. The current study also found that a positive association between IST status and intellectual disability and between IST and PDD, remained statistically significant after adjustment for age. Results of the Breslow-Day test confirmed that these disorders and CST status were similar across age groups, suggesting an absence of bias owing to age. Further, juveniles in each age group with a diagnosis of intellectual disability were more likely to have been found IST than their same-age peers. This finding suggests that, regardless of age, an intellectual disability may play a significant role in impairing the abilities requisite for participating in legal proceedings. Of note, the sample size of those diagnosed with a PDD (n = 20) was too small to analyze CST differences within age groups with statistically meaningful results.
In another unexpected finding, juveniles with diagnosis of a mood, substance use, or psychotic disorder were more likely to have been found CST than those without these disorders. Further, after adjustment for age, the relationship between each of these disorders and CST status remained significant, and Breslow-Day test results confirmed that these disorders and CST status were similar across age groups, suggesting an absence of age bias. However, when looking more specifically at within-group differences by age, although youths with mood disorders in all age groups were more likely to have been found CST than their same-age-group peers without the disorder, the relationship between CST status and a diagnosis of a substance use or psychotic disorder remained significant only among 16- and 17-year-old participants.
Overall, these findings suggest that regardless of age, simply having one of these disorders is not enough to impair juveniles' abilities relative to CST. In fact, the likelihood of being found competent was significantly greater for those with a diagnosis of a mood disorder, regardless of age, and with a substance use or psychotic disorder, if aged 16 or 17 years. However, this result seems counterintuitive, particularly in the case of psychotic disorders, which commonly impair thought processes and behavior. One explanation could be that, given heterogeneity in type, pattern, and severity of symptoms within a specific diagnosis, these more nuanced factors may be stronger predictors of competency status than a singular diagnostic label of psychotic or substance abuse disorder. For example, one juvenile with a psychotic disorder may hold the delusional belief that there is a judicial conspiracy against him, leading to an IST designation, whereas another youth's delusional thought content could be unrelated to legal proceedings and lead to a CST finding. It should also be considered that, given the age range of our sample, many of the juveniles diagnosed with psychotic disorders may be in the prodromal phase of their illness and may have symptoms that are less severe or less likely to impair competency abilities than a more fully developed or persistent psychosis. However, the current study is limited, in that data regarding participants' severity of illness or specific symptoms were not available, although future data collection procedures are likely to allow this hypothesis to be tested going forward.
Consistent with the mental illness in general, most of our sample endorsed comorbid psychiatric disorders. Further, juveniles in our sample with more than one diagnosis were more likely to have been found IST than those with a single diagnosis. However, further analyses must be completed that examine the role of comorbidity patterns, to improve understanding of how specific clusters of disorders impact CST status in this population. This approach may also aid in further explaining the seemingly counterintuitive relationship between mood, substance use, and psychotic disorders and CST status.
In contrast to prior studies demonstrating an association between mental health treatment and juvenile-justice–involved youth with IST status,6,7 we found that participants in LAJHMC with a history of any type of treatment (psychotherapy, medication management, or both) were significantly more likely to be found CST than those without any treatment history. It is possible that current or past mental health treatment conferred some protection against impairment of adjudicative competency capacities. In addition, there may be other factors related to mental health service utilization that may increase the likelihood that specialty-court–involved youths will be found CST. Further analyses will more specifically address the impact of certain classes of psychotropic medications on CST status relative to mental illness designation. Moreover, future analyses will investigate differentiation between those whose developmental immaturity may have been the primary factor impairing CST status, rather than mental health symptoms. For the former group, psychiatric treatment would not be as salient in attaining competency as would simply getting older.
Implications
More than half of juveniles accepted to participate in the LAJMHC lacked the requisite competence to participate in the adjudicative process. IST youths are mostly likely to be the youngest and the most cognitively and developmentally impaired in the legal system. Over 40 percent of youths admitted to the LAJMHC had not received mental health services before entering the juvenile justice system. The LAJMHC and mental health courts in general may therefore be an important interface and entry point for referral and linkage to mental health services. More broadly, the juvenile court system, the primary referral source for LAJMHC, has increasingly identified youths in need of treatment or supportive services through the somewhat indirect mechanism of the questioning of competency by the court or attorney. Although not necessarily intended for this purpose, competency evaluations have accordingly become a unique pathway by which youths may be assessed and recommended for services, such as those offered by specialty courts in the few jurisdictions where they exist. Determining the correlates of incompetency may help identify those who could benefit from competency training, so that they can proceed with their legal cases, and it may facilitate the identification of services that would be of benefit to the youths (such as mental health services and educational and learning rehabilitative resources). Once a juvenile has been found IST, in many jurisdictions, legal proceedings are suspended. This interruption poses a difficult dilemma for the court system, as suspension of legal proceedings means that the court has limited legal power to mandate that a rehabilitative treatment plan be in place, but at the same time must balance the need for public safety.21
Limitations
There are multiple limitations to this study that may inform future research and approaches in collaborating with juvenile court systems to develop better understanding of challenges faced by young offenders. This study was a retrospective chart review, and the data were obtained from multiple sources. Although mental health, treatment, and social variables were culled from brief summary reports completed by the court psychologist, not all juveniles had the same data available at intake. Our sample was heterogeneous, and we were limited to data that were available in the court files, both in quantity and substance. In addition, there was variability in the types of measures used to assess CST and psychiatric diagnosis. Furthermore, in the case of mental health data from a real-world setting, the use of standardized assessment tools to aid in diagnosis is the exception rather than the rule. Moreover, only juveniles who have been court ordered to undergo a mental health assessment (e.g., to assess CST, overall mental health and treatment recommendations) would have access to this rigorous approach. Based on the inability to perform direct evaluations of the juveniles in the sample for the purpose of this study, we were not able to verify the quality or accuracy of the clinical data through independent interviews. Although it is thought that the strength of the data derived from these varied evaluation approaches were sufficiently robust to substantiate current findings, future studies may benefit from analyses with exclusion criteria based on the comprehensiveness of evaluation methodology.
Finally, generalizability of findings may be limited by factors that could appreciably differentiate the juvenile mental health court population from youths with mental or developmental disorders who either have not been referred to or are not eligible for participation in mental health court or who live in jurisdictions that lack specialty courts. The present sample includes only juveniles who have been referred and accepted to participate in the LAJMHC, with inclusion criteria primarily defined by diagnosis of a major mental disorder and a youth's amenability to treatment recommendations. However, given the multidisciplinary specialty court context in which this decision is made, the LAJMHC team has the ability to include or exclude participants for additional reasons, such as developmental immaturity and related impairments that may be aided by court-based treatment services. Moreover, based on this discretion and the voluntary nature of the court, individuals who otherwise meet criteria but also express amenability to treatment may be more likely to be included for participation than those who do not express interest in treatment. Nonetheless, it should be noted that comparisons between study participants and individuals who are referred to LAJHMC but rejected did not suggest significant differences between participants and nonparticipants on key demographic variables, suggestive of some level of generalizability based on age, race, and gender. However, juveniles who participated in the court were more likely to have been found IST than those who were referred and not accepted for participation, which may decrease generalizability to some degree.
Comparing the current sample to one containing adjudicated juveniles with mental illnesses who were not referred to LAJMHC was outside the scope of this study. However, based on the nature of the legal system, mentally ill youths charged with highly violent crimes or for whom prosecution in nonspecialty courts is otherwise strongly pursued, may be less likely to be referred to LAJMHC, and accordingly, may differ on other characteristics from the present sample. Accordingly, the present study's inability to compare specialty-court–involved youths to a traditional juvenile justice population on various factors may be seen as a limitation in terms of generalizability. Nonetheless, given that the severity of the crime is not an explicit exclusionary criterion for LAJMHC, and many juvenile participants have been charged with violent crimes, this point may be less salient in limiting generalizability to non–mental-health court youths charged with serious offenses. Future analyses will further explore the relationship between offense type and competency, as well as the characteristics of those rejected from participation in the LAJMHC. Finally, this finding highlights how little is currently known about factors that may affect a legal professional's decision to refer a youth to specialty court. Future studies are needed to assess the various factors that may influence or deter the referral of youths involved in juvenile court proceedings to specialty court settings.
Future Considerations
To our knowledge, this study marks the first attempt to examine factors associated with competency status in a juvenile mental health court. Further analysis is needed to explore the possible interplay of comorbid psychiatric and developmental conditions, as well as the impact of specific types of treatment received, including psychotropic medications, on CST status. Moreover, further investigation regarding the relationship between CST status, diagnosis, and other psychosocial factors by gender will provide additional insight into potential reasons for our finding that females were more likely to be found CST than were males. In addition, data are limited on the longitudinal clinical and judicial outcomes of youths who are referred for CST evaluations, let alone the impact of services provided in juvenile mental health courts on these outcomes. Although the LAJMHC does not currently provide competency-attainment services for youths found IST who enter the court, further investigation of specific court-recommended interventions and improvements in functional abilities akin to those associated with adjudicative competence (e.g., communication or reasoning abilities and behavior regulation) may have bearing on the development of tailored approaches to restoration programming in juvenile courtroom settings in which restoration is the primary dispositional objective. Finally, consistent with the rehabilitation goal of juvenile mental health courts, identifying correlates of competency in youths is an important means of improving assessment and determining the types of mental health, educational, and supportive services imperative to increase the likelihood of the future health and prosocial trajectory of this highly vulnerable group of youths.
Acknowledgments
The authors thank the following mentors, colleagues and Los Angeles County community partners for their input, support, and guidance: The Los Angeles County Juvenile Mental Health Court Team, David Farabee, PhD, Gail Wyatt, PhD, Norweeta Milburn, PhD, Gerhard Hellemann, PhD, the Honorable. Judge Christina Hill, Commissioner Robert Leventer and the Hon. Presiding Judge Michael Nash.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2015 American Academy of Psychiatry and the Law





{kind=link}