


Abstract
This study examined the effect of clozapine on time assigned to restrictive housing (RH; i.e., solitary confinement), disciplinary infractions, and assaults on custody staff among patients treated within the North Carolina prison system. Records were reviewed for patients initiated on clozapine (n = 84) over a 3.5-year period. Fifty-nine patients completed at least three consecutive months of treatment and were included in data analysis. Assigned RH days and disciplinary infractions were assessed for the periods prior to and after treatment with clozapine. Patients accumulated 13,500 RH days pretreatment and 3,560 days postclozapine initiation. There was a significant reduction in RH days with clozapine treatment (P < .05). Patients with personality disorders (n = 36) had a significant decrease in RH days (P < .05), while those with psychotic disorders (n = 23) showed a decrease with borderline significance (P = .051). There were 253 disciplinary infractions pretreatment, including 27 assaults on custody staff, and 118 infractions posttreatment, including 7 assaults; the decrease in infractions was significant in the first three months of treatment (P < .05). The mean ± SD duration of treatment was 269 ± 102 days. Expanding clozapine use in state prisons should be a high priority, as these data are consistent with reports of clozapine's benefits in community settings.
Clozapine is the only psychotropic medication in the United States with Food and Drug Administration (FDA) indications for treatment-resistant schizophrenia and reduction in suicide risk for patients with schizophrenia or schizoaffective disorder.1–2 Several studies have also shown potential benefits of clozapine in the management of self-injurious behavior and aggression toward others for both psychotic and nonpsychotic individuals.3,–,9 Clozapine's benefits appear independent of its antipsychotic efficacy or sedating properties.4,5
Despite these unique benefits, clozapine remains underused in the United States.10 In the community, statewide rates of clozapine use range from 1 to 8 percent of Medicaid beneficiaries with schizophrenia.11 In correctional settings, a recent survey showed that one-third of state prisons do not have clozapine on their formularies; those that do offer clozapine treat a median of eight individuals per state.12 This is occurring despite a U.S. state prison population of nearly 1.3 million people and an estimated prevalence of serious mental illness two to four times higher in prisons.13,14 Rates of self-injury and aggression toward others are also much higher among incarcerated individuals when compared with the general population.15,16 Patients with personality disorders in particular have a disproportionate share of self-injurious and aggressive episodes, often leading to use of multiple psychotropic medications and restrictive interventions. Traditional therapeutic management of violence for individuals with mental illness (including personality disorders) includes behavior plans, contingency management, cognitive-behavioral therapy, and various pharmacologic agents including, but not limited to, antipsychotics, antidepressants, and mood stabilizers. There are limited data supporting the effectiveness of any of these methods.
While repetitive self-injury and violence toward others may have similar underlying biological mechanisms related to impulsivity and emotion dysregulation,17 the consequences in corrections are very different from those in mental health settings. The use of restrictive housing (RH), also known as solitary confinement, is often employed as a consequence for general rule breaking in correctional settings, especially for aggressive behaviors. RH involves confinement to one's cell for up to 23 hours a day, with one hour out of the cell for solitary exercise or hygiene. RH has been associated with increased psychological distress, paranoia, self-injurious behavior, aggression, and an increased risk of death upon community reentry.18,–,21 A search of PubMed/MEDLINE using the search terms (“restrictive housing” OR “solitary confinement” OR segregation) AND (psychotropic OR medication) revealed no current studies on the effect of any psychotropic medication on time assigned to RH related to infractions incurred (i.e., disciplinary segregation).
Data regarding clozapine's effectiveness in managing violence in a prison setting are limited. A case series on seven patients with a history of violence and antisocial personality disorder treated with clozapine reported reduced overall aggression and improvements in Clinical Global Impression scales22; however, only one patient had an episode of physical aggression while hospitalized before clozapine treatment. We previously reported on eight patients with a primary diagnosis of a severe personality disorder in the North Carolina prison system treated with clozapine, and we noted marked reductions in self-injurious behavior, infractions, and assaults on custody staff.7 This study aims to expand on those preliminary data and analyze changes in time assigned to disciplinary segregation, overall infractions, and assaults against custody staff among all patients treated with clozapine for at least three consecutive months over a 3.5-year period within the North Carolina prison system.
Methods
Patient Population
Electronic health records were reviewed for all patients prescribed at least one dose of clozapine between July 1, 2016, and December 31, 2019, within the North Carolina prison system. Patients initiated prior to July 1, 2016, or who entered the prison already taking clozapine were excluded. Only patients who completed at least three consecutive months of treatment were included for analysis; this criterion was used to ensure an adequate trial for the outcomes measured, taking into account the slow titration occurring in the first month. Eight patients who were included in a previously analyzed data set related to self-injury and infractions were included only for analysis of time assigned to RH.7
Eighty-four patients were started on clozapine during the study period. Fifty-nine patients completed three consecutive months of treatment and were included in the analysis. Background information collected included demographics; primary psychiatric diagnosis as determined by consensus agreement of two of the authors, TRZ and BBS; history of intentional self-injury or suicide attempt; presence of intellectual disability, seizure disorder, or substance use disorder; gang affiliation; crime of conviction; and previous antipsychotic and mood stabilizer trials while in prison. Prior medication trials in the community were not counted due to lack of consistently available records. Patients with schizophrenia, schizoaffective disorder, or bipolar disorder type I with psychotic features were collectively grouped as “psychotic disorder,” while those with borderline personality disorder or antisocial personality disorder were grouped as “personality disorder.” Patients with both a psychotic disorder and a personality disorder were included in the psychotic disorder group. Descriptive statistics were used to compute proportions for categorical variables, and differences between included and excluded patients were assessed using Fisher's exact test. The level of significance was set at .05.
Clozapine treatment was characterized by initiation date, duration of therapy, and maximum dose achieved. The posttreatment period began with the first 12.5-mg dose administered. Adherence was calculated using the total doses administered divided by total prescribed doses. Absolute neutrophil counts were reviewed at initiation and upon any termination of treatment due to neutropenia. Other clinically significant side effects were measured by initiation of medications to target them (e.g., atropine ophthalmic drops for sialorrhea, or laxatives or stool softeners for constipation) or a need to terminate treatment (e.g., myocarditis, ileus, etc.). Weight was documented at the time of initiation and at every three months as available for the first year. Interruptions in treatment were defined as missing more than three consecutive days of therapy, which would in most cases necessitate re-initiation of the medication.
The primary outcome was time assigned to RH, measured in days, as a consequence of infractions incurred (i.e., disciplinary segregation). Secondary outcomes included counts of all disciplinary infractions and assaults against custody staff. Only disciplinary infractions with a guilty verdict, as adjudicated by the prison's disciplinary hearing board, were included in the analysis. Assaults against other incarcerated individuals were not included in the analysis because these do not always result in disciplinary infractions and appear to be less reliably recorded. No additional data were collected outside what was available in clinical and administrative records.
The duration of clozapine treatment varied (either because treatment was discontinued by the patient or prescriber, or because some patients started treatment late in the study period and reached the end of the data collection window), and patients were grouped by three-month quarters of completed treatment for analysis. Therefore, we had patients who had completed 3, 6, 9, or 12 months of clozapine treatment.
For all pre/post analyses, we sought to compare the within-subject number of events occurring during the completed quarter(s) of continuous clozapine treatment with the number occurring during the same length of time prior to clozapine initiation. For our primary analysis, we examined pre/post changes in the number of assigned RH days among those who had completed 3 months of clozapine with assigned RH days in the three months preceding clozapine initiation. We then repeated this analysis separately for those with personality disorders and those with psychotic disorders. Additionally, we assessed for differences in assigned RH days for each of the following pre/post clozapine treatment periods: 0 to 3, 3 to 6, 6 to 9, and 9 to 12 months.
The distributions of the within-subject difference between pre and postclozapine assigned RH days were not normally distributed on the basis of the Shapiro-Wilk normality test. Furthermore, nearly half of patients experienced zero assigned RH days and infractions in the 3 months before and after clozapine initiation, limiting meaningful comparisons of the median value for pre and post events (because both pre and post median values were zero). Accordingly, we reported results by creating box and whisker plots of the distribution of the difference between assigned RH days before and after clozapine treatment, and we tested for pre/post differences using the nonparametric Wilcoxon signed-rank test using a two-sided alpha of 0.05. The Wilcoxon signed-rank test is analogous to a paired t test but is used for data with nonnormal distributions.
Study Site
The North Carolina Department of Public Safety (NC DPS) housed approximately 35,000 individuals in 55 correctional institutions throughout the state during the study period. NC DPS offers a continuum of mental health services including inpatient, residential, and outpatient levels of care. Approximately 18 percent of incarcerated individuals in NC DPS custody were receiving some form of mental health services during the study period. The majority of individuals in this study were initiated on clozapine while receiving inpatient care at the Central Prison inpatient mental health unit. The clozapine protocol, therapy services, and unit are described elsewhere.7 Clinical pharmacists worked closely with providers to assist with lab monitoring and entering data into the Clozapine Risk Evaluation and Mitigation Strategy Program website. Patients on the inpatient unit were offered cognitive-behavioral therapy groups during their admission, even while in restrictive housing. Other mood stabilizers and antipsychotics were tapered and discontinued when clozapine was started, unless the mood stabilizer was being used to treat a seizure disorder. If carbamazepine was used for this indication, it was changed to levetiracetam to avoid drug-drug interactions with clozapine. Antidepressants were permitted while on clozapine. Two of the authors (TRZ and BBS) provided training to nursing staff and were available on a consultative basis to all providers in the NC DPS system to address clozapine-related questions or concerns. In addition, faculty from the Department of Psychiatry at the University of North Carolina School of Medicine were available to provide direct psychiatric services at Central Prison to help with clozapine initiation as part of a prison-academic partnership that began in 2014.
This study was approved by the Office of Human Research Ethics at the University of North Carolina at Chapel Hill (IRB #18-2968).
Results
Eighty-four patients were initiated on clozapine during the study period, and 59 patients met inclusion criteria. Demographic and clinical characteristics of the included and excluded cohorts are presented in Table 1. The groups were statistically similar for all variables except for a higher proportion of individuals with a history of self-injury or suicide attempt in the included cohort (P = .008). Of the 59 patients included for analysis, 36 had a primary diagnosis of personality disorder (borderline or antisocial) and 23 had a primary diagnosis of a psychotic disorder. Sixteen of the 23 patients with a psychotic disorder also had a diagnosis of personality disorder. Fifty-seven patients had a comorbid substance use disorder. Sixteen patients had a conviction of murder or manslaughter, while 19 had an active gang affiliation.
Demographic and Clinical Characteristics of Patients Receiving Clozapine for ≥ 3 Months or < 3 Months
Twenty-four patients had completed 12 months of treatment at the time data collection ceased. The remainder (n = 35) received less than 12 months of treatment, because of patient preference (n = 5), side effects (n = 10), or release from prison (n = 9), or were continuing treatment but reached the end of the study period (n = 11). In sum, all 59 patients took clozapine for at least three months but less than six months (3 months of data analyzed); 44 completed at least 6 to 8 months (6 months of data analyzed), and 33 took it for at least 9 to 11 months (9 months of data analyzed). In total, there were 474 patient-months of treatment. Previous medication trials for these patients included an average of 3.8 ± 2.0 antipsychotics and 1.8 ± 1.1 mood stabilizers in the prison system prior to clozapine initiation.
Among the 59 patients, 29 (49%) had no assigned RH days in the three months prior to or following initiation of clozapine; 23 (39%) patients had a reduction in assigned RH days following clozapine initiation, and 6 (10%) had an increase; one was assigned RH days in both periods but had no change. The sum of assigned RH days for all patients was 13,500 days pretreatment and 3,560 days postclozapine initiation. There was a statistically significant reduction in posttreatment RH days for each quarter analyzed (0 to 3, 3 to 6, 6 to 9, and 9 to 12 months) (Fig. 1 and Table 2). Patients with personality disorders (n = 36) had a statistically significant reduction in RH days (P < .05) in the three months following clozapine initiation compared with the prior three months; those with psychotic disorders also had a reduction in assigned RH days in the three months following clozapine, but this reduction had borderline statistical significance (P = .051). The distribution of assigned RH time by quarter among patients taking clozapine for 12 months is presented in Fig. 2. Infractions were analyzed for 51 patients after removing 8 patients who were previously reported on. Twenty-four (47%) had no infractions in the three months before and after starting clozapine; seven (14%) patients had an increase in infractions, while 17 (33%) had a decrease; three (6%) had the same number of infractions in both periods. Infractions were reduced from a total of 93 in the three months before treatment to a total of 41 while on clozapine; the within-person reduction in infractions was statistically significant (P < .05). Assaults against custody staff decreased in the first three months from a total of 12 pretreatment to a total of three while on clozapine, although the within-person reduction of assaults did not reach statistical significance (P = .125).
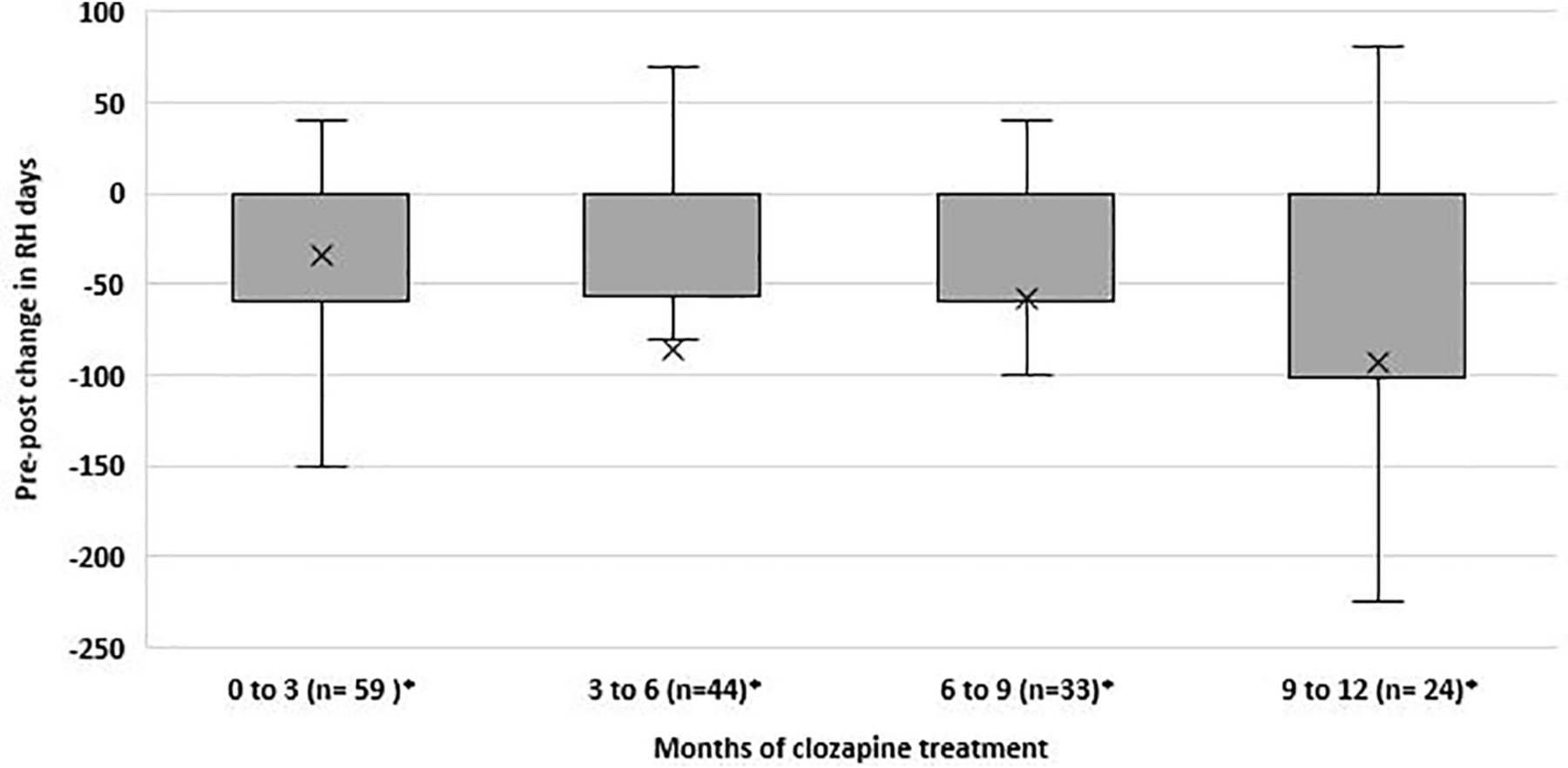
Distributions of the difference in assigned restrictive housing (RH) days among patients before (pre) and after (post) clozapine treatment for 0–3, 3–6, 6–9, and 9–12 months. The X indicates the mean reduction; the shaded area represents the interquartile range, and whiskers represent minimum and maximum values excluding outliers (i.e., values > 1.5 times the interquartile range below the 25th percentile or above the 75th percentile; outliers not shown). Median values are typically represented by a horizontal line within the interquartile range, but in these plots, the median overlaps with the 75th percentile line (i.e., has a value of zero).*The test to detect a pre-/post difference was statistically significant using the Wilcoxon-Signed Rank Test (P < 0.05).
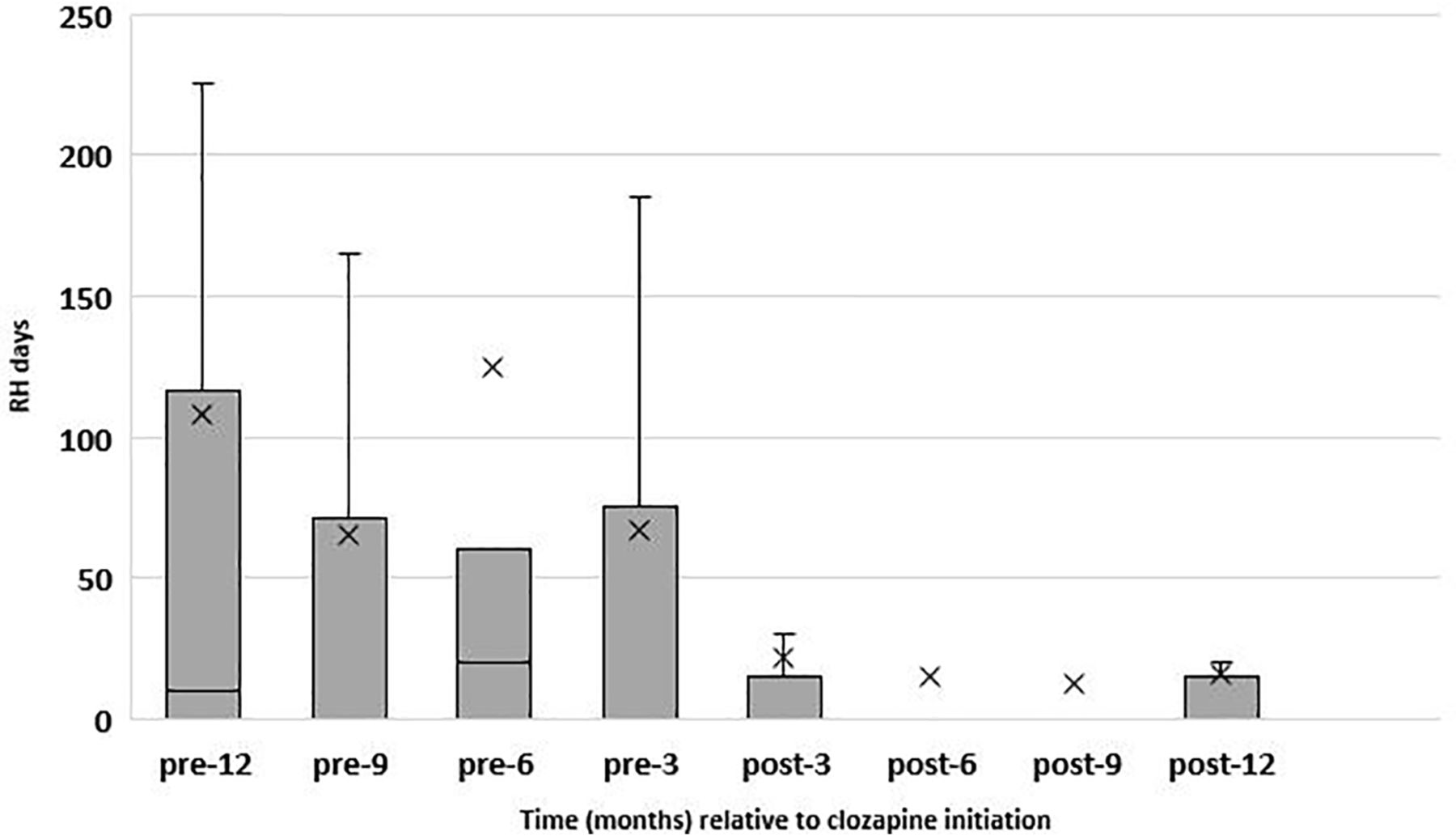
Distribution of quarterly assigned restrictive housing (RH) days among patients during 12 months of continuous clozapine treatment The X indicates the mean reduction; the shaded area represents the interquartile range, and whiskers represent minimum and maximum values excluding outliers (i.e., values > 1.5 times the interquartile range below the 25th percentile or above the 75th percentile; outliers not shown). Median values are typically represented by a horizontal line within the interquartile range, but in some instances the median overlaps with the 25th percentile line (i.e., has a value of zero).
Distribution of Assigned Restrictive Housing Days Pre- and Post- Clozapine Treatment
The average duration of clozapine treatment over the course of the year was 269 ± 102 days. The average maximum dose achieved was 186 ± 95 mg/day (range 50–450 mg/day). Patients with personality disorders and psychotic disorders took 164 ± 84.5 mg/day and 222 ± 101 mg/day on average, respectively. The overall medication adherence rate was 93 percent. Forty-four patients experienced side effects requiring the initiation of another medication for symptomatic management: 28 patients experienced constipation, 24 reported sialorrhea, and four had tachycardia. Ten patients stopped treatment because of side effects, including one due to neutropenia. There were no discontinuations related to suspected myocarditis or other serious side effects. Thirty-one patients had a 7 percent or greater weight gain over the course of treatment. The average weight gain for all patients was 7.6 ± 8.0 kg, or 1.1 ± 1.1 kg/month of treatment.
Discussion
To our knowledge, this is the first study to assess the effect of clozapine on time assigned to restrictive housing. The patients included in this study demonstrated reductions in RH time totaling nearly 27 years when comparing the periods before and after starting clozapine for all months of treatment. All patients had been tried on multiple other antipsychotics and mood stabilizers, in addition to available psychotherapies. This effect was independent of diagnosis, with both the psychotic and nonpsychotic groups displaying relatively similar percent reductions, though only those with personality disorders reached statistical significance after three months. The borderline significance in the psychotic disorders group may be a function of the smaller sample size. It should also be noted that the postclozapine period began with the first dose of medication. The slow titration and onset of treatment effect (1 to 2 weeks later at the earliest) may have skewed results against clozapine during this period. The longitudinal results in the 12-month treatment group reflect clozapine's benefits in the first quarter of treatment, which also persist and increase over time. The observed decrease in RH time is conservative given that only disciplinary RH time was counted, not additional administrative time which custody may assign for the protection of others when disciplinary time expires. Though not statistically significant in the first quarter analyzed, there was a reduction in assaults against custody staff, consistent with previously published data.7 The average dose of 186 mg/day is less than what might be used to treat schizophrenia and mitigates the risk of serious side effects.
These data are consistent with prior studies demonstrating clozapine's reduction of aggressive behaviors in psychotic patients treated in community settings.4,–,6,23,–,25 Many of the patients in this cohort are characterized by severe emotion dysregulation, impulsivity, an inability to cope with stress, and prior history of trauma. These traits, when combined with the prison setting itself and subsequent placement in solitary confinement, can exacerbate chronic patterns of impulsive behaviors including violence and self-injury. While the antiaggressive effects of clozapine may be related to alleviation of psychotic symptoms in some patients, prior studies have shown these effects to be independent of antipsychotic efficacy.4,5 Furthermore, the majority of patients in this study did not have a psychotic illness.
Of particular interest, 57 of the 59 patients treated with clozapine had a comorbid substance use disorder. The high prevalence of substance use disorders in patients with personality disorders and psychotic disorders is well documented.26,–,28 Individuals with substance use disorders are thought to experience dysfunction of the dopamine-mediated mesocorticolimbic reward system, which has been implicated in the pathophysiology of addiction.29 They may then engage in the repetitive use of substances to modulate this disordered reward system.30 While individuals may obtain illicit substances while incarcerated, the patients in this study were not thought to be using routinely, though no regular testing was done for confirmation. Some studies have noted an interesting association between clozapine use and reduced relapse on substances and cravings for substances, including cigarette smoking.31,–,36 Investigations into clozapine's effect on the reward system have shown that clozapine plays a role in modulating the activity of dopaminergic neurons located in the ventral tegmental area.37 Furthermore, a normalization of neurotransmitter activity occurs in the prefrontal cortex in patients taking clozapine.25 Though speculative, these neurobiological effects may explain in part how clozapine confers benefits in the study population, while other psychotropics (including other antipsychotic medications) were not as effective.
Clozapine remains grossly underused in correctional settings despite its potential benefits. Common community barriers, which are also true of prison systems, include the need for mandatory blood monitoring, administrative burden, concern about serious side effects, and providers having little training or experience initiating clozapine. The initiation process is also much more complex than that of other antipsychotics, requiring more time and attention by the prescriber. Historically, clozapine prescribing has been left to psychiatrists, and many prison systems face shortages of psychiatrists or rely on part-time telehealth or other contract providers for services with little to no experience initiating clozapine.
Clozapine treatment offers the opportunity to meet medicine's quadruple aim: improved quality of care, patient satisfaction, staff satisfaction, and reduced costs.38 Multiple efforts have been made on a national level to educate community providers and administrators about clozapine, with no apparent substantial increase in prescribing over time. Expecting education alone to change prison prescribing patterns, with its many additional challenges, is likely unrealistic. A consultative system, similar to the Extension for Community Healthcare Outcomes (ECHO) model,39 offers one potential solution. By implementing a similar model in North Carolina, we were able to initiate an average of two new clozapine patients per month over a 3.5-year period. Alternatively, in correctional settings without psychiatrists available, off-site psychiatrists (such as those linked to academic medical centers) could serve as expert advisors, with prescribing handled by primary care providers and advanced practice providers with support from clinical pharmacists. In this manner, systems can leverage limited psychiatric resources to reach many more patients. Such changes could have profound implications nationally, as there are likely thousands of incarcerated individuals across the United States who could potentially benefit from clozapine therapy.
This study should be interpreted in the context of several limitations. Analyses conducted with the prison population are susceptible to the potential for secondary gains influencing the results. All patients signed a voluntary consent form agreeing to clozapine treatment. It is therefore possible that patients thought this would offer additional benefits beyond the opportunity to control their symptoms effectively. It is not uncommon for incarcerated individuals to feign symptoms or improvements in symptoms to obtain some perceived benefit. In addition, the abuse of prescribed medication in this group is very common, including medications that are typically not thought of as having abuse potential.40 In particular, any medication that is sedating or stimulating has high abuse potential in prison. Clozapine, with its sedating qualities, is therefore a candidate for misuse.
Furthermore, there was no control or comparison group, and because this was a retrospective chart review, there were no standardized assessments of symptom reduction, side effects (including sedation), or patient experience. Clozapine blood levels were not drawn routinely, but were drawn on the basis of providers' prescribing habits. The cohort of included patients had a higher baseline rate of self-harm, and regression to the mean could have influenced these results. As with our prior analysis, the treatment setting, including custody or housing status, was not standardized before or after clozapine initiation, and increased attention from providers may have influenced results early in the treatment course. The persistence of treatment effect over time in the 12-month cohort, however, argues against this being primarily a placebo effect. This study did not address the contributions of adjunctive psychotherapy. It was also not possible to assess aggression against peers due to the lack of available data.
Conclusions
Incarcerated individuals with severe psychiatric disorders pose special challenges to correctional systems. The use of restrictive housing or solitary confinement in managing patients with problematic behaviors often exacerbates psychological distress. To our knowledge, no prior studies have evaluated the use of psychotropic medication in reducing restrictive housing time. In this study, treatment with clozapine led to significant declines in disciplinary segregation time and infractions. Strikingly, this effect was not limited to individuals with psychotic disorders, as it was possibly more effective for individuals with severe personality disorders.
Despite the cautions outlined above, these data do offer the promise of reducing behaviors that result in many patients with a severe mental illness being placed in solitary confinement for extended periods of time. Future research should attempt to replicate these findings in other correctional settings.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2021 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}