


Abstract
The rate of civil commitment in Oregon fell from 53.2/100,000 in 1972 to 9.2/100,000 in 2020. The paper discusses this decline in civil commitment as related to statutory and case law changes and complex interactions including bed availability at Oregon State Hospital (OSH). The latter was in turn influenced by the significant increase in the last decade of hospitalization at OSH of competence to stand trial evaluation and restoration (CST) patients. Multnomah County, which contains the city of Portland, was responsible for the largest number of investigations and commitments and led the state in using a 14-day diversion alternative to commitment. This analysis may serve as a model for other states to engage in similar longitudinal research to shed light on the functioning of their involuntary commitment statutes.
Civil commitment of people with mental illness, a process intended to provide treatment to protect a vulnerable population and society from potential danger, continues to be controversial. There are substantial ethics and legal concerns which reflect conflict between beneficence, nonmaleficence, justice, and autonomy.1,–,5 Many of these concerns arose in the context of deinstitutionalization, the crisis of incarceration,6,7 and changes in commitment laws starting in the 1960s requiring, among other changes, the presence of a mental illness and an increasingly restricted finding of dangerousness.2,3
Given these concerns, one might expect that rates of civil commitment would be closely monitored and decreasing. Unfortunately, as Miller and Hanson noted (Ref. 1, p xvii), there is no national database for civil commitment. Morris8 reported that public tracking of civil commitment statistics is challenging and though he notes that some states9,10 report data online, the variability of types of commitment data make comparisons difficult. Lee and Cohen11,12 also found national data difficult to access and reported for Oregon only involuntary detentions rather than civil commitments. Recent state-wide involuntary commitment data (2015) from the National Association of State Mental Health Program Directors Research Institute (NRI) included 32 states and reveals a wide range in rates of civil commitment,13 likely reflecting difficulty in gathering comparable data as well as variations in statutes, definitions, and procedures.
The civil commitment process in Oregon begins with a signed petition alleging mental illness, and dangerousness to self or others or inability to care for basic personal needs.14 These petitions may be signed by a county community mental health program director or a police officer, or rarely by two citizens who do so by notifying the county mental health program. The situations leading to petitions nearly always require urgent evaluation in a medical facility. The police officer who signs a petition is required by statute to bring the person to a recognized medical emergency facility for evaluation by a licensed independent practitioner (usually a physician or psychiatric nurse practitioner) who decides whether to continue the petition by signing a “physician’s hold” (called a Notice of Mental Illness, or NMI), or to admit the patient voluntarily, or to release the person back to the community. The commitment process can also be initiated by a licensed independent practitioner (usually a physician or a psychiatric nurse practitioner) filing a NMI in the emergency room or during a patient’s hospitalization. The evaluating clinician determines whether the person meets the statutory definition of mental illness and if so, after consultation with a second clinician, immediately files the NMI with the court, providing the legal basis for detention during an investigation which may last for up to five judicial days.15 A judicial day is a day when the courts are open, Monday to Friday. Patients can be involuntarily medicated while on a NMI for safety, and clinicians can decide to cancel the NMI if new information or patient improvement indicates that detention under the NMI is not needed.16
Investigation17 is done by a court investigator, who works for the court but is paid by the local county Involuntary Commitment Program (ICP). Investigators are trained mental health clinicians who often discuss patients with the clinicians. The investigator then makes a recommendation to the circuit court as to whether there is probable cause for the judge to hold a commitment hearing. Since 1993, a statutory change allowed for a 14-day diversion (14DD) by which an investigator can divert the patient from a hearing by recommending intensive hospital treatment for up to 14 days.18,19 The patients who are diverted must meet the investigator’s criteria for a commitment hearing and the commitment hearing is held in abeyance. A 14DD can be rescinded if the patient becomes voluntary in the hospital, improves and is discharged, or if the patient declines to continue with the treatment plan, leading to either a commitment hearing or a release from care. Commitment hearings are held by a circuit court judge with input from additional mental health evaluators, the person’s attorney, the ICP investigator, and other witnesses, such as family or friends. If the judge finds by clear and convincing evidence that the person meets the statutory definition of “a mentally ill person,”15,20 the person will be placed under the supervision of the Oregon Health Authority (OHA) for up to 180 days. Once under OHA supervision the person may be placed in Oregon State Hospital (OSH) or may be released following the presentation of an outpatient treatment plan. Currently, the person usually comes to the judicial hearing from a community hospital where a period of active treatment is expected after commitment before transfer to OSH. The period of community hospital treatment is influenced by bed availability at OSH where there has been both a decrease in overall beds from 788 in 2000 to 602 in 2020, and an increase in competence to stand trial evaluation and restoration (CST) patients.21 Committed patients can be discharged from commitment either at the community hospital or from the OSH by a physician without an additional hearing.
Specialized criteria for civil commitment also exist in Oregon for those persons who are found incompetent to stand trial and not restorable secondary to a criminal charge, and who are still considered to be dangerous.22 Under this statute, as of January 7, 2021, 29 people had been committed to the Psychiatric Security Review Board (PSRB) as “extremely dangerous” persons with twenty-five continuing under PSRB jurisdiction (Bort A, personal communication December 7, 2021).
Previous work in Oregon by Faulkner and colleagues23,–,26 explored various aspects of the civil commitment process. In addition, articles by Bloom,5 and Bloom and Williams27 noted that Oregon commitment laws changed in 1973 in keeping with national trends to protect constitutional rights and due process. This major revision lead to the present iteration of the civil commitment law establishing that to be considered mentally ill, the person had to have a mental disorder and to be either dangerous to self or others, or “unable to provide for his basic personal needs and is not receiving such care as is necessary for his health and safety” (Oregon’s version of grave disability).28 Procedural due process was also increased, including a right to legal counsel, requirement for an investigation to assure probable cause to believe the person met these criteria, and the institution of a beyond a reasonable doubt standard of proof for the court.
In 1979, the U.S. Supreme Court found in Addington v. Texas29 that the clear and convincing standard of proof was adequate to protect the rights of individuals in civil commitment proceedings. Oregon then changed the standard of proof in its statute to clear and convincing evidence.30 Bloom et al.31 reviewed Oregon Court of Appeals civil commitment decisions from 1998 to 2015 and reported that the appeals court continued to require a high likelihood of risk for harm. This made even clear and convincing evidence a high bar for commitment such that grave disability was interpreted to mean that the person would not survive in the near term in the current circumstances. In 2015, the Oregon Legislature changed the basic needs criteria to “unable to provide for basic personal needs that are necessary to avoid serious physical harm in the near future and is not receiving such care as is necessary to avoid such harm,”32 a broader statutory standard than the Oregon Court of Appeals had promulgated in its opinions up until that point. If the Appeals Court changed its previous approach because of the new legislative definition of grave disability awaits further research.
The information on civil commitment and its controversies that we have just presented serves as the background for a detailed examination of civil commitment in Oregon. This article provides complete civil commitment data from the signing of the NMI to the results of judicial commitment hearings in Oregon from 1996 to 2020. The goal is to expand on data reported in earlier studies33 going back to 1972, which then provides a unique opportunity to illustrate factors affecting civil commitment over many decades in Oregon. The discussion addresses comparative data from other states, and possible consequences of the decline in Oregon’s use of civil commitment. The paper may serve as a model for other states to engage in similar longitudinal research to shed light on the functioning of their civil commitment statutes over extended periods of time.
Method
The OHA Office of Health Analytics provided data detailing the number of civil commitment investigations, number of commitment hearings, and number of civil commitments for the years 1996 to 2020. The percentages of investigations leading to formal judicial hearings and from hearings to commitment were then calculated and the state population in each year was used to calculate rates adjusted for population. Similar data for commitments and investigations in 1972, 1983, 1993, and 2013, were also provided by OHA to the authors of earlier publications.29,30 The OHA also provided the average daily census at OSH from 2000 to September 30, 2021.
The Portland metropolitan area includes Multnomah (including the city of Portland), Clackamas, and Washington counties, which in 2020 contained 43 percent of Oregon’s population. Each of these counties has a mix of urban, suburban, and rural areas, but not in the same proportions. Given the likelihood of variation in services available compared with more rural parts of the state, data were requested from the Behavioral Health Departments of each county (including 14DDs) and adjusted by population (full data for all three counties mentioned above was only available from 2013 to 2020). Multnomah County could provide 14DD data only for 2016 to 2020. The Oregon Justice Department provided statewide data on 14DDs for January to December 2020.
This project was reviewed by the Oregon Health & Science University IRB (Office of Research Integrity) and waived from monitoring as it was not found to involve human subject research.
Results
Oregon’s civil commitment rates (all rates are per 100,000 unless stated otherwise) dropped steadily from 53.2 in 1972 to 9.2 in 2020. Table 1 includes the numbers of investigations, hearings, and commitments, and the percentage reduction of numbers between each stage (investigations to hearings, hearings to commitment). The percentage of investigations leading to hearings fell from about 17 percent in 1996 to the seven percent range by 2013 to 2014, then increased to about 12.5 percent as the number of investigations dropped. The proportion of hearings leading to commitment has shown less variation over time from as high as 88 percent to as low as 73 percent, most recently 80.7 percent. The percentage of commitments from investigations was 14.6 percent in 1996, then fell to as low as 5.9 percent from 2007 to 2014, rose to as high as 10.0 percent in recent years, and was 8.0 percent in 2020.
Oregon Investigations, Hearings, and Commitments
Figure 1, with the new data from 1996 to 2020, shows the linear decline in commitments from 1972 to 2020 and in hearings from 2001 to 2020, with variations in rate of investigations (per 30,000 for graphing) from 1983 to 2020. Investigations, which are driven by NMIs, increased from 149.8/100,000 in 1983 to 253.6/100,000 in 2012, then began to decline, falling to 115.6/100,000 in 2020.
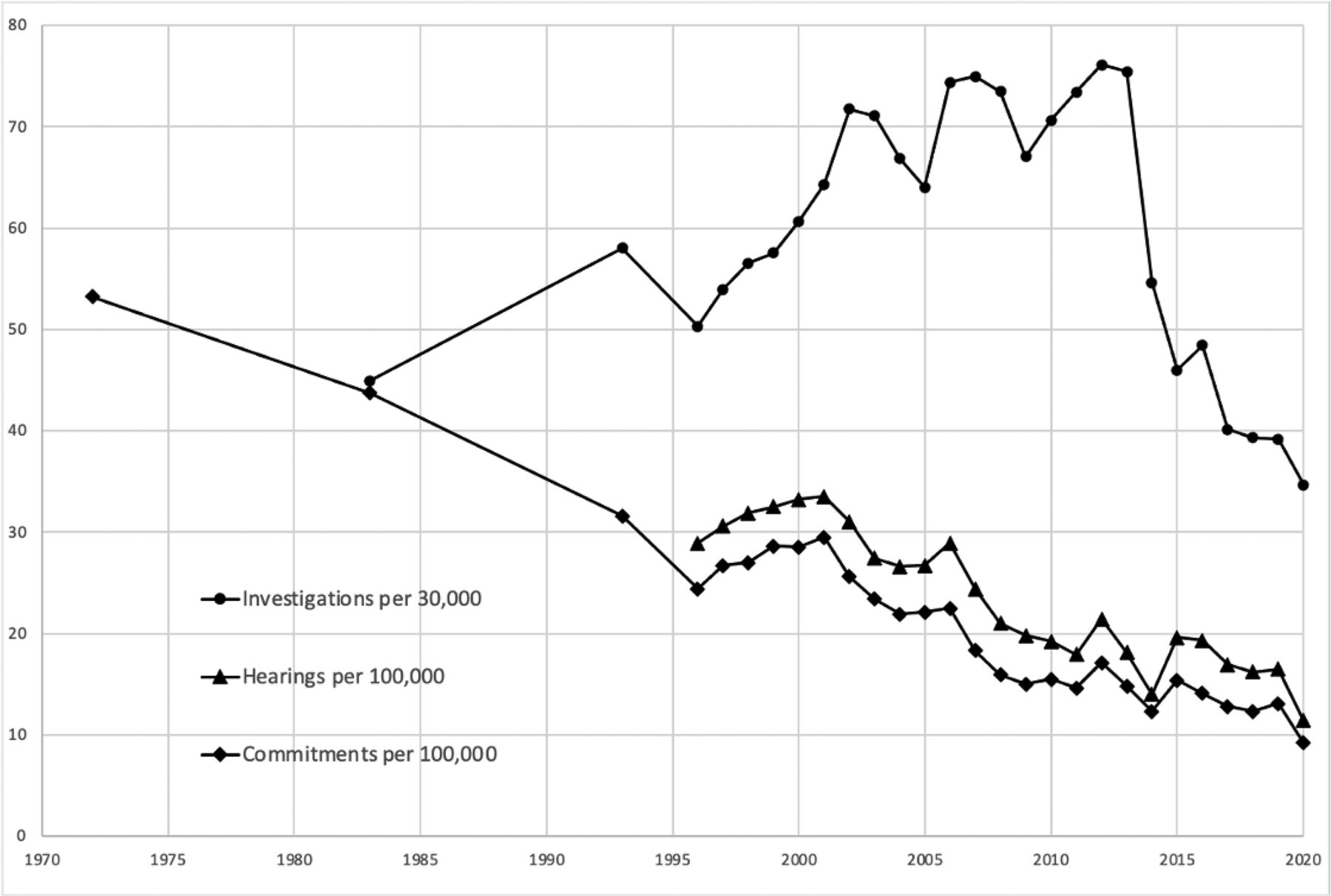
Oregon Investigations, Hearings, and Commitments.
Table 2 contains the rates per 100,000 of investigations, hearings, and civil commitments, as well as the percentage of investigations leading to 14DDs, for the three metropolitan Portland area counties from 2013 to 2020, listed in order of size of population. Rates varied from being comparable with the statewide data (Clackamas County commitments fell from 16.5 to 9.7/100,000) to being lower and dropping more for Washington County (fell from 6.8 to 1.3/100,000), with Multnomah County having a consistently higher rate (28.3/100,000 in 2020). Multnomah County committed 170 people in 2020 out of the state total of 390; without Multnomah County, the state commitment rate was 5.2/100,000 compared with 28.3/100,000 in Multnomah County. Between 2016 and 2020, the use of 14DDs increased in Clackamas County (from 5.5% to 15.0% of investigations) and decreased in Washington County (17.6% to 10.9%). Utilization in Multnomah County exceeded the other counties, going from 11.9 percent to 21.5 percent.
Portland Metropolitan Area County Data
Table 3 provides 14DD data from the Oregon Justice Department for 2020 from the six most populous Oregon counties and the total use in all counties in the state. Multnomah County had the greatest use of 14DDs in absolute numbers (614) and by population (75.2/100,000). Without including Multnomah County, the overall state rate drops from 29.6/100,000 to 18.9/100,000.
14-Day Diversions (14DD) by Most Populous Counties and for State, 2020
Discussion
Civil commitment rates in Oregon declined throughout the entire study period, reaching 9.2/100,000 in 2020 with the decline accentuated during the current COVID-related reduction in bed capacity. Comparable data from other states are not available, and specific rates for other states would not in themselves indicate whether their processes are effective regarding the treatment of their citizens with serious mental illness. Before reaching conclusions about the civil commitment rates in any state it is important to examine its total civil commitment process. Oregon’s apparent low use of civil commitment now might indicate that it is only used when truly needed to improve outcomes, presumably because there is now greater use of effective community services for those who in prior years might have been committed. This would be a welcome supposition, but it does not correspond to our lengthy experience in Oregon where such programs do exist in the community but are not sufficiently robust to supplant the need for civil commitment.
Testa and West2 noted that, starting in 1964, commitment statutes among states had moved from a need for treatment to dangerousness standards. In 1988, Hiday34 reviewed empirical research on reform of civil commitment law and concluded these changes had successfully reversed the flagrant abuses of the previously paternalistic system. Further, she concluded that it did not appear that people were being abandoned because of a preference for liberty and that inclusion of grave disability with dangerousness would allow for care of people with serious mental illness. She also opined that problems such as homelessness and incarceration of people with mental illness were not a consequence of commitment law reform but caused by social factors such as lack of affordable housing and inadequate financial resources. Also in 1988, Rubin35 described how economic principles involving costs and benefits to society and individuals might influence how commitment laws develop, with the optimistic thought that costs could be contained, rights respected, and better treatment provided. Even prior to these articles, a 1982 study of people referred for psychiatric evaluation in an urban jail noted a high rate of severe mental illness, leading Lamb and Grant36 to suggest that the diversion of patients to jails might indicate the need for greater use of involuntary treatment.
In contrast to what was envisioned in these articles from the 1980s, we now see in Oregon predictable consequences of insufficient hospital and community care possibly leading to homelessness, substance use, and an increase in low level criminal activity.6 Once encountered by police, a person with serious mental illness might be taken to a jail, and then need competency evaluation and restoration in a hospital bed which might otherwise be utilized for a civilly committed patient.21,37 Further insight into these processes awaits empirical studies of those who are committed in Oregon and those who are released without going to a commitment hearing.
For the changes in Oregon’s civil commitment rates over the years, the complexity of social and legal processes precludes making definitive conclusions about causation and consequences, but knowledge of contemporaneous events and circumstances can suggest relationships. Investigations, hearings, and commitments constitute the steps in the process of involuntary commitment or release in Oregon. Inspecting these steps in the data in Table 1 and Figure 1 leads to three slightly overlapping phases that are worthy of comment.
Phase 1 extends from 1972 to about 2014. The 1973 civil commitment statutory revision28 included the prongs of dangerousness to self and others and inability to provide for basic needs, Oregon’s version of grave disability. In addition, the 1973 statute contained significantly higher procedural standards and an initial beyond a reasonable doubt standard of proof. These revisions more than likely initiated the decline in civil commitments. One might have expected the effects of this statutory change to plateau, but they did not. Between 1993 and 2014 the numbers of investigations (which follow filing of an NMI) continued to rise, possibly reflecting clinical concerns about dangerousness. At the same time the number of hearings and commitments continued to fall each year. We believe that these changes may well have been influenced by decisions made by the Oregon Court of Appeals which increased the focus on clear dangerousness both in relation to danger to self and others and also to grave disability, which was construed in both areas to require imminent risk of death.31 From our direct experience, the Court of Appeals’ decisions influenced judges who in turn influenced the commitment program investigators’ decisions about which patients should be brought to hearings.
Phase 2 began in about 2013 and continued through 2020. In this phase, investigations dropped precipitously while the number of hearings/100,000 and commitments/100,000 continued to decline. Based on communication with the Multnomah County Involuntary Commitment Program (ICP), starting in about 2012 investigators actively encouraged hospital emergency departments to initially detain highly impaired or dangerous patients under a substance use treatment statute38 which allows 48 hours of involuntary detention for sobering. This statute is not a component of the civil commitment statute and does not require reporting to the courts, so the actual frequency of its use is not known, but the coincidence of ICP encouragement and the decrease in investigations suggests a possible link. Also during the time of this phase, OSH began to be overwhelmed by CST patients,21 caused in part by the requirement to admit all jailed CST detainees within seven days of a judicial order, a consequence of the Ninth Circuit Court of Appeals decision in Oregon Advocacy Ctr. V. Mink.39,40 While CST admissions increased notably in 2004, the impact on the average daily population (ADP) at OSH was greatest starting in 2014, which was followed by an unfortunate competition between civil commitment and CST admissions. With priority indirectly required for CST patients by the Mink decision and overall ADP falling from 788 in 2000 to 602 in 2020, the ADP for civilly committed patients fell from 410 (52.0%) in 2000 to 68 (11.3%) in 2020. At the same time, CST beds increased from an ADP of 74 (9.4%) to 284 (47.2%).
During this second phase, we anticipated that the 2015 legislative change in the commitment statute which attempted to clearly state that imminence of death was no longer required to establish grave disability32 might have caused more people to be committed. But to date no research has been published to demonstrate the effects of the change in language or how the court of appeals now interprets the statute.
We propose a third phase in the data, which most likely started in 2016, involving the retention of civil commitment patients in Oregon’s acute care hospitals, most clearly reflected in the rise of the use of the 14DDs. From the time that OSH opened in 1883 until it was overwhelmed with competency to stand trial patients in this second phase, the state hospital was the main facility in Oregon’s civil commitment process. The commitment statue designates that the OSH will be used for care and treatment of persons with mental illness who are assigned (meaning committed) to the Oregon Health Authority, unless otherwise ordered.41 As OSH became less and less available because of the replacement of civil commitment patients by CST patients,21 the system had nowhere to turn except to push civil commitment patients back to the counties and their general hospitals. Today, civilly committed patients are retained in various acute care psychiatric units or in general hospitals while waiting for transfer to OSH.42–43
This article’s exploration of civil commitment in Oregon included the goal of examining how statutes, legal processes, and case law influence care of people with impaired judgment and insight related to serious mental illness. The high rate of commitment from hearings could mean that there are patients who might benefit from commitment but do not have hearings. This could lead to negative consequences of undertreatment, homelessness, drug use, and criminalization of mental illness44 and need for CST services, which nationally constitute a crisis.45,46 While use of 14DDs can be seen as a consequence of insufficient access to civil commitment, the use of 14DDs could also be seen as an alternative for providing much needed supervised care. The concept that relatively short periods of initial treatment might reduce the need for longer term commitment has been proposed as a justification to use slightly longer times under initial detention in Virginia.47
In conclusion, the rate of civil commitment in Oregon has steadily dropped since 1972, with likely influences from statutory changes, judicial interpretation, and limitations in state hospital bed capacity and community alternatives. These limitations in resources have been barriers to improving public mental health services over many decades. This article may serve as a model for other states to engage in similar longitudinal research to shed light on the functioning of their statutes involving involuntary commitment over extended periods of time, ultimately leading to changes that benefit patients.
Acknowledgments
We express our appreciation to Jeanne Windham, Public Records and Internal Litigation Process Coordinator for the Oregon Health Authority, for providing data. We also received information and assistance from staff members with the Behavioral Health Divisions of Multnomah County, Clackamas County, and Washington County, the Multnomah County Circuit Court, the Oregon Justice Department, and the Archives Division of the Oregon Secretary of State’s office.
Footnotes
The authors have no financial relationships with commercial interests.
Disclosures of financial or other potential conflicts of interest: None.
- © 2022 American Academy of Psychiatry and the Law





{kind=link}