


Abstract
We examined the impact of Medicaid expansion and of race/ethnicity on medication-assisted treatment (MAT) for opioid use disorder among those referred for treatment through the criminal justice system. Using a cross-sectional design, we combined data from the Substance Use and Mental Health Services Administration’s Treatment Episode Data Set with data on Medicaid expansion and age-adjusted mortality for drug poisoning deaths. Logistic regression was performed within state panels from 2012 to 2016, with 2014 excluded due to this being the transitional Medicaid expansion year. We found that Medicaid expansion led to an increase in the use of MAT to treat those referred to substance treatment facilities through the criminal justice system. We also identified key racial disparities in the use of MAT for those referred from the criminal justice system, with Blacks and Hispanics less likely to receive MAT than non-Hispanic Whites.
Medication-assisted treatment (MAT) for opioid use disorder (OUD) in the United States has historically been politically contentious and highly stigmatized.1,2 MAT options include methadone, a full opioid agonist that is strictly regulated and typically dispensed in a clinic setting; buprenorphine, a partial opioid agonist that is heavily regulated but available from office-based physicians; and naltrexone, an opioid antagonist that reduces opioid cravings and is regulated like a standard pharmaceutical.
Policymakers have often framed OUD as a problem for the criminal justice system, with increased policing and incarceration understood as appropriate policy responses. The criminal justice model of responding to substance use disorders has helped fuel differential outcomes across racial/ethnic groups in interactions with law enforcement and the court system, in sentencing, and in the secondary consequences that flow from criminal convictions (such as decreased access to employment opportunities).3,–,5 In addition, scholars have found that referrals to substance treatment centers through the criminal justice system are less likely to receive MAT than others, suggesting an important gap in services for OUD.6,7
The ongoing opioid epidemic has led to a shift among policymakers toward a medical model for confronting OUD, with increased attention directed to MAT as an evidence-based means of addressing OUD, preventing overdose deaths, and preventing the spread of diseases such as HIV and Hepatitis C.8,–,12 Access to MAT may also help reduce future contacts with the criminal justice system.13 Importantly, research on media and public policy framing of the current epidemic has suggested that the shift toward a medical model is associated with the increased proportion of non-Hispanic Whites among those diagnosed with OUD.14,15
Growing attention to OUD as a public health rather than criminal justice problem among policymakers has been complemented by changes implemented under the 2010 Patient Protection and Affordable Care Act (ACA).16 These changes have created potential pathways toward expanded MAT access. State-based exchanges for purchasing health insurance have increased overall coverage. Building on the earlier Mental Health Parity and Addiction Equity Act, insurance regulations have been altered with the intention of expanding access to substance use disorder services.17
Implemented in 2014, Medicaid expansion under the ACA has created another potential route toward increasing MAT access.18 For individuals referred for substance use treatment through the criminal justice system, Medicaid expansion may remove financial obstacles to evidence-based care. At the same time, variation in the implementation of expansion has the potential to foster new disparities in access or reinforce existing patterns. Although the ACA was intended to expand Medicaid coverage for a large portion of the low-income population throughout the United States, the Supreme Court’s 2012 decision in National Federation of Independent Business v. Sebelius19 altered these provisions. Under this decision, state governments decide whether or not to expand Medicaid to cover those living in households making up to 138 percent of the federal poverty level.20 The result is significant cross-state variation in access to insurance through Medicaid.
Recent research has sought to examine the impact of Medicaid expansion on access to MAT and to identify patterns in MAT use. Work in this arena has identified significant growth in MAT access in states where Medicaid was expanded.21,–,24 Critically, research on racial/ethnic disparities in MAT use has pointed in different directions. Researchers found that counties with a higher percentage of Black residents were less likely to have outpatient substance use disorder facilities that took Medicaid.25 Researchers have also identified higher uptake of buprenorphine in areas with larger White populations, a finding that further suggests that minority groups may be getting left behind as MAT has become available in a less strictly regulated form.26,27 A notable recent article, however, has suggested that African Americans and Hispanics may be more likely to receive MAT than non-Hispanic Whites.28
An impressive array of studies has sought to illuminate the impacts of Medicaid expansion. At the same time, important work has been done on racial/ethnic disparities in MAT. Nonetheless, little is known about the relationships between the criminal justice system, MAT, and Medicaid expansion or between the criminal justice system and access to MAT across racial/ethnic categories. Understanding these relationships is important because Medicaid expansion is a primary means through which access to care has been increased in recent years and because the criminal justice system is a key institutional driver of racial/ethnic disparities across multiple metrics.4,5
In this study, we used data from the Substance Abuse and Mental Health Services Administration’s (SAMHSA) Treatment Episode Data Set, data on state Medicaid expansion, and data on drug-related deaths from the Centers for Disease Control and Prevention.29,–,31 We considered the impact of Medicaid expansion on access to MAT for those referred for treatment from criminal justice settings and analyzed racial/ethnic disparities among criminal justice referrals to substance use treatment facilities. As a point of reference, we also considered the impact of Medicaid expansion on non-criminal justice referrals and examined racial/ethnic patterns in MAT among non-criminal justice referrals.
Methods
Data
The primary data source for this study was the 2000–2017 Treatment Episode Data Set (TEDS), collected by and publicly available from SAMHSA. TEDS reports admissions to substance use treatment centers that receive public funding, which are compiled from state agency data systems and fully de-identified. TEDS captures individual admissions, rather than individual people. This means that, throughout, our unit of analysis is individual admissions to substance use treatment facilities. TEDS encompasses U.S. states, Washington, DC, and Puerto Rico. Georgia and Oregon were excluded from this study because of incomplete TEDS data over time. West Virginia did not report data on MAT use and was also excluded. We excluded Puerto Rico because its Medicaid program operates in a distinct manner, with a different funding formula.
We restricted our statistical analysis to admissions (n = 2,200,822) where any opioid was the primary substance used at admission in 2012-2013 and 2015-2016. Descriptive statistics for the data are shown in Table A1 in the Appendix. These opioids included heroin, morphine, nonprescription methadone, and the full range of other opiates/synthetics, including codeine, hydrocodone, oxycodone, and tramadol, among others. Our central outcome of interest was the planned use of MAT options such as methadone, buprenorphine, and naltrexone as part of a treatment plan among admissions referred through the criminal justice system. We note that TEDS data does not differentiate between methadone, buprenorphine, and naltrexone.
The criminal justice-referred admissions analyzed included referrals from judges, prosecutors, probation officers, and others affiliated with federal, state, or county court systems. This encompasses a wide swath of circumstances, such as deferred prosecution, pretrial release, pre- or post-adjudication cases, work release, and civil commitment. We also analyzed racial/ethnic disparities in MAT among criminal justice referrals and non-criminal justice referrals. The distinction between race and ethnicity as reported in the TEDS data corresponds to the conventional use of race and ethnicity by the U.S. Census Bureau. The questionnaire on which TEDS is based inquires about race and ethnicity as separate categories. Therefore, both race (Black, White, etc.) and ethnicity (Hispanic or non-Hispanic) are recorded for each admission in the data. While Hispanics can identify with any racial group, we treat Hispanics as a distinct group, categorizing as Hispanics all those reported as Mexican, Puerto Rican, Cuban, or unspecified Hispanic in the data and differentiating them from non-Hispanics within the same racial group (e.g., White Hispanic versus non-Hispanic White). In separating Hispanics and considering their outcomes along with those of each race, we treat the Hispanic category akin to a racial group while recognizing that the Hispanic category is understood as an ethnicity in the United States and treated as such in the TEDS data. We combined TEDS data with data on state Medicaid expansion accessed via the Henry J. Kaiser Family Foundation30 and age-adjusted mortality data for drug poisoning deaths retrieved from the Centers for Disease Control and Prevention’s Web-based Injury Statistics Query and Reporting System.31
Statistical Analysis
Following the approach of Schiff et al.,32 we used logistic regression at the individual admission level to estimate the relationship between Medicaid expansion and our binary outcome variable, which was whether or not an individual was assigned MAT following admission to a substance use facility.
The logistic regression was performed within state panels from 2012 to 2016. Observations in 2014 were excluded due to this being the transitional Medicaid expansion year. States that changed their status from nonexpansion to expansion during 2015 or 2016 (Alaska, Indiana, Louisiana, Montana, Pennsylvania) were excluded. Because Georgia, Oregon, and West Virginia were excluded because of incomplete data, the analysis encompassed 42 states and Washington, DC. The logistic regression included relevant control variables: whether an admission was referred through the criminal justice system; age; sex; race/ethnicity; employment status; education; whether the admission occurred after a previous admission; annual age adjusted state deaths from drug poisoning; and an indicator variable for state Medicaid expansion. We also include interactions between race/ethnicity and Medicaid expansion, as well as race/ethnicity and criminal justice system referral, to assess disparate impacts of expansion by race/ethnicity and referral by the criminal justice system.
We computed adjusted odds ratios of MAT versus the interaction of Medicaid expansion and race/ethnicity to assess the marginal increase/decrease in the odds of treatment following Medicaid expansion by racial/ethnic group. We also calculated the partial dependency of the predicted probability of MAT in the logistic regression versus Medicaid expansion, disaggregated by race/ethnicity. To compute the partial dependency, for each admission in the dataset we calculated the logistic regression probability of MAT with and without Medicaid expansion (while holding the other variables for each admission fixed).
Results
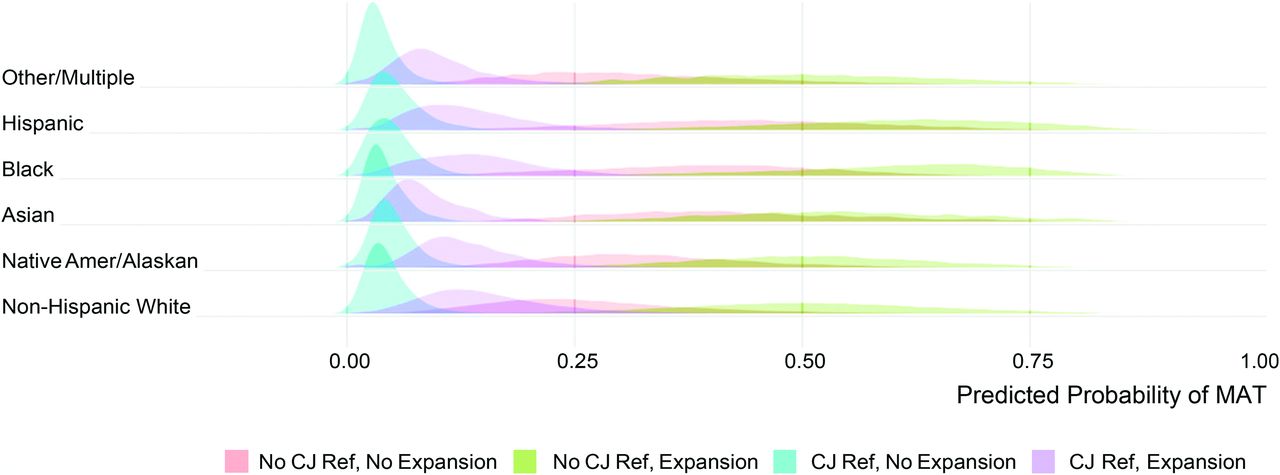
In Fig.1, we display the partial dependency distribution of the MAT probabilities from the logistic regression versus Medicaid expansion, disaggregated by race/ethnicity and the criminal justice referral variable. We note that these distributions are multi-modal, due to the large effects of both Medicaid expansion and whether an individual was referred by the criminal justice system. Here, we see that individual admissions referred by the criminal justice system had on average a lower probability of MAT. The variation within each of the four groups was due to variations in age, education, employment, and drug poisoning deaths in the states across the data.
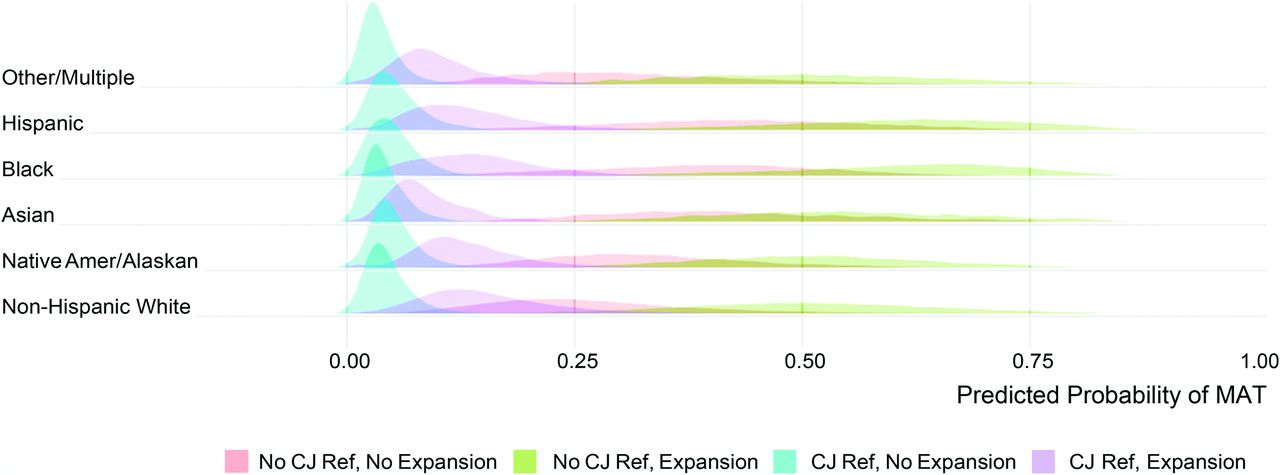
Partial dependence plot of logistic regression predicted probability of medication-assisted treatment (MAT) versus race/ethnicity disaggregated by Medicaid expansion and criminal justice referral.
In Table 1, we report the adjusted odds ratio of MAT for individual admissions in states with Medicaid expansion relative to individual admissions in states with no expansion. We found that when controlling for the other factors listed above, the odds of treatment were larger for admissions in states with Medicaid expansion (odds ratio = 3.014 [2.987, 3.043]). We also display the adjusted odds ratio of MAT versus the interaction of race/ethnicity and Medicaid expansion relative to White admissions. We found that other racial/ethnic groups, while having a greater likelihood of being assigned MAT in expansion states, had less of an increase compared with Whites of the same age, employment, education, and other control variables.
Adjusted Odds Ratios of Medicaid Expansion, Criminal Justice Referral, Expansion, Race/Ethnicity Interaction, and Criminal Justice Referral Variables from Logistic Regression
Importantly, we found that, when controlling for the other factors listed above, the odds of MAT in Medicaid expansion states are smaller for criminal justice-referred admissions (odds ratio = .126 [.123, .129]). We also identified critical disparities in treatment among those referred through the criminal justice system. Among criminal justice-referred admissions, we found that Blacks were less likely to receive MAT than Whites when controlling for other factors in the logistic regression (odds ratio = .644 [.613, .677]). Criminal justice-referred Hispanics were also less likely than Whites to receive MAT (odds ratio = .559 [.537, .583]).
In Table 2, we display the partial dependence of the probability of MAT in the logistic regression and Medicaid expansion. When averaged across the dataset, the marginal probability of MAT was .263 in the logistic regression when individual admissions were not exposed to Medicaid expansion and .465 when admissions were exposed to Medicaid expansion. In addition, we compute the marginal probability of MAT with respect to the interaction of Medicaid expansion and race/ethnicity. Here, we found that Black and Hispanic individuals had the highest probability of MAT when exposed to Medicaid expansion. These results are partially explained by Black and Hispanic individuals having higher ages on average in the data compared with White individuals, where higher age is associated with higher probability of MAT (see Table A2 in the Appendix). We also note a significant effect of race/ethnicity in the logistic regression, where Black and Hispanic group variables had a higher (positive) value relative to White. In Table 3, we display the partial dependence of the probability of MAT in the logistic regression and Medicaid expansion, disaggregated by whether the individual was referred by the criminal justice system. We found that expansion increased the probability of MAT from .307 to .528 for individual admissions not referred by the criminal justice system, whereas the probability of MAT increased from .046 to .147 for individuals referred by the criminal justice system.
Partial Dependence of Logistic Regression Predicted Probability of Medication-Assisted Treatment (MAT) versus Medicaid Expansion and Interaction of Expansion and Race/Ethnicity
Partial Dependence of Logistic Regression Predicted Probability of Medication-Assisted Treatment (MAT) versus Medicaid Expansion and Criminal Justice Referral (CJ Ref.) Variable
Discussion
Medicaid expansion significantly increased the average predicted probability that individual admissions referred through the criminal justice system would be assigned MAT. While the predicted probability that a criminal justice-referred admission in a nonexpansion state would receive MAT was .046 [.045,.046], it grew to .147 [.146, .148] in expansion states. These findings highlight the importance of Medicaid expansion in increasing access to evidence-based treatment for OUD among those referred for treatment through the criminal justice system. At the same time, they emphasize a distinct failure: while MAT use is substantially higher among criminal justice referrals in expansion states, it still lags behind the rest of the population. Among those referred for treatment from non-criminal justice settings, Medicaid expansion led to an increase in the likelihood of being assigned MAT from .307 [.306, .307] to .528 [.528, .529].
When we consider racial/ethnic patterns in MAT among those referred through the criminal justice system, we observe stark racial/ethnic disparities. Relative to White criminal justice referrals, Black and Hispanic referrals were substantially less likely to be assigned MAT as part of a course of treatment. These patterns diverge from those observed among the non-criminal justice population, where Blacks and Hispanics were more likely to receive MAT than Whites. We note that our findings on the non-criminal justice population diverge from broader well-known patterns in access to health services. One plausible explanation is that Blacks and Hispanics may have a higher likelihood of receiving MAT as a result of inherited policy legacies and geographic proximity to MAT providers.33 As the opioid epidemic has increasingly affected Whites living in suburban, exurban, and rural areas, the confluence of residential segregation and the geography of access created by earlier decisions about the location of substance use facilities may have placed Whites at a disadvantage in terms of treatment.34,35
The disadvantages in access to MAT that we identified for Black and Hispanic admissions referred from the criminal justice system highlight a key institutional factor that policymakers interested in addressing racial/ethnic disparities should consider. These disparities emphasize the role of the criminal justice system as a driver of differential outcomes across racial/ethnic categories.
Limitations
Because of how TEDS is reported, our level of analysis was individual admissions, rather than individuals. Where some researchers have chosen to exclude admissions with a prior history of admission, we addressed this potential limitation by including a control variable for prior admission. Taking this approach allowed us to consider the full extent of the TEDS data, as 1,427,376 observations (64.9%) follow a prior admission. We also performed a logistic regression that excluded individual admissions with a prior history of admission (shown in Table A2 in the Appendix). In Figure A1 in the Appendix, we plot a comparison of logistic regression coefficients including and excluding prior admissions. Coefficients across both models are correlated at .989. We note two key differences that result from excluding observations with prior admission (shown in Appendix Table A3): the coefficient for the interaction of Medicaid expansion and Black becomes positive and the coefficient for the interaction of expansion and criminal justice referral was not statistically significant. Because TEDS is compiled from state reports, data collection is not fully uniform. Methodologically, we note that the logistic regression is only able to measure associations, rather than causal dependencies, between MAT and explanatory variables such as Medicaid expansion, referral from the criminal justice system, and race/ethnicity.
Conclusions
This study found that Medicaid expansion was associated with a substantial increase in the use of MAT to treat those referred to substance treatment facilities through the criminal justice system. It also identified key racial/ethnic disparities in the use of MAT for those referred from the criminal justice system, with Blacks and Hispanics less likely to receive MAT than Whites. These findings highlight the role of institutional factors in driving critical disparities in treatment across racial/ethnic categories.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2022 American Academy of Psychiatry and the Law





{kind=link}