


Abstract
Cannabis is the most widely used drug worldwide. Data about the association of cannabis use with aggression is heterogeneous. The objective of the current study was to assess the nature of the association between cannabis use disorder (CUD) and self-directed, other-directed, and combined aggression. We used data from the National Survey on Drug Use and Health across 2008 to –2014, with a pooled sample of 270,227 adult respondents. We used regression models to estimate the odds ratios (ORs) for those having CUD perpetrating each form of aggression compared with no aggression and other-directed compared with self-directed aggression. CUD was associated with significantly increased odds of committing other-directed (adjusted OR [aOR] = 1.42, 95 percent CI = 1.26–1.60) and combined aggression (aOR = 2.11, 95 percent CI = 1.36–3.26) compared with no aggression. CUD was associated with a nonstatistically significant risk of other-directed compared with self-directed aggression (aOR = 1.29, 95 percent CI = .97–1.69). In those 18 to 25 years old, CUD was significantly associated with an increased differential risk of other-directed versus self-directed aggression (aOR = 1.29, 95 percent CI = 1.03–1.62). Cannabis use disorder seems to increase the risk of other-directed aggression compared with self-directed aggression, especially among youths.
Cannabis is the most widely used drug worldwide, with an estimated 188 million users in 2017, corresponding to 3.8 percent of the global population aged 15 to 64 years.1 Cannabis use disorder (CUD) is by far the most prevalent drug use disorder in the United States.2 It is estimated that about 9 percent of those exposed to cannabis develop a use disorder, with the prevalence reaching 50 percent if cannabis use was daily.3 The recent legalization of cannabis use in some states in the United States and the increasing potency of cannabis (i.e., increased concentration of Delta9-TetraHydroCannabinol (THC)) has reportedly led to a rise in cannabis-related health care use, accidents, and deaths.4 States adopting medical cannabis laws have been experiencing increased use of cannabis among adults, although it remains unclear whether this increase leads to greater CUD and CUD-associated risky behaviors.5
Prior research has not consistently identified a link between cannabis use and suicidality. A prospective general population cohort study published in 1990 failed to find an association between past-year cannabis use and self-reported suicide attempts.6 In a more recent study, analysis of data obtained from 1,790 individuals interviewed in the Australian National Survey of Psychosis found no significant association between cannabis use and suicide attempts, except in older men who consume the substance daily.7 A recent Canadian study of 43,466 participants found significant gender differences in the strength of the association between cannabis use, suicidality, and psychological distress, with female regular users reporting higher psychological distress and suicidal thoughts and attempts.8 Similarly, analysis of data from a survey targeting adolescents from 21 low- and middle-income countries, past 30-day and lifetime cannabis use were both significantly and independently associated with suicide attempts.9 Recent evidence from a meta-analysis highlights the low quality and high heterogeneity of the data addressing this topic but points to the duration of cannabis use being instrumental in predicting suicidal behavior: chronic cannabis use significantly predicted attempted or completed suicide in the general population, whereas acute use did not.10 Another meta-analysis also found that CUD in the general population was significantly associated with attempted suicide.11
On the other hand, earlier studies seem to regularly link cannabis use with other-directed aggression. A meta-analysis of cross-sectional studies found a mild-to-moderate association between male cannabis use and male-to-female perpetration of intimate partner violence.12 More recently, in a prospective cohort of males followed from the ages of 8 to 56, continued exposure to cannabis was associated with a higher risk of subsequent violent behaviors.13 Moreover, cannabis withdrawal increased the likelihood of interpersonal aggression.12,14 Age of first use seems to be a moderator of the potential effect of cannabis on perpetrating other-directed aggression. Self-reported use of cannabis at 15 years of age, but not at the age of 18, significantly predicted involvement in violence at 19 years of age, after controlling for socio-demographic variables and antecedents of aggressive behavior.15 Self-reported past-month cannabis use predicted violence perpetration from adolescence to early adulthood but failed to predict aggressive behavior in adulthood.16 Alternatively, self-reported cannabis use in adolescence and early adulthood (“consistent use”) predicted perpetration of intimate partner violence later in adulthood.17
We have previously shown that studying self- and other-directed physical aggression in an integrated model based on a stress-diathesis model can be useful.18 Originating in the 1960s, the stress-diathesis model conceptualized mental illness as being rooted in two sets of etiologic factors: those present from an early age and temporally stable in their effect (diathesis) and discrete factors typically occurring around the time of onset of the illness (stress).19 The integrated model of aggression considers self-directed and other-directed aggression to be “two sides of one coin” rather than two distinct entities.20 This model considers that self-directed and other-directed physical aggression can be studied simultaneously within the same population to determine predictors of the directionality of aggression. Indeed, such a model can identify predictors of one type of aggression over the other and thus help design more accurate and reliable predictive tools.18 We have previously found that individuals with drug use disorders were more likely to commit other-directed as opposed to self-directed aggression.18
Given the conflicting data regarding the association between cannabis use and aggression, we believe that a different approach is warranted and that using the integrated model of aggression can add value. The objectives of our current study are to assess the associations between having CUD and engaging in aggressive behaviors, and whether individuals with CUD were more likely to engage in other-directed rather than self-directed aggression.
Materials and Methods
Data Source
We retrieved the publicly available de-identified data of the National Survey on Drug Use and Health (NSDUH) from the Inter-university Consortium for Political and Social Research (ICPSR).21 The NSDUH is “an annual nationwide survey involving interviews with approximately 70,000 randomly selected individuals aged 12 and older” and is conducted by Research Triangle Institute (RTI) International.22 The survey is authorized by Section 505 of the Public Health Service Act, which mandates yearly surveys to collect information about substance use.22. The NSDUH research protocol is approved by RTI International's Office of Research Protection, which serves as the Institutional Review Board of the organization.22 Field interviewers are mandated to obtain informed consent from respondents before initiating the survey.23 Details about the methodology of each survey are available in the yearly methodology reports.23
For our study, we pooled data from consecutive cross-sectional NSDUH surveys from 2008 through 2014.24,–,30 As the survey was redesigned in 2014,31 subsequent NSDUH data were not used. We analyzed the data of the 270,227 adult respondents (aged 18 years or older). Institutional Review Board approval was waived.
Measures
Dependent Variable
As we previously described,18 our composite categorical variable measuring aggression (A) is based on answers to two questions: “During the past 12 months, did you try to kill yourself?” and “During the past 12 months, how many times have you attacked someone with the intent to seriously hurt them?”
The outcome categories are:
Nonaggressive (NA). No aggression reported
Self-directed aggression (SDA). At least one suicide attempt reported, and no physical assault reported
Other-directed aggression (ODA). At least one physical assault reported, and no suicide attempt reported
Combined aggression (CA). At least one suicide attempt and one physical assault reported.
Independent Variable
To design our substance use disorder variables, we relied on the NSDUH diagnostic algorithms. These algorithms were based on DSM-IV criteria, but we modified them as recommended to better fit DSM-5 criteria; we combined DSM-IV substance abuse and dependence criteria and dropped the legal criterion.32
We constructed the dichotomous independent variable (C) to measure CUD in the past twelve months. A diagnosis of CUD is positive if the respondent fulfilled two or more of the criteria detailed in Table 1.
Design of the Variable C to Measure CUD in the Past 12 Months
Control Variables
We controlled for age, sex, race/ethnicity, marital status, household type, education level, past-year employment, personal income level, area of residence, religiosity, past-year tobacco use, past-year mental illness (i.e., depressive symptoms, feelings of anxiety, and reports of emotional stress), past-year alcohol use disorder, past-year drug(s) use disorder (excluding CUD), past-year mental health treatment (i.e., inpatient hospitalization or outpatient treatment for mental health problems, excluding alcohol and drug use), past-year substance use treatment, juvenile substance use, and survey year.
Analysis Plan
We conducted our analyses using the Complex Samples module in the Statistical Package for Social Sciences (SPSS) version 21. Since we pooled data from multiple years, we adjusted sample weights by computing a variable (We) according to the following recommended formula:24,–,30

We conducted bivariate analyses for the independent and control variables with the dependent variable. The associations were measured using the adjusted F test, a variant of the chi-square test adjusted for complex samples. We set statistical significance at the alpha level cutoff of 0.83 percent after using Bonferroni’s method to adjust for multiple testing, with six comparisons being conducted across the dependent variable’s categories. We then conducted a multinomial logistic regression with the set of control variables that were significant in bivariate analyses. We adjusted the models to reach the best fit for our analysis and we documented McFadden’s R2 for each model. Finally, we calculated the adjusted OR (aOR) and its corresponding 95 percent confidence interval (CI) for committing different forms of aggression when fulfilling criteria for CUD. We conducted the same analyses among the age category 18 to 25 years old to test whether CUD’s association with aggression is stronger among youths. We restricted this analysis to the 18 to 25 age group and excluded the CA category from it because of the limited sample.
Results
Sample Characteristics
Our total sample included 270,227 adults (population size estimate [PSE] = 232,414,058). Approximately 2.5 percent of the total sample fulfilled CUD criteria. CUD was equally prevalent as other drug use disorder(s); comparatively, 8.5 percent of the total sample fulfilled criteria for alcohol use disorder (AUD). Figure 1 displays the prevalence of subtypes of aggression within the CUD group, other substance groups, and respondents without a substance use disorder. Most individuals in all subgroups reported no aggression over the past year. Close to 9 percent of individuals with CUD reported engaging in ODA. Within the total sample, the prevalence of CUD was 10.4 percent among those who reported SDA, 17.9 percent among those who reported ODA and 32.2 percent among those who reported CA. All three prevalences were significantly higher (p < .0083) in the three groups compared with the prevalence of CUD (2.2 percent) in the NA group.
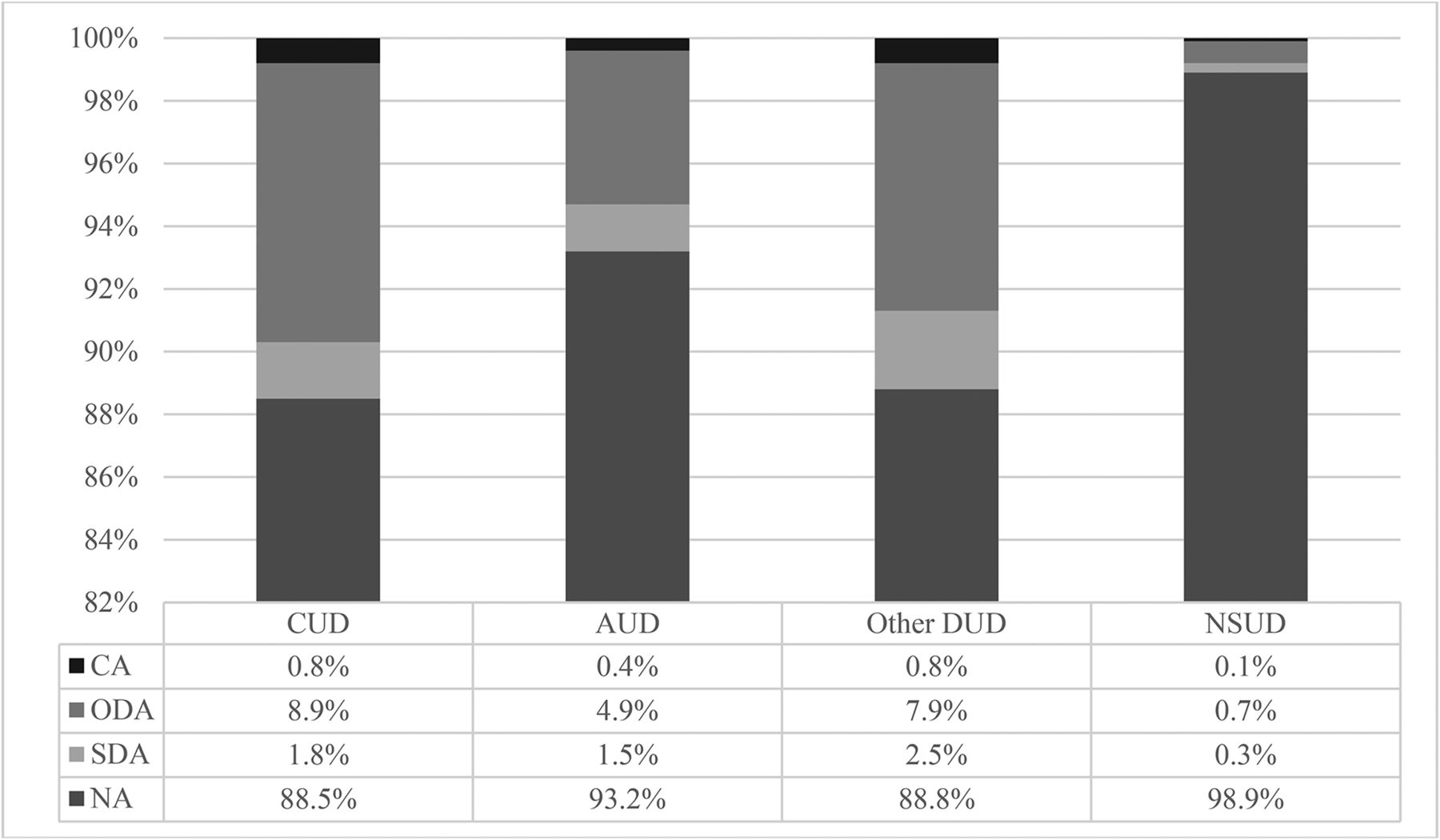
Weighted distribution of aggression subtypes (A) by cannabis (C), alcohol, and other drug use disorders. CUD, cannabis use disorder; AUD, alcohol use disorder; DUD, drug use disorder(s); NSUD, no substance use disorder; CA, combined aggression; ODA, other-directed aggression; SDA, self-directed aggression; NA, non-aggressive.
As shown in Table 2, most of the CUD subjects were 18 to 25 years old (55.0 percent), males (68.6 percent), and non-Hispanic whites (61.4 percent). More than 80 percent of this population had used alcohol and cannabis during their juvenile years.
Weighted Prevalence Estimates in Percent of CUD Sample Characteristics
Association of CUD and Forms of Aggression
As shown in Table 3, the best-fit model (R2 = 0.196) showed that CUD was significantly associated with ODA (aOR = 1.42, 95 percent CI = [1.26–1.60]) and CA (aOR = 2.11, 95 percent CI = [1.36–3.26]) only. CUD was not associated with an increased risk of ODA compared with SDA in the best-fit model (aOR = 1.29, 95 percent CI = [.98–1.70]) for the total sample. When we restricted our sample to youth (18–25 years old), the best-fit model (R2 = 0.152) showed that CUD was significantly associated with an increased differential risk of ODA versus SDA (aOR = 1.29, 95 percent CI = [1.03–1.62]) (see Table 4).
Odds Ratios from Multinomial Logistic Regression Analyses of Reporting Different Forms of Aggression on Cannabis Use Disorder
Odds Ratios from Multinomial Logistic Regression Analyses of Reporting Different Forms of Aggression on Cannabis Use Disorder among Individuals 18–25 Years Old
Discussion
We have detailed, in our literature review, the mixed evidence regarding the association between cannabis and self- and other-directed violence. In our study, we found that CUD significantly increased the odds of perpetrating ODA and CA but did not increase the odds of SDA. This is a substantial finding as both associations were identified in a nationally representative U.S. sample and remained significant after adjusting for other substance use, socio-demographic, and clinical factors. Furthermore, there is evidence that CUD favored ODA versus SDA, although this association was not statistically significant in the overall sample. Alternatively, the association of CUD with ODA was significant when we restricted our analyses to the youth.
Self-Directed Aggression
Similar to our results, a recent meta-analysis of 43 studies with 870,967 participants from a general or psychiatric population found that the effect of cannabis on suicidal ideations and attempts was weaker when compared with other substances and did not reach statistical significance.11 In specific subgroups with a psychiatric disorder, Waterreus and colleagues found no association between CUD and suicide in 1,790 patients with psychosis. In particular, the odds of attempting suicide in those who used cannabis daily remained statistically nonsignificant compared with nonusers, even after adjusting for age, depression, anxiety, hallucinations, delusions, and other illicit drug use.7
The inconsistencies in research studying cannabis use and suicide might stem from heterogeneous definitions of cannabis use across studies, as well as lack of control for potential confounders. In a recent cross-sectional study of 43,466 Canadians aged 15 years and older, regular cannabis use over the past year was associated with suicidal thoughts or attempts among men and women, irrespective of age;8 however, the study did not seem to control for other sociodemographic variables and other potential substance use. Similarly, a recent meta-analysis of nine studies analyzing the association between cannabis misuse and suicidality showed that chronic cannabis consumption could predict suicidality. The included studies were highly heterogeneous, however, and poorly accounted for confounding variables.10
There are other studies that have reported a correlation between CUD and SDA, particularly in some population subgroups. In a survey-based study by Carvalho and colleagues, past 30-day cannabis use and lifetime cannabis use were both significantly and independently associated with suicidal attempts among 86,254 adolescents from 21 countries.9 While Naji and colleagues did not find a correlation between suicide attempts and cannabis use in 909 individuals with various psychiatric disorders, they did report that an increased frequency of cannabis use among men showed a small but statistically significant association with suicidal behaviors.33 Moreover, CUD seems to be associated with attempted suicide among individuals diagnosed with bipolar disorder, as evidenced in a recent meta-analysis of 11 observational studies with low to moderate heterogeneity.34
Other-Directed and Combined Aggression
Research findings have been more consistent regarding the effect of CUD on ODA and our results replicate the available evidence. In a large meta-analysis of 96 studies assessing the relationship between drug abuse and aggression, cannabis use was identified as having a significant small-to-medium range association with intimate partner aggression.12 Also, youths using cannabis seem to be more susceptible to ODA. In a study of Mexican-American and European-American adolescents followed from the age of 15 to 19 years, self-reported use of marijuana at 15 but not 18 years of age, significantly predicted involvement in violence at 19 years, independent of sex, ethnicity, socioeconomic status, and prior status of risky behaviors.15 Similarly, data from 9,421 adolescents and young adults followed between the ages of 15 to 26 years showed that self-reported consistent use of cannabis during adolescence was the strongest predictor of intimate partner violence in adulthood.35 A prospective study of 411 males from the ages of 8 to 56 years revealed that, compared with never-users, continued exposure to cannabis was associated with a higher risk of subsequent aggressive behaviors, as measured by convictions and self-reports; this effect persisted after controlling for other risk factors of aggression, including psychiatric disorders.13
Cannabis seems to be an independent predictor of other-directed aggression among individuals with psychiatric disorders. For instance, in a sample of adult psychiatry inpatients in New Zealand, cannabis use was found to be correlated with a lifetime history of aggression.36 Similarly, in a sample of 265 patients with early psychosis, CUD was found to be a significant risk factor for aggression, particularly when combined with impulsivity, lack of insight, and nonadherence to treatment.37 Finally, in a meta-analysis of 12 studies involving individuals with severe mental illness, cannabis use was moderately to strongly correlated to aggression.38
Pathophysiology of Aggression
One hypothesis suggests that CUD promotes aggression through decreasing prefrontal response inhibition39,40 and downregulation of CB1-R in the amygdala, prefrontal cortex and hippocampus.3,41 Studies have shown that the endocannabinoid system plays a key role in regulating stress and reward responses and that continuous stimulation of this system by cannabis can disrupt its role.3 Additionally, some animal studies have shown that CB1-R knockout mice displayed significantly more aggressive behaviors in certain conditions compared with wild-type mice.41 These pro-aggression effects are modulated by the active ingredient of cannabis, THC, and become more prominent as the potency of cannabis increases.3,4 A recent meta-analysis of neuroimaging studies in chronic cannabis users also showed structural and functional deficits in the prefrontal cortex, mainly associated with inhibitory processing.42 These neurological deficits have been described as important determinants of impulsive aggression.43,–,45
Psychopharmacological effects of intoxication with or withdrawal from substances in general, and cannabis in particular, may lower the threshold for violence.46 The acute adverse effects of cannabis intoxication typically involve an impairment in cognition and emotions by producing panic, loss of control, disinhibition, intensification of negative feelings, and paranoia.47 Such effects may ultimately trigger aggressive behaviors toward others. Cannabis intoxication has also been shown to exacerbate underlying psychiatric symptomatology, such as psychosis, which can further increase the risk of other-directed aggression.47,–,50 Moreover, early research consistently demonstrated that cannabis users reported greater irritability and increased aggressive behaviors during withdrawal.51,52 Also, CUD withdrawal activates the extrahypothalamic stress system in the prefrontal cortex and extended amygdala,53,54 brain regions that have been implicated in other-directed aggression.
Another potential explanation for the link between cannabis and violence is that individuals with CUD are more likely to have several additional risk factors for violence; likely, the combination of a predisposition for impulsivity with the disinhibiting effects of cannabis leads to unplanned violent behaviors.55,56 Unsurprisingly, violence may occur while trying to get money to buy substances57 or when users become involved in illegal drug markets where aggression is commonplace.58 This again puts into perspective the range of associated risk factors that may affect the outcome of aggression in individuals with CUD.
All these mechanisms have been implicated in self- and other-directed aggression, but there is some evidence that might explain the tendency to aggress toward others rather than oneself. For instance, volunteers with no substance use disorders were found to have increased hostile attributional bias and impulsivity within two days of use of cannabis compared with days when no cannabis was used.59 We might argue that individuals with CUD exhibit higher levels of hostile attributional bias due to circuit-specific modulating effects, putting them more at risk to engage in other- versus self-directed aggression.
Limitations
Our work has several limitations. First, although we coded our exposure variable to further resemble DSM-5 criteria, it does not fully comply. This might have underestimated the prevalence and impact of substance use disorders in our population. With regards to CUD, the NSDUH did not include a “withdrawal criterion” for cannabis. But our prevalence of CUD was nonetheless in line with another study that used validated DSM-5 diagnostic tools.2 Second, despite the fact we pooled seven consecutive years of cross-sectional data, we had to adjust our analyses due to low sample sizes in some categories: for example, we had to exclude the Combined Aggression category to perform our youth-specific analyses. This has limited our understanding of whether cannabis use is associated with combined aggression in this at-risk population. Third, our outcome measure was based on two survey questions and strictly focused on physical aggression without appreciating the behavior’s context and circumstances. This limits the generalizability of our findings with regards to nonphysical forms of aggression. Fourth, our algorithm to diagnose past-year psychiatric disorders is not based on DSM-5 criteria. It is based on a mathematical equation that considers information from screening tools and has low sensitivity and specificity.23 It is, therefore, possible that it underestimated the prevalence and impact of mental illness on the outcome. Fifth, our information is based on the respondents’ answers, which might be affected by recall bias; furthermore, the NSDUH survey did not include homeless and institutionalized individuals, limiting the generalizability of our findings. Given that the NSDUH sample is strictly representative of the U.S. general population, our results may not be generalizable to other cultures. Finally, our study design is cross-sectional and we, therefore, cannot establish a causal relationship between cannabis exposure and the reported outcomes.
Conclusions
The use of cannabis has significantly increased over the past few years. As a result, CUD has become an important and relevant public health concern. As shown in our study, CUD is independently associated with a significantly higher risk of exhibiting other-directed aggression but not self-directed aggression. Among youths, we found that CUD predicted the directionality of aggression in that it differentially predicted other-directed as opposed to self-directed aggression. Further research is needed to explore the mechanisms by which cannabis differentially promotes other-directed and not self-directed aggression, especially among youths.
Acknowledgments
Research reported in this publication was supported by the Fogarty International Center and Office of Dietary Supplements of the National Institutes of Health under Award Number D43 TW009118. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Mr. Trad was involved in this research under the Medical Research Volunteer Program (MRVP) at the American University of Beirut.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2022 American Academy of Psychiatry and the Law





{kind=link}