


Abstract
The relationship between cannabis use and violence, and to what extent this association is causal in nature, remains unclear. The aim of this scoping review was to ascertain whether cannabis use increases the risk of violence and aggression in adults. Because cannabis use can result in irritability, disinhibition, and altered cognition, it is plausible that its use increases the risk of violence and aggression and that this association is exacerbated in psychiatric illness. A search of the literature using PubMed, Scopus, and PsycINFO databases was performed; all materials published in English until April 2020 were considered. Peer-reviewed publications that assessed cannabis use and perpetration of violence or aggression in adults were included in this review. Of the 327 articles that were screened for eligibility, 19 articles met inclusion criteria for this review. Results suggest that there is a link between cannabis use and violence; however, this relationship is strictly correlational, and the strength of this relationship varies depending on the population (e.g., populations with severe and persistent mental illness versus the general population). These findings have important ramifications for treatment considerations and for public health and safety approaches.
Violence poses a serious burden on public health and safety.1 Literature suggests that violence and criminality occur at higher rates in individuals with severe and persistent mental illness (SPMI) and substance use disorders compared with the general population.2 The association between substance use, particularly alcohol and stimulants (e.g., cocaine and methamphetamine), and violence is relatively well established.3 The extant literature on cannabis and its relation to violence, however, is much more limited and nuanced. There is debate whether the relationship between cannabis and violence is factual or factional (i.e., characterized by dissent in the literature). Cannabis is one of the most widely used drugs after alcohol and tobacco and is the most commonly used illicit substance in most jurisdictions where it is not yet legal.1,4 More than 192,000,000 people (ages 15–64 years) regularly consume cannabis worldwide.5 These rates are increasing due to widespread availability, decriminalization, and changes in the public perception of the drug.4 According to the 2019 Quarter 1 National Cannabis Survey results, generated after the legalization of cannabis in Canada in October 2018, 18 percent of Canadians aged 15 years or older reported having used cannabis in the past three months, which was an increase from the 14 percent who reported using just one year earlier.6 Similarly, U.S. data from the 2019 National Survey of Drug Use and Health indicate that 17.5 percent of Americans aged 12 years or older reported having used cannabis in the past year, which was an increase from 15.9 percent in 2018.7
Cannabis is composed of two main ingredients: cannabidiol (CBD) and 9Δ-tetrahydrocannabinol (9Δ-THC). 9Δ-THC is the psychoactive ingredient that acts on the body’s endocannabinoid system via cannabinoid type 1 receptors, leading to mental and physical effects such as producing a drug high, altering perception, and increasing appetite.8 The general public’s perception of cannabis is that it is a relatively harmless drug associated with positive states, notably relaxation and calmness.9,10 The actual experience of being high is subjective and variable, depending on the dose of the drug, the route of administration (inhalation or oral), the environment in which it is consumed, and the expectations or experience of the user.8
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)11 includes a category for cannabis use disorder (CUD), which includes 11 criteria. One criterion is withdrawal, during which time irritability, anger, aggression, anxiety/nervousness, and restlessness can occur.12 Given that such symptoms of anger and aggression can occur in the context of cannabis use, a salient concern is the perpetration of violence related to cannabis.
Abel13 proposed four different mechanisms that could mediate the relationship between cannabis and violence: cannabis is a major cause of violence as reflected in the number of crimes associated with the drug; an underlying predisposition toward violence may be precipitated by the drug; some antisocial individuals are more likely to use drugs such as cannabis, but there is no causal relationship between their behavior and drug use; and cannabis does not incite violence but instead acts to reduce the likelihood of violent behavior in individuals who are under the influence of this drug. Moreover, a causal link between cannabis use and violence may be mediated by disinhibiting effects or withdrawal symptoms such as irritability, anger, aggression, or violent outbursts; acute adverse psychopharmacological effects such as confusion, hallucinations, panic, and paranoia that may affect emotions and cognitions in ways that enhance aggressive responses to provocations; depersonalization, defined as a change in the experience of one’s self or reality, which during cannabis intoxication can lead to disorienting qualities; violent behavior in connection with market transactions or a lifestyle that has more tolerance for deviance and risk-taking behaviors; and the purity of cannabis (e.g., its unregulated nature means that it may be laced with other drugs).14,15 While some studies report that cannabis users are more likely to engage in violent or aggressive behavior, other investigations conclude the opposite, namely, that cannabis use is unrelated to violence or even suppresses such behavior.16,–,19 To date, there is little research on the cannabis–violence relationship in adult populations, and it is unknown to what extent any association may be causal. This review seeks to determine whether a relationship between cannabis use and violence exists.
Methods
Search Strategy
A scoping review was selected over other knowledge synthesis techniques (e.g., systematic review), as it allowed us to explore a broader research question and assess multiple study designs, while still following a prescribed format. A comprehensive search of literature using PubMed, Scopus, and PsycINFO databases was performed (all sources until April 2020) according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) Statement.20 The search terms consisted of “cannabis or marijuana or THC or tetrahydrocannabinol or weed” and “violence or violent or aggressive or aggression or hostile.” Any potential bias was minimized by following predetermined inclusion and exclusion criteria, using a comprehensive search string and following PRISMA guidelines.
Selection Criteria
Only peer-reviewed publications assessing both cannabis use and the perpetration of violence or aggression in adults (age 18 years and over) were included in this review. Reviews were limited to articles published in English. Cohort, longitudinal, clinical trials, and cross-sectional studies were all included. Reasons for exclusion of publications were the following: the study involved the use of animal models; the study involved adolescent cannabis users or subjects under the age of 18 years; the study did not control for polydrug use; the study included subjects with head injuries; the study considered the results of prenatal exposure to cannabis; the study focused on cannabis use in victims of violence (rather than in the perpetrators); the study involved relational aggression or domestic violence; or the study had an extremely small sample size (n < 10).
Data Extraction
The following data were extracted from each eligible study: the year in which the study was published, total sample size, sample size of cannabis-using group, study design, sex(es) of cannabis-using group, mean age of cannabis-using group, type of population studied (e.g., inpatient, outpatient, or general population), pattern of cannabis use (e.g., frequent or infrequent cannabis use), measure used to characterize cannabis use (e.g., questionnaire or urine drug test), and method of measuring violence and aggression.
Results
The literature search yielded 325 articles that were screened for inclusion on the basis of their titles, abstracts, and full text (Fig. 1). Two publications were included through reference tracking of included studies and from published reviews of cannabis and violence. After the removal of duplicates and ineligible articles, 19 articles were considered eligible and were included in this review. Themes were not selected a priori; rather, themes emerged after analysis of the extracted data, and all articles were classified according to one of the themes. These themes are emblematic of how articles are typically grouped in the literature. The details of the studies that were included are described in Table 1 and Table 2.
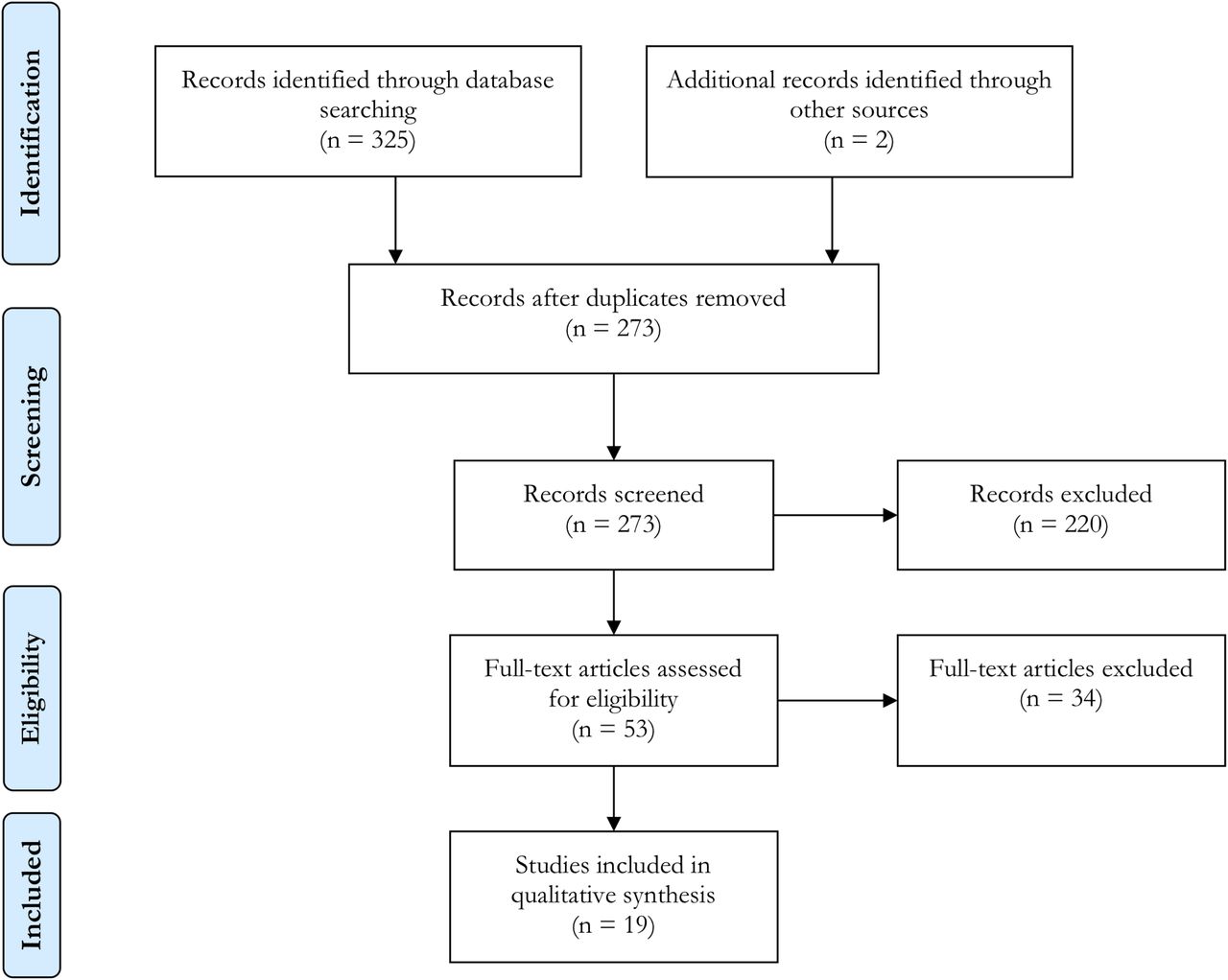
PRISMA flow diagram of literature search results.
Demographic Details of Studies Included in this Review
Population and Measurement Tool Details of Studies Included in this Review
Cannabis Alters Aggressive Responding
Four studies from the literature search suggest that cannabis use influences aggressive responding; some also revealed a dose-response relationship between cannabis intoxication and aggression. Taylor et al.34 administered a low versus high dose of alcohol (0.5 oz or 1.5 oz per 40 lbs of body weight) or 9Δ-THC (1.82 mg or 5.44 mg per 40 lbs of body weight) to 40 male undergraduate students. Subjects were provoked in an electric shock paradigm whereby aggression was measured by the intensity of the shock the subject set for his opponent to receive. The results revealed that, whereas subjects in the high-dose alcohol condition set significantly higher shocks for their opponents than subjects in the low-dose alcohol condition, high-dose 9Δ-THC did not elicit aggressive responding and, in fact, suppressed such responding. Another study by Myerscough and Taylor30 replicated these data using a similar electric shock paradigm, where low-dose 9Δ-THC facilitated more aggressive responding compared with moderate- and high-dose 9Δ-THC. These data paradoxically suggest that a dose-response relationship may exist, where aggressive behavior may be facilitated by low but not by high doses of cannabis. High doses of cannabis may actually suppress aggression.
Two more recent studies have maintained that a positive relationship does not exist between cannabis use and violence, like earlier studies have suggested. De Sousa Fernandes Perna et al.23 studied aggression in intoxicated cannabis users after exposure to an aggressive stimulus. The aggressive stimuli were the Point Subtraction Aggression Paradigm (PSAP) and the Single Category Implicit Association Test (SC-IAT). The PSAP is a computer-based task in which subjects are paired with fictitious opponents to either earn money, steal money from the opponent (e.g., aggressive behavior), or have money stolen by the opponent (e.g., provocation).35 The number of thefts is used as a behavioral index of aggression in the laboratory. The PSAP is a widely used and well-validated instrument. For instance, subjects who steal more in the PSAP also tend to have higher scores on other measures of aggression and hostility,36 such as the Overt Aggression Scale37 and the Brown History of Violence.38 Cherek et al.39 reported that male parolees with a history of violence (on the basis of their criminal records) stole more money on the PSAP than parolees in the nonviolent group. Therefore, the PSAP possesses good construct and external validity. In the SC-IAT,40 positive and negative words are coupled with an aggressive stimulus (e.g., images of aggressive scenes), and subjects must respond to whether the word is positive or negative by pressing corresponding keys; hence, a quicker response to aggressive stimuli paired with positive words indicates that the subject has a positive association with aggressive behavior and a quicker response to aggressive stimuli paired with negative words indicates that the subject has a negative association with aggressive behavior. The results of the study by De Sousa Fernandes Perna et al.23 indicated that aggression significantly increased in subjects after exposure to the aggressive stimulus when they were sober. Cannabis intoxication resulted in fewer aggressive responses, however, as measured with the PSAP and SC-IAT. The authors concluded that cannabis diminishes aggressive feelings in regular cannabis users. It should be noted that subjects received a moderate to high dose of cannabis (300 μg THC/kg body weight), which diminished aggressive responses during intoxication, in line with the results of Myerscough and Taylor.30
Another study utilized an Internet survey to study aggression in long-time concomitant cannabis and alcohol users.19 Subjects reported consuming alcohol a mean of 2.17 ± 1.98 days per week with a mean of 4.55 ± 3.59 drinks consumed per drinking occasion. Subjects reported smoking cannabis a mean of 4.98 ± 2.37 days per week and rated how high they got on each occasion: 3.13 ± 1.80 on a Likert-type scale ranging from 1 (very little) to 6 (very much). Subjects had been smoking cannabis an average 14.24 ± 11.22 years. The authors concluded that self-reported aggression following cannabis consumption was less likely than self-reported aggression following alcohol consumption. Moreover, they concluded that there was no relationship between cannabis and aggression once alcohol use, age, gender, and drug history were taken into account.
In summary, the above studies do not provide persuasive evidence that cannabis use increases aggression in nonregular and regular cannabis users; rather, the data suggest that there is a more complex and nuanced relationship between cannabis and aggression. Nonetheless, cannabis may still be associated with increased aggression in other phases of drug use, such as during withdrawal, which these studies did not investigate.
Aggression during Cannabis Withdrawal
Three studies emerged from the literature search that provided data to suggest that cannabis users experiencing withdrawal pose the greatest risk of violent behavior. Kouri et al.16 recruited a sample of chronic cannabis users from the general population, consisting of subjects who had reported at least 5,000 separate “episodes” of cannabis use in their lifetime (the equivalent to smoking cannabis once per day for 13.7 years) and who reported smoking daily at the time of recruitment. The authors defined an episode as an occasion of smoking cannabis separated by at least one hour from another episode. Additionally, they recruited two groups of controls: one group consisted of subjects who had smoked cannabis fewer than 50 times in their lifetime and had not smoked more than once per month in the last year, and the second group consisted of subjects who had formerly smoked cannabis daily but who had not smoked more than once per week during the past three months. Using former or infrequent smokers as controls, as opposed to cannabis-naïve individuals, minimized confounding variables between subjects who had never tried cannabis from those who had used. The investigators observed that the chronic cannabis users displayed significantly more aggressive behavior during the first week of cannabis abstinence compared with the control groups, specifically on days 3 and 7, as measured with the PSAP. After 28 days, aggressive behavior returned to prewithdrawal levels. Other studies in chronic cannabis users from the general population have reported that irritability, anxiety, anger, and aggression commence between days 0–3 of abstinence and can last up to 14 days.22,27
Conversely, an investigation of adult cannabis users examined whether there was a relationship between cannabis withdrawal and general aggression, that is, aggression that was rooted in a pattern of antisocial behavior as opposed to relationship aggression, which results from poor conflict resolution abilities that are typically not due to antisociality.33 Using the Alcohol Use Disorder and Associated Disabilities Schedule-IV41 to assess both general aggression and cannabis withdrawal, the study authors found no association between cannabis withdrawal and general aggression and no interaction between cannabis withdrawal and history of aggression on general aggression.
Despite some debate as to whether there is a relationship between aggression and cannabis withdrawal, evidence seems to suggest that the two are related, particularly in the first week of withdrawal. On the other hand, all of the studies identified in this search investigated samples of the general population, and these results may underestimate the prevalence and severity of cannabis withdrawal in specific subpopulations. We maintain that there is insufficient evidence at this time to conclude that cannabis withdrawal does not contribute to aggression in certain segments of the population, such as those with SPMI.
Cannabis Use and Violent Criminal Behavior
Substance use is often linked to crime, and cannabis use is no exception as demonstrated by the five studies that emerged from the literature search. Arseneault et al.17 studied a regular birth cohort from the Dunedin Study, a longitudinal study of health, development, and behavior in New Zealand. The cohort was assessed at multiple follow-up points: ages three, five, seven, nine, 11, 13, 15, 18, and 21 years. The data from the age 21 assessment demonstrated that cohort members with cannabis dependence, diagnosed according to criteria from the Diagnostic Interview Schedule for DSM-III-R,42 had a greater risk of committing a violent offense. Specifically, there was a higher prevalence and frequency of self-reported robberies, gang fights, and assaults compared with control subjects (e.g., cohort members who did not meet criteria for alcohol dependence, cannabis dependence, or a schizophrenia spectrum disorder). In a separate report of the same cohort, the authors investigated whether substance use before a violent offense, juvenile history of conduct disorder, or excessive threat perception accounted for this relationship with violence.43 Study members were classified as having adolescent conduct disorder if they met DSM-IV44 criteria at 11, 13 or 15 years of age. In individuals with cannabis dependence, analyses indicated that juvenile history of conduct disorder accounted for most of the variance in the violence committed. Because conduct disorder explained most of the variance for violent behavior, cannabis dependence may have simultaneously offered less explanatory power for violent behavior. The authors concluded that young adults who were dependent on cannabis were most at risk for committing violent street crimes when untreated.
Friedman et al.24 studied violent behavior in relation to use of illicit drugs among a sample of inner city, low socioeconomic status, African-American young adults. The sample was generated from the National Collaborative Perinatal Project, an epidemiological study of maternal and child health. With respect to prevalence rates of lifetime use (until age 26 years), 57 percent of the sample used cannabis at least five times within a single month, and 44 percent of the sample regularly used cannabis. Regular use was defined as use on at least two days during a one-week period. The results of the study demonstrated the following: cannabis use was associated with a greater likelihood of committing weapon offenses and attempted homicide or reckless endangerment offenses; cannabis use at earlier ages was more strongly correlated with subsequent commission of such serious offenses; and cannabis use was positively correlated with the frequency of drugs sales and trafficking. In a later study of the same sample,25 subjects were divided into delinquent and nondelinquent subgroups using the Peer Activity and Culture section of the Texas Family, Friends, and Self Scale.45 A differential disinhibition effect of cannabis use on violent behavior was found: the low-delinquent behavior subgroup displayed a stronger significant, positive relationship between cannabis use and violent behavior or offending compared with the high-delinquent behavior subgroup.25 This was an unexpected finding; however, it suggests that cannabis use may be more disinhibiting in more drug-naïve populations. Therefore, individuals in the low-delinquent group, who were the most inhibited, may have also been the most susceptible to losing such inhibition.25,46
An association between cannabis use and homicide and drug trafficking, independent of other factors, has also been reported.26 A positive relationship between cannabis use and violent offending was also present in a sample of female prison inmates; in fact, compared with property and drug offenders, violent female offenders more frequently reported cannabis as their drug of choice.31 In an analysis of the Cambridge Study of Delinquent Development, a longitudinal study of the development of offending and antisocial behavior in a cohort of boys in London, Schoeler et al.32 reported that continued cannabis use (e.g., cannabis use across more than one time point) in males between ages 18 and 48 years was associated with a seven-fold increased risk of subsequent violence, as indexed by self-reports and convictions. Moreover, the results from structural equation modeling showed statistically significant reciprocal relationships between cannabis use and violence; not only did cannabis use predict subsequent violence, but violence also predicted subsequent cannabis use.
As evidenced by these studies, cannabis use has been shown to have an association with violent criminal behavior in both males and females, leading to the suggestion that cannabis use may be a risk factor for violence in offender populations. These data highlight the safety concerns and seriousness of problematic cannabis use in this particular cohort.
Cannabis Use in SPMI
Four studies reported a relationship between cannabis use and violent behavior in patients with SPMI. Using a multi-wave (five-assessment) follow-up design, Dugre et al.2 investigated the continuity of cannabis use across each time wave following acute psychiatric discharge. A primary affective disorder was diagnosed in the majority of the sample (52.6%), substance use disorder in 23.9 percent, a schizophrenia spectrum disorder in 21.6 percent, and a personality disorder in 1.8 percent. The results demonstrated that when cannabis was used across more than one time wave, there was an association with increased risk of future violence. Individuals who reported having used cannabis at four time points were more likely to display violent behavior than individuals who reported having used cannabis at three time points. These relationships were true across the diagnostic categories. The association between cannabis use across time waves and risk of future violence was unidirectional (e.g., violence across time points was not a statistically significant predictor of cannabis use). These results contrast with the conclusion drawn by Schoeler et al.32 that the association between cannabis use and risk of future violence is reciprocal. Another study replicated the results of Dugre et al.2 and concluded that CUD was a risk factor for violence in early psychosis patients, particularly when cannabis use was combined with either impulsivity, lack of insight, or treatment nonadherence.29
Dharmawardene and Menkes18 studied 141 inpatients with diagnoses of schizophrenia, bipolar disorder, or schizoaffective disorder. Eight percent of the sample had a history of either violence, self-harm, or both. The study authors reported that, while controlling for other variables such as alcohol use, higher scores on the Cannabis Use Disorders Identification Test, Revised (CUDIT-R)47 significantly predicted lifetime history of violence, as measured by clinical records and self-report. Females were more likely to have histories of self-harm, which also correlated positively with CUDIT-R scores. In short, it is the consensus across the literature that an association exists between cannabis use and the perpetration of violence in patients with SPMI. The directionality and reciprocity of the cannabis-violence relationship, however, is more challenging to discern.
Cannabis Use in Substance Use Disorder
Two studies investigated violence and aggression in individuals with substance use disorder. Bácskai et al.21 reported that individuals with cannabis dependence endorsed higher scores on the self-report Buss Perry Aggression Questionnaire48 (includes physical, verbal, hostility, and anger subscales) compared with controls from the general population. In addition, females scored significantly higher on the hostility and anger domains, suggesting that aggression in females with cannabis dependence is more pathological or, conversely, that cannabis triggers greater hostility. These data highlight the importance of considering gender differences when studying any relationship between cannabis use and violence.
Another investigation examined violence in clients with primary problems with alcohol, cocaine, cannabis, gambling, or tobacco.28 Subjects were asked to indicate whether they had consumed drugs in the six-hour period prior to a violent incident. The results suggested that alcohol, cocaine, and cannabis were all significantly related to violence; however, cannabis had the weakest relationship with violence among the substance use groups, but this relationship was stronger than the tobacco and gambling groups.
Taken together, these studies provide supporting evidence for the role of cannabis dependence on violent behavior and highlight important gender differences that must be taken into account.
Discussion
This review aimed to reveal any relationship between cannabis use and violence in the adult population. The findings of this review suggest that there is an association between frequent (whether it is misused or not) cannabis use and perpetration of aggression. At most, however, we can say that this relationship is correlational, and the strength of this relationship varies depending on the population. For example, there is a stronger association between cannabis use and violence in populations with SPMI or CUD, but this association is much weaker among individuals without SPMI or CUD.
Of the 19 studies reviewed in this article, 14 identified a relationship between cannabis use and violent or aggressive behavior in specific study populations and under specific circumstances. The specific areas of risk include the following: cannabis withdrawal, offender populations, and patients with SPMI or CUD. Three studies of cannabis users derived from the general population reported an increase in aggressive behavior during cannabis withdrawal, peaking during the first week of abstinence.16,22,27 These data are in line with the withdrawal symptoms outlined for CUD in the DSM-5.11 In offender populations, studies reported an association of cannabis use with violent crime in both males and females; specifically, cannabis use was associated with violent street crimes and drug trafficking.17,24,–,26,31 In SPMI and CUD, studies also showed a positive correlation between cannabis use and violent behavior. One study of cannabis users in the general population did not find an association between cannabis withdrawal and general aggression; these data must be interpreted cautiously, however, as they were obtained from the general population and may not reflect the rates and severity of cannabis withdrawal in other, more vulnerable populations (e.g., inpatients or individuals in treatment).33 The remaining studies reported no association between cannabis use and aggression nor did they find that cannabis use suppressed aggressive responding.19,23,30,34
Limitations
There are several limitations in the cannabis and violence literature. First, there is considerable variability in study design, resulting in differing methodologies. The definitions and measures of cannabis use, violence, and aggression also differ greatly across studies. For example, regular cannabis use was defined as using cannabis more than 25 days per month in the study by Budney et al.,22 whereas in the study by Friedman and colleagues,24,25 regular use was defined as using cannabis at least two times a week. Consistent definitions matter because cumulative effects of cannabis can ensue, as it can take over a month for cannabis to be eliminated from the body.49 Second, not all of the literature provides information on the route of cannabis administration (e.g., smoking or orally), the drug dose or amount, the strain of cannabis, or the 9Δ-THC:CBD ratios. Although some of this information may be difficult to collect, these are important data as variations in cannabis consumption create different experiences and, subsequently, produce different behaviors. Most cannabis-violence studies only assess frequency of cannabis use, even though the route and dose of cannabis are known to result in different effects; for example, smoking cannabis produces more rapid and intense effects, which may influence behavior differently.8 Third, because cannabis is unregulated in most regions, street cannabis may contain traces of other psychoactive substances that could be the true cause of violent or aggressive behavior in a cannabis user and not the cannabis itself.12 Hence, the source and purity of cannabis used by the subjects in such studies are key to interpretation of results. Fourth, studies must account for whether the individual was under the influence of cannabis and other drugs at the time of a violent event. If, for example, a cannabis user is intoxicated with cannabis plus another drug at the time of a violent act, it then becomes more difficult to attribute the violence or aggression to cannabis. Although all of the studies in this review controlled for alcohol and polydrug use, many of the studies published on cannabis and violence do not. Fifth, geographic location (e.g., rural versus urban) and socioeconomic status must be taken into account due to differential social, economic, and situational factors that lead to alternative patterns of substance use.50 For example, the findings of the studies by Friedman et al.24,25 were based on a sample of inner-city, low socioeconomic status African Americans, which does not allow for generalization to other populations.
Generalizability of study results is key. The studies discussed in this review considered individuals whose drug of choice was cannabis and only considered the relationship between cannabis use and violence. These findings may, therefore, lack ecological validity because many individuals engage in polydrug use.51 A CUD diagnosis is associated with greater lifetime use of drugs from other classes and greater current use of multiple illicit substances.4 Steele and Peralta52 reported that subjects who used both cannabis and alcohol reported higher levels of physical aggression compared with monodrug users of alcohol or cannabis. Nonusers in turn reported lower levels of physical aggression compared with monodrug users. Therefore, other substances in addition to cannabis must be considered in studies of drug use and aggression.
Finally, the major limitation of a scoping review approach is that it lacks an assessment of the quality of the evidence and gathers information from multiple study designs. Moreover, scoping reviews do not necessarily provide a synthesized result but rather an overview of the literature.
Future Directions
First, future studies on the cannabis-violence relationship should use clear, standardized definitions of violence and aggression in addition to what regular (or frequent) cannabis use actually constitutes. Much more detailed data on the type of cannabis and patterns of use (including dose, quantity, and frequency) are necessary (e.g., number of joints, grams per joint, number of days cannabis is used per week, route of administration, 9Δ-THC:CBD ratios). We recognize that this information is not always easily obtainable. Second, some studies fail to control for factors such as alcohol use, tobacco use, geographical location, and personality traits. It is important to control for these features because they are all confounding variables that could drive the cannabis-violence relationship to some degree. Third, current studies rely heavily on self-report of cannabis use, which may be inaccurate due to biases in retrospective memory and social desirability.19 In one study assessing the validity of self-reported cannabis use, more than two-thirds of a sample of frequent cannabis users tested positive on a urine drug test, despite many having claimed not to have used cannabis in the preceding week.53 Accordingly, future studies should make use of urine toxicology analyses in addition to self-report. Given the lack of females in the described study samples, we encourage more recruitment of females and under-represented groups in future studies. Further studies are needed to understand the underlying mechanisms that contribute to an association between cannabis use and violence; longitudinal studies will be beneficial in this respect to suggest or provide insight into cause-and-effect relationships.
Clinical Implications
Given the relationship between cannabis use and violence, there are important implications for both clinicians and patients. In clinical settings, cannabis use should be queried and monitored, and patients, particularly those with SPMI or histories of violence, should be actively discouraged from using cannabis as a way to reduce risk and improve patient well-being. Psychotherapeutic techniques such as motivational interviewing, contingency management, or cognitive-behavioral therapy, which have all been shown to reduce cannabis use, could be particularly helpful in this regard.54,–,56 Clinical trials of certain pharmacotherapies, such as the anticonvulsant gabapentin and the glutamatergic agent N-acetylcysteine, have shown promising results for the reduction of cannabis use, craving, and withdrawal symptoms; however, more research is needed in this area.57,58 A combination of both psychotherapeutic and pharmacological interventions will likely be most effective in reducing cannabis use. For patients with SPMI or histories of violence, it is critical to curb cannabis use given the stronger associations between cannabis use and violence. For instance, in patients with recent-onset psychosis, reductions in cannabis exposure were related to improvements in patient functioning as assessed with the Global Assessment of Functioning Scale.44,59 In states where cannabis has been legalized (e.g., Colorado, California, or Vermont), it might be reasonable to place more restrictions on obtaining cannabis for individuals with a history of violence.60
There are further implications to reducing cannabis use from a public health and safety perspective. Intervention programs that concurrently target both cannabis use and violent behavior are of particular importance and should focus on early detection and preventive strategies, perhaps beginning in adolescence.17 Research into the cannabis-violence relationship will be vital for designing such programs relevant to cannabis misuse (as well as cannabis misuse plus polydrug use) and violence prevention.4,9,10
Conclusions
Considering that cannabis is the most commonly consumed illicit drug and with increasing legalization of cannabis throughout the world, it is important to understand its effects on violence and its consequences for public health and safety.1,9 The findings from this review suggest that, on the basis of the current literature, frequent cannabis use is a potential risk factor for violence and aggression, particularly in individuals who may have a unique susceptibility for engaging in violent behavior (e.g., certain individuals with SPMI). More standardized and empirical research is required. Findings from such studies will help to clarify misconceptions surrounding cannabis use and are of high relevance to clinical settings and public health and safety.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2021 American Academy of Psychiatry and the Law





{kind=link}