


Abstract
In 2005, the Chief Coroner of Ontario instituted a review into 45 cases of criminally suspicious child deaths about which a prominent pediatric forensic pathologist had expressed an opinion that the cause was homicide. Subsequently, a provincial inquiry was called to review the practice and oversight of pediatric forensic pathology in Ontario and to make recommendations to restore and enhance public confidence in forensic pathology. Recommendations from the inquiry addressed medical subspecialization, the evidentiary basis for expert opinion, oversight of the profession, and development of best forensic practices. Although the inquiry focused on pathologists, it is clear that these recommendations have significant implications for all forensic professions, including forensic psychiatry. This article summarizes the inquiry report and considers the potentially important implications for forensic psychiatry.
Pediatric forensic pathologists are often called as expert witnesses in cases involving suspicious deaths of children. Their evidence can be critical for assisting the court to arrive at a verdict in what are inevitably emotionally charged and often highly publicized cases. As with all forensic experts, it is therefore vital for pediatric forensic pathologists to have had sufficient training to perform their task and to base their opinion on best practices available in their field.
Between 1981 and 2005, Dr. Charles Smith worked as a pediatric pathologist in Toronto at a world-renowned treatment and research facility. Over the course of his 24 years of practice, Dr. Smith conducted over 1000 autopsies of children,1 many of whose deaths were suspicious. As a result of his specialized area of practice, he was called to testify in a large number of legal cases and over time became the leading expert on shaken-baby syndrome in a province of over 8 million people. Indeed in 1999, a CBC Fifth Estate documentary identified him as one of four Canadian leaders in the field.1 However, over the course of the 1990s, he was subjected to an increasing amount of criticism by the judicial system regarding his methods, competence, and, in particular, his testimony at trial. In 2005, the Chief Coroner for Ontario instituted a review of 45 cases about which Smith had expressed professional opinions that the death was either homicide or criminally suspicious.2 The coroner's review determined that Smith had made questionable conclusions of foul play in 20 cases, 13 of which resulted in criminal convictions.1 As a result, the province of Ontario established a full inquiry into the matter, chaired by the Honorable Stephen T. Goudge, a respected member of the judiciary. The inquiry was charged with two tasks: first, to review what went wrong with the practice and oversight of pediatric forensic pathology in Ontario, and second, to make recommendations to restore and enhance public confidence in forensic pathology. The review concluded that Smith actively misled his superiors, made false and misleading statements to the court, and misrepresented the nature of his expertise.3
This review is not unique. In 2005, a review of all convictions for infant deaths since 1994 was ordered in the United Kingdom following an appeals court decision to overturn the 2003 conviction of Angela Cannings, found guilty in the murder of her child. The review examined 297 cases, including 88 cases of shaken-baby syndrome. The final report by Attorney General Lord Goldsmith set out guidelines for expert witnesses as a result of what was determined to be questionable testimony.4 A related General Medical Association hearing revoked the privilege to practice of Professor Sir Roy Meadow after finding him guilty of providing erroneous and misleading evidence in an infant death case.5
At first blush, we as forensic mental health professionals may feel a certain vindication in seeing others on the firing line. On reflection, however, it is clear that the Canadian and British reviews of forensic pathologists raise critical concerns for all forensic experts in the courtroom. In this article, we examine the findings of the Goudge Inquiry into Pediatric Forensic Pathology in Ontario3 and present the lessons learned.
The Purpose of the Goudge Inquiry Report
The 2007 release of the Coroner of Ontario's review of cases involving the testimony of Smith was described as the “last and most serious blow to public faith in pediatric forensic pathology and the central role it must play in criminal proceedings involving child deaths ” (Ref. 3, p 7). Six days later, an Order in Council established a commission to conduct a review into the conduct and oversight of pediatric forensic pathology in Ontario, to make recommendations for the future use of forensic pathology in criminal investigations and proceedings. Specifically, Justice Stephen Goudge was charged with examining 20 cases identified in the earlier Chief Coroner's Review,2 where the reviewers took issue with Smith's opinion. This review arose out of a sense of public outrage and in a highly emotional atmosphere.
Commissioner Goudge did not shy away from the emotional nature of the report. Indeed, in introducing the report he noted:
In many of the 20 cases, parents or caregivers were charged with criminal offenses that bear a significant social stigma. Some of those charged were convicted and incarcerated. In some cases, siblings of the deceased children were removed from the care of their parents. In Valin's case [the niece of Mullins-Johnson], the Court of Appeal for Ontario has determined that a miscarriage of justice occurred [Ref. 3, p 8].
This review therefore was identified as necessary to restore public confidence in pediatric forensic pathology and the court's reliance on forensic experts.
Further, in the opening pages of the Goudge Inquiry report, the potential costs of expert testimony were highlighted. The attorney for William Mullins-Johnson, a man who was determined to have been wrongfully convicted of the murder of his niece on the basis of Smith's testimony, asked Smith to apologize to his client who was in the audience at the Inquiry. The following emotionally charged exchange begins the report:
DR. CHARLES SMITH: Could you stand, sir? (BRIEF PAUSE) Sir, I don't expect that you would forgive me, but I do want to make it—I'm sorry. I do want to make it very clear to you that I am profoundly sorry for the role that I played in the ultimate decision that affected you. I am sorry.
MR. WILLIAM MULLINS-JOHNSON: For my healing, I'll forgive you but I'll never forget what you did to me. You put me in an environment where I could have been killed any day for something that never happened. You destroyed my family, my brother's relationship with me and my niece that's still left and my nephew that's still living. They hate me because of what you did to me. I'll never forget that, but for my own healing I must forgive you [Ref. 3, p 5].
The tone set in the initial pages of the report is critical. It speaks to the nature of forensic testimony and the profound effect it has on individuals, society, and the court system itself. It also speaks to the seriousness with which inadequately substantiated testimony will be viewed by those charged with reviewing the conduct of forensic experts.
Findings of the Goudge Inquiry
The Goudge Inquiry report defined the role of the forensic pathologist as focusing on postmortem findings that will assist the state in the investigation of a death. Unlike other clinical pathologists, it is noted that forensic experts must be trained in, and develop an aptitude for, the legal process. They must be able to develop their documentation to serve the needs of the justice system. They must also be able to testify fairly and objectively in a manner that is accessible to the trier of fact. To meet these requirements, forensic experts must have an understanding of the legal system and legal investigative methods. In the case of Smith, it was noted that he had no formal training in forensic pathology, and at the inquiry, he admitted that he had had no continuing medical education or upgrading in this field. Sadly, the report noted that “he was willing to fill a void that no one else wanted to fill” (Ref. 3, p 13). It was also noted that, as his reputation grew, he began lecturing on these matters, including lectures to prosecutors and police officers. This further enhanced his reputation and overall credibility. The inquiry concluded, however, that Smith lacked basic knowledge about forensic pathology. It went on to say that he compounded the problem not only by being unaware of the limits of his expertise but by exaggerating his expertise to the court.3
The inquiry report noted that “the criminal justice system values finality ” (Ref. 3, p 13). That is, an ultimate decision must be reached regarding guilt or innocence and culpability must be assigned. Perhaps discordantly, the report acknowledges that in science there is a certain evolution of findings and opinions that require interpretation for the purposes of the legal system. If these tests are not performed competently then justice is not served and public confidence in the legal system is eroded. The report noted certain deficiencies in the methods used by Smith: that he was disorganized, his note-taking was poor, and on several occasions his work was not given to the appropriate authority in a timely manner.3 Perhaps more pertinent, the report noted that Smith did not account for contradictory evidence that may have come to his attention. He also did not consider adjusting his opinion to take into account new information. In his reports, he did not elaborate on the reasoning or provide any supportive literature that might have connected the dots between his findings and his conclusions.3
Startlingly, the report noted that Smith failed to understand his role or that he was required to give an opinion with independence and objectivity. It went on to note that when providing evidence, Smith considered himself to be an advocate for the Crown, viewing it as his responsibility to bolster the prosecution's case. The report noted that Smith had deeply held beliefs about the evil of child abuse and became overly invested in cases. Laudable though these goals were, Smith could not separate his role as an expert witness from his advocacy role, particularly in view of the fact that he admitted he had no training in giving evidence and no particular ethics guideline to correct any misconceptions that he may have had.3 The inquiry noted that the expert's role must be understandable, reasonable, balanced, and substantiated by evidence. In contrast, it repeatedly noted that Smith gave his evidence in a dogmatic manner, did not acknowledge the existence of controversy in his field, and was quite willing to testify on matters outside of his area of expertise, such as the profile of a perpetrator of a particular crime, even though his views were sometimes unsubstantiated and not based on any objective findings. It was stated that these problems were exacerbated by the fact that Smith was a very effective speaker who could be engaging and charismatic; thereby, presumably he was effective before a jury.3
Despite awareness of these problems by others, the report stressed that the chief forensic pathologist had a limited role in oversight of individual pathologists. Therefore, there was an absence of a mechanism for providing feedback to correct faults in pathologists. While there were three separate complaints regarding Smith to The College of Physicians and Surgeons of Ontario (CPSO), the licensing body for physicians in Ontario, the investigation and discipline process leading to a verdict and sanctions can be lengthy. On February 1, 2011, the Discipline Committee of the College of Physicians and Surgeons of Ontario found that:
In his practice of forensic pediatric pathology and his work providing expert opinion evidence in relation thereto, Dr. Charles Smith committed acts of professional misconduct, in that he failed to maintain the standard of practice of the profession in Ontario, engaged in disgraceful, dishonourable or unprofessional conduct, and is incompetent [Ref. 6, p 1].
Restoring Confidence in Pediatric Forensic Pathology
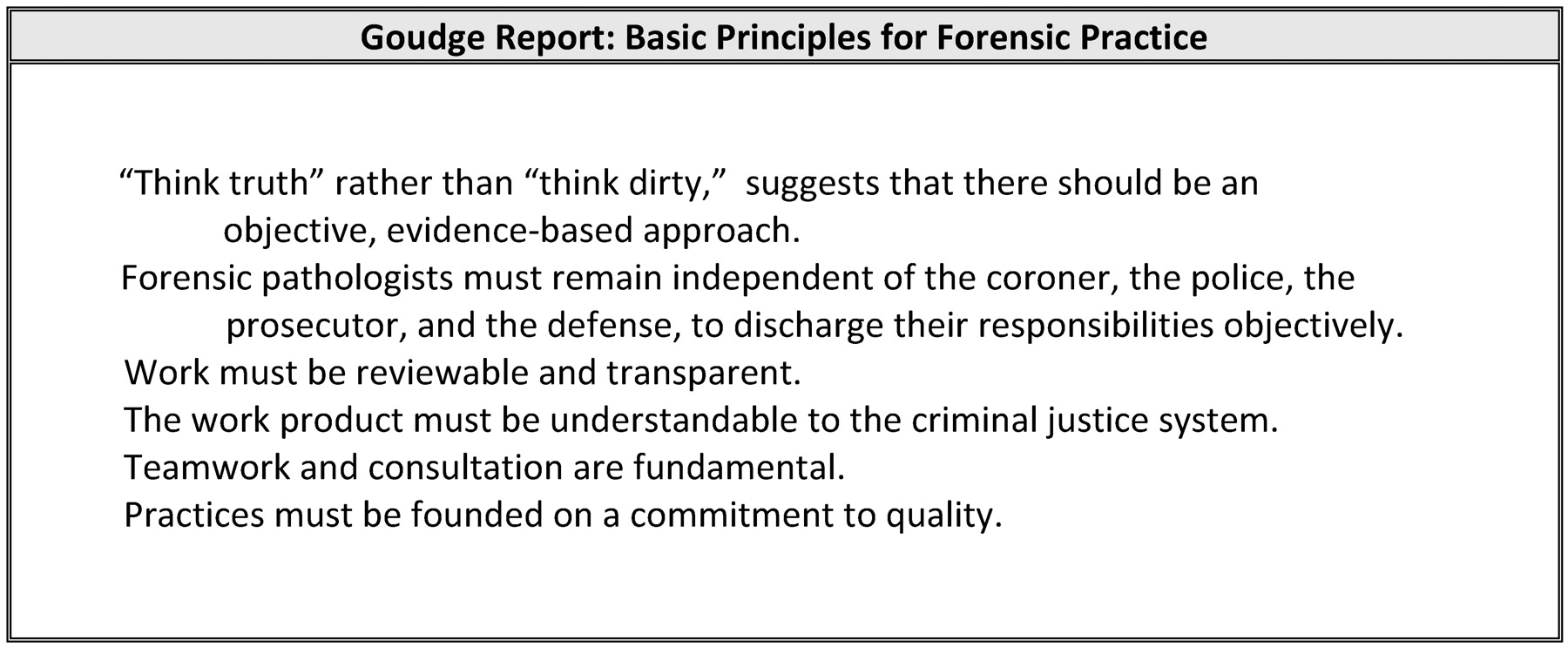
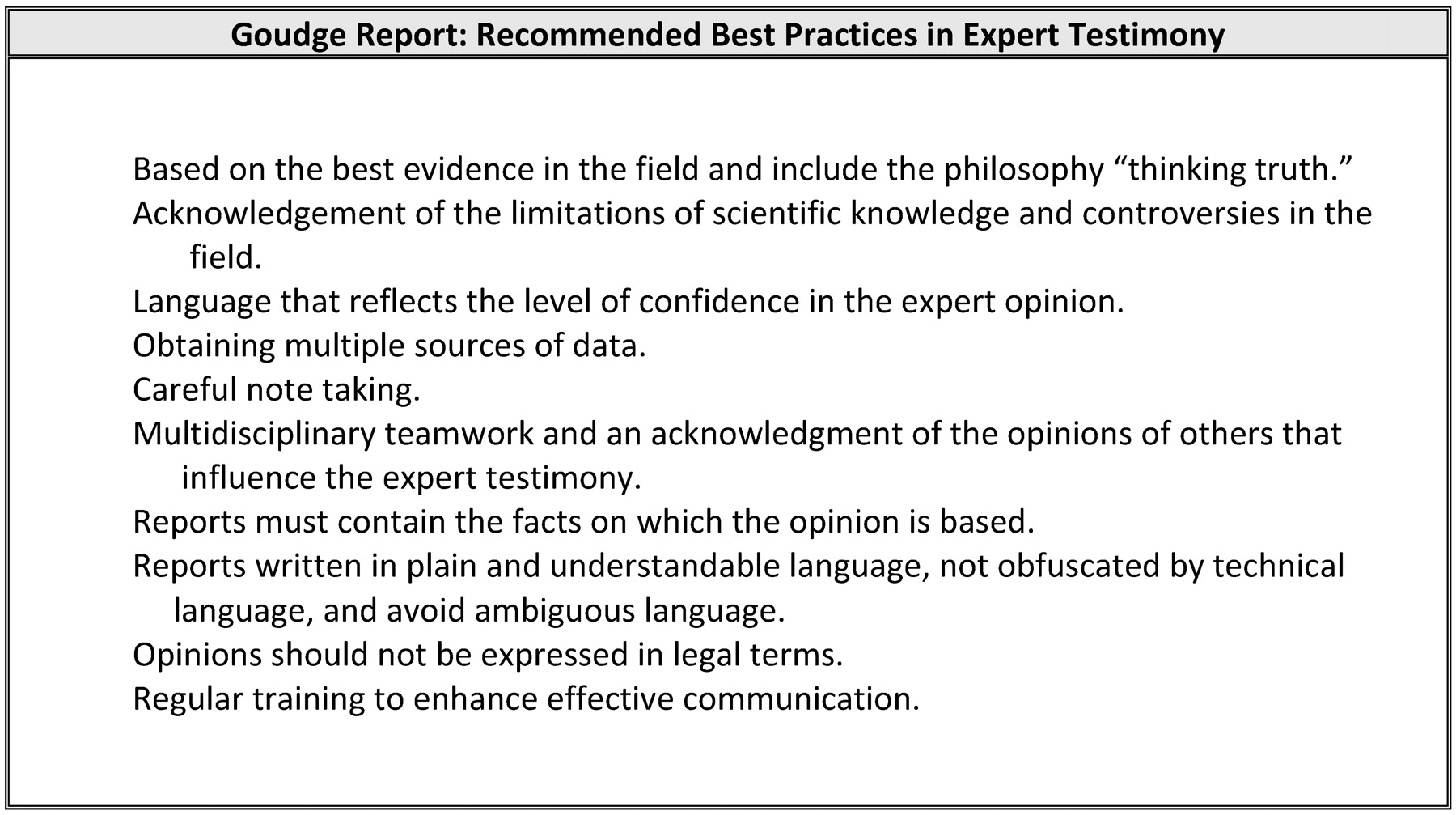
The final report of the Goudge Inquiry made a series of recommendations for systemic changes to the field of forensic pathology (Fig. 1). The report further outlined basic principles for forensic practice (Fig. 2) and suggested best practices (Fig. 3).

Inquiry recommendations.
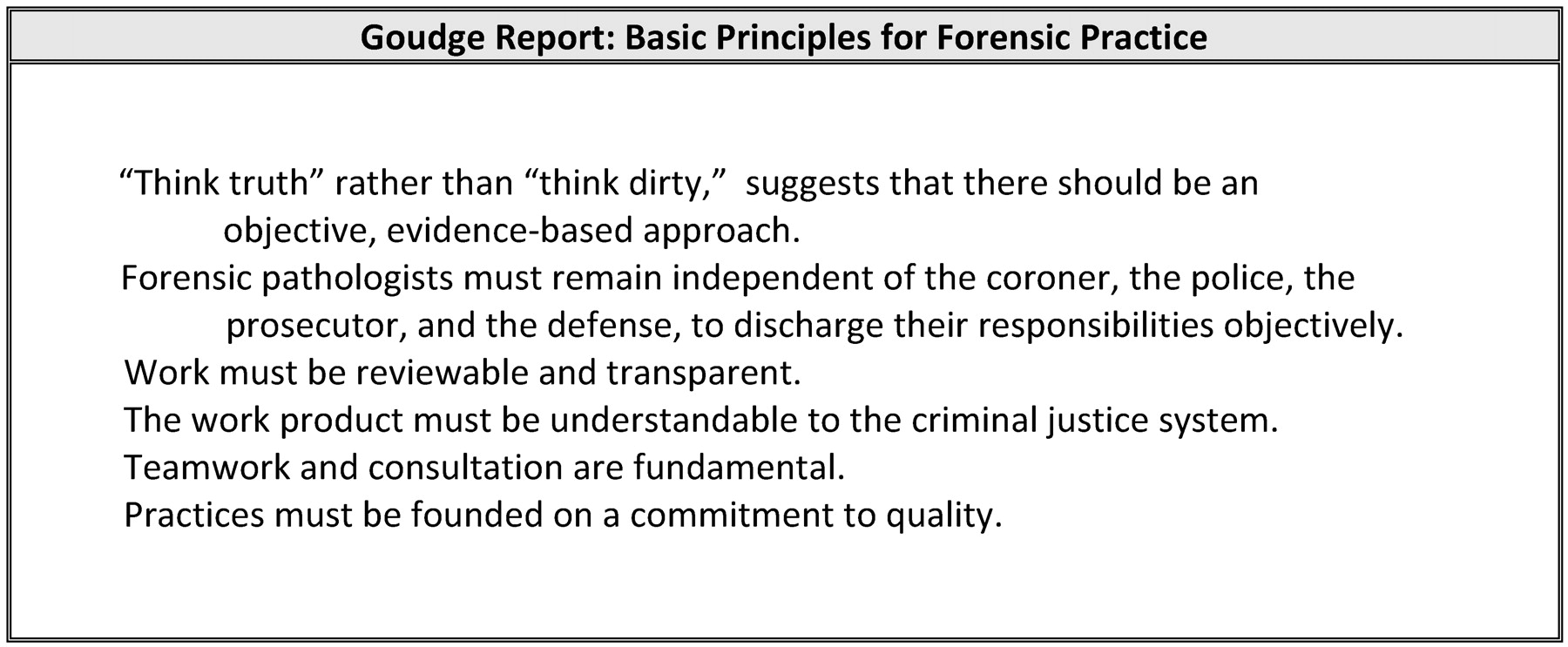
Basic principles for forensic practice.
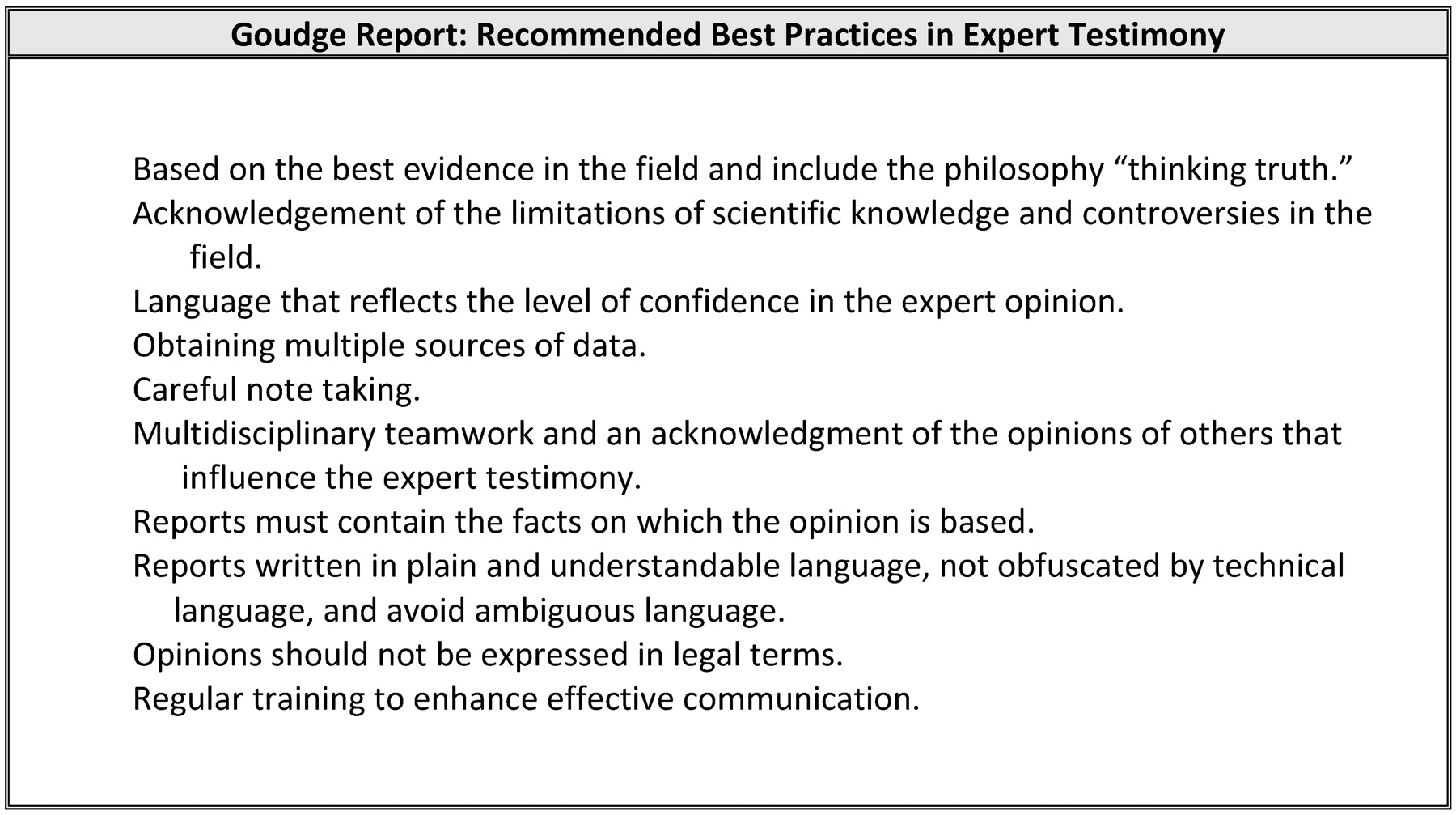
Recommended best practices.
Subspecialization
The Goudge Inquiry report strongly recommended that the Royal College of Physicians and Surgeons recognize pediatric forensic pathology as a subspecialty. This would provide a mechanism for accreditation of approved training systems. They also suggested mechanisms for increased recruitment in this subspecialty and recommended that the subspecialty should develop guidelines and practices based on the basic principles in Figure 2.
Evidentiary Basis for Expert Opinion
It was recommended in the Goudge Inquiry report that counsel prepare experts to give testimony and disclose fully anticipated opinions. The commissioner emphasized the role of the judge as the gatekeeper, in particular with reference to the reliability of a witness. In addition to this, the inquiry report paraphrased the principles enunciated in Daubert v. Merrell-Dow Pharmaceuticals, Inc.7,8 Legal definitions regarding expertise and competent practice have changed dramatically in recent years. Since 1923, the standard for expertise in the courts in the United States (and by default, in Canada) has been based on the concept of general acceptance,9 that is, is the method of treatment “generally accepted” by members of the profession. The 1993 U.S. Supreme Court ruling in Daubert was an important case regarding the admissibility of expert evidence. The Court cited four additional factors for assessing whether a particular test has a reliable foundation: whether the theory or technique can be and has been tested; whether the theory or technique has been subjected to peer review and publication; whether the error or potential rate of error had been identified; whether standards have been established; and whether this theory or technique is generally accepted. In 2000, the Supreme Court of Canada explicitly adopted the criteria in Daubert in the case of R v. J.(J.-L.).10
The Goudge Inquiry used these factors to outline a role for judges with respect to the evidentiary basis for expert opinion. The report recommended that judges carefully examine the reliability of the theory or technique that underlies expert testimony and whether it is generally accepted, is peer reviewed, and meets professional standards. It was noted that the judge should also seek evidence as to whether a theory or technique has been scientifically tested and whether there is serious dispute about the science. Evidence should also be garnered about alternative theories or interpretation. The report suggested that experts be allowed to give evidence only in language that is appropriate to the degree of controversy that exists in the field.
Despite the guidelines offered in both Daubert and the Goudge Inquiry, several publications have cautioned that there continues to be considerable risk, particularly in the area of mental health. In large part, the risk arises because the Court in Daubert did not give explicit guidance as to how stringently each of the four identified criteria should be applied.11 Grove and Barden12 argued that general acceptance is too frequently based on the assertion of the experts, as opposed to documented evidence. Levine13 cautioned that there is a false assumption that expert opinion in mental health is objective or impartial, unaffected by the adversarial process. Bonnie and Slobogin further asserted: “We are troubled by the poor quality of much clinical testimony which seems to rely more heavily on the assertion of Aesculapian authority than proven expertise” (Ref. 14, p 495). Clearly all disciplines, including psychiatry, must continue to develop scientific knowledge and consensus guidelines regarding best practices. In psychiatry, this includes, for example, establishing the reliability and validity of diagnostic categories.12
Development of Best Practices in the Field
The Goudge Inquiry report recommended best practices in the field of forensic pathology, many of which have direct relevance to forensic psychiatry. These recommendations focus on the evidence that underlies the expert opinion. They include both the collection of evidence from multiple sources and the acknowledgment of the limitations of the evidence and the manner in which the limitations affect the confidence that should be placed in the opinion. The recommendations also focus on the manner in which the expert expresses an opinion—for example, using understandable language that is not overly reliant on technical medical jargon. The report recommended that experts refrain from using legal language that directly addresses the ultimate issue and therefore usurps the role of the trier of fact. This is a contentious matter, as some judges may direct witnesses to address the ultimate issue, and in some jurisdictions psychiatrists are explicitly mandated to do so.
Oversight
Finally, the Goudge Inquiry made recommendations for the oversight of forensic pathology. It recommended that the attorney general develop a way to communicate adverse judicial comments or other concerns to “the body” of forensic pathologists. It was unclear how these comments would be reported and to whom. A further question that arises is whether information about the competence of experts would be disclosable to opposing counsel in future trials.11 It is hard to envision how this would apply to forensic psychiatrists in terms of which governing body would collect the information and how it would be used.
Implications for Forensic Psychiatry
While the Goudge Inquiry report was initiated as a result of severe concerns about the conduct of a pediatric forensic pathologist and addressed its recommendations to the practice of forensic pathology, it becomes clear that these recommendations have significant implications for all forensic professions. Forensic psychiatry has not been immune to high-profile experts who have undermined public confidence through their testimony. The case of Dr. James Grigson provides a chilling example. In a 1988 New York Times article,15 Grigson is referred to as Dr. Death, Dr. Doom, and a menace to society as a result of his testimony in death penalty cases. Concerns about Grigson's testimony in various cases included assertions that he would predict behavior without interviewing or attempting to interview the defendant and that he frequently performed examinations without the knowledge of the defendant's lawyer. In 1995, he was expelled from the American Psychiatric Association.16 Clearly, there are compelling arguments to ensure competent practice in forensic psychiatry that are analogous to the suggestions made regarding pediatric forensic pathology.
Report Writing and Assessment
The Goudge Inquiry report recommends that assessments be multifaceted, including gathering information from a variety of sources (for instance, in the case of forensic pathologists, attending the death scene) and be based on multidisciplinary teamwork. This practice is common in forensic psychiatry, in that we frequently work with psychologists and social workers who bring their own special expertise to add to that of the psychiatrist. The report also suggests that evidence included in expert reports and testimony be clear and accessible to cross examination. To this end, the report discusses the practice of videotaping autopsies. The use of videotaping in forensic psychiatry is an area of controversy that requires further consideration and discussion. The report of the American Academy of Psychiatry and the Law (AAPL) Task Force on Videotaping was not prepared to commit to the question of whether it should be routine practice in forensic psychiatric interviews.17 Gutheil et al.18 debated whether videotaping should become the standard. These presenters noted that the accuracy and reproducibility of the work product are greatly increased with videotaping. However, there are practical expenses and inconveniences, as well as detrimental effects on rapport and the psychiatrist-patient relationship, to be taken into account. The use of videotaping is therefore still evolving in forensic psychiatry, and there is as yet no consensus on whether it is good practice.
The Goudge report included considerable discussion regarding accurate and factual report writing, including the use of appropriate language. For example, it suggested that the phrase “consistent with…” not be used and that the profession design a compendium of appropriate phrases and expressions that should be used. Developing guidelines for appropriate language for use in reports is the type of activity that organizations such as the American Academy of Psychiatry and the Law (AAPL) or the Canadian Academy of Psychiatry the Law (CAPL) could foreseeably undertake. These organizations have already taken the lead in another area addressed by the Inquiry: training in writing forensic reports. For example, AAPL, in addition to providing comprehensive training for forensic psychiatrists, has a Peer Review Committee that regularly reviews and comments on the products of its members in a collegial and constructive manner.
Preparation for Court
The inquiry stressed that it is important for experts to put their opinions in writing in a timely manner, so that the opposing counsel can consider the opinion and retain an expert if necessary. In addition, the inquiry report suggested that counsel prepare experts for giving testimony, to ensure that the testimony is delivered in an appropriate manner. Finally, where there are differences of opinion, it was suggested that the opposing experts meet to delineate areas of agreement and disagreement. While this may seem antithetical to the current practice in an adversarial system in North America, in the United Kingdom there is provision for the experts to meet and discuss the extent of the areas of agreement and disagreement and produce a document summarizing these points to the parties. Generally the parties set an agenda outlining the questions for the experts to resolve.19 Although it has, after some initial resistance, become the norm in the United Kingdom, it is not anticipated that this practice would be readily accepted in North America.
Expert Testimony
The Goudge Inquiry report emphasizes that experts not take an advocacy role in attempting to pursue a particular agenda. Where opinion evidence cannot meet the standards of scientific scrutiny, it is the contention of some authors that forensic experts have an ethics-based duty to refuse to testify.12 In forensic psychiatry, the ethics guidelines of both AAPL and CAPL clearly stress the need for objectivity and honesty in the conduct of practice. In the courtroom, such objectivity means conceding the limits of one's expertise and considering alternative theories and evidence.11 In addition, experts should inform the courts of the scientific basis of their evidence and current controversies in the field.13 Psychiatry, like any other evolving science, has had no shortage of controversy, including the debates surrounding recovered-memory syndrome, rape accommodation syndrome, and multiple personality disorder. Experts can thus assist the court by educating others about the difference between “good science and junk ” (Ref. 12, p 238). The Goudge Inquiry further suggested that experts define their level of confidence in their opinions.
Training and Oversight
During the inquiry, Smith admitted that his training had been inadequate for the tasks that he had been asked to perform and that he had not taken advantage of any continuing medical education to upgrade his skills and knowledge.3 Organizations such as AAPL and CAPL have provided excellent educational opportunities for forensic psychiatrists of all levels of expertise. It is incumbent on all individual practitioners to take advantage of these opportunities and ensure that they are up to date on developments in the field and changes in the law pertaining to their practice. In addition, subspecialization in forensic psychiatry has led to the establishment and accreditation of fellowship programs in the United States and England and in the near future, Canada. Professional licensing bodies also carry a responsibility for investigating allegations of unprofessional conduct and an adherence to a reasonable standard of care to ensure public safety. If forensic professionals are not self-monitoring, others will step in to fill the void.
Conclusions
The case of Dr. Charles Smith is a chilling reminder of the perils of forensic practice. There is risk to the individual forensic practitioner if he or she does not appropriately exercise professional responsibility. The reputation of a specific forensic profession is imperiled when one of their members is accused of gross professional misconduct or incompetence. The loss of public confidence is highlighted in the framing of the Goudge Inquiry report, the stated purpose of which was to restore it. Finally and most important, when the profession does not adequately train, guide, and police its members, it might put the administration of justice at risk. While we may take comfort in the fact that the Goudge Inquiry focused on the failings of another forensic profession, we should take it as a warning to evaluate our own practices critically, to ensure that none of us will be the focus of a future inquiry.
Footnotes
Disclosures of financial or other potential conflicts of interest: None.
- © 2012 American Academy of Psychiatry and the Law





{kind=link}
{kind=link}
{kind=link}